Development of kidney
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
Excellent - I have all the content and diagrams I need. Let me now compile the comprehensive answer.
Development of the Kidney
The kidney develops through three successive, overlapping systems - all derived from intermediate mesoderm - that appear in a cranial-to-caudal sequence: the pronephros, mesonephros, and metanephros. Only the last becomes the permanent kidney.
- Langman's Medical Embryology, p. 276
- Campbell-Walsh-Wein Urology, p. 445
Origin: Intermediate Mesoderm
As the embryo undergoes transverse folding, intermediate mesoderm separates from the paraxial mesoderm and migrates ventrally to the dorsal wall of the intraembryonic coelom. It forms bilateral longitudinal masses called nephrogenic cords, which bulge from the posterior wall as the urogenital ridges. The gonadal ridge lies on the medial aspect of this ridge.
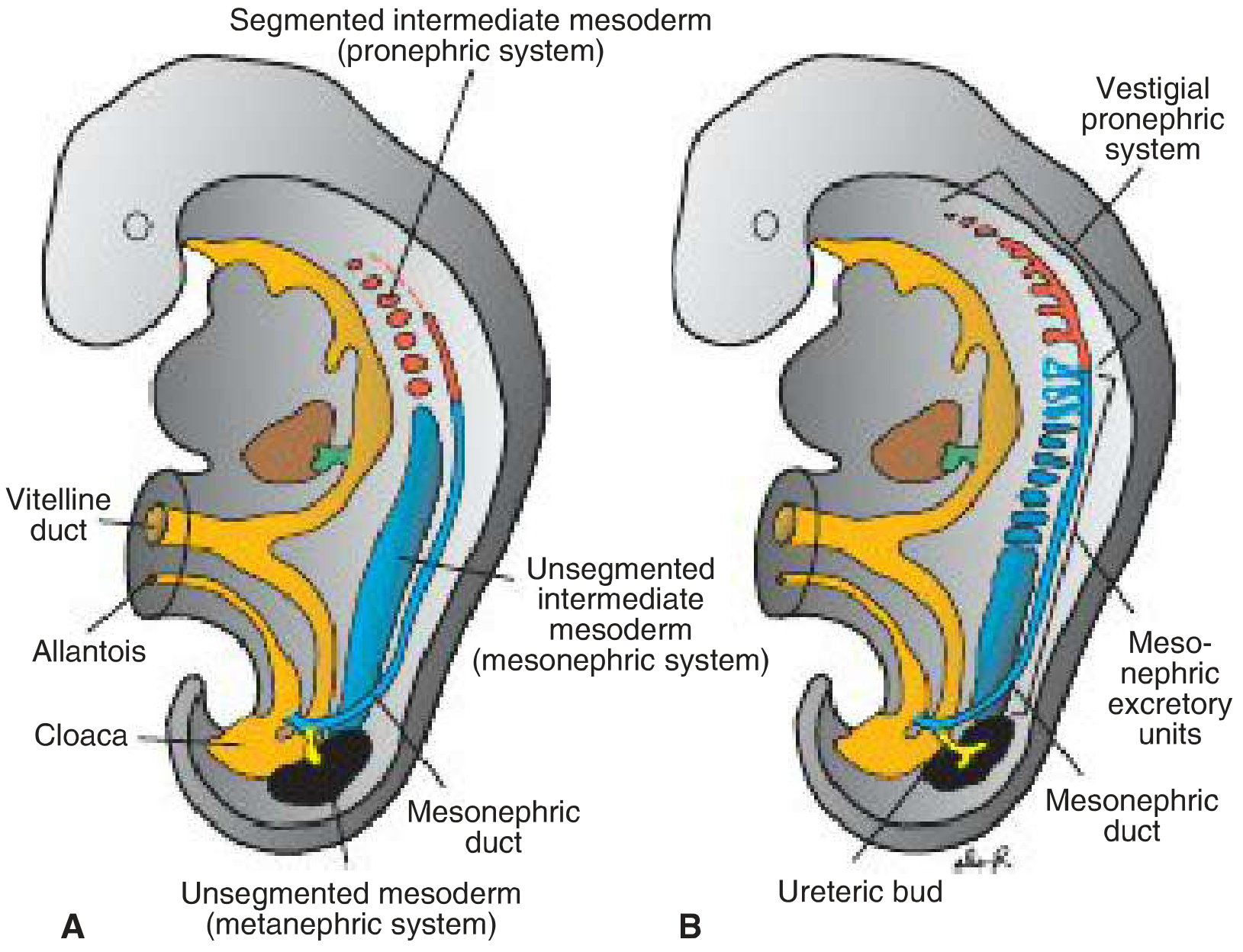
FIGURE: Relationship of the intermediate mesoderm of the three kidney systems. (A) Early, showing mesonephric duct. (B) Later, showing the ureteric bud growing from the mesonephric duct toward the metanephric mesoderm (blastema).
1. Pronephros (Week 4 - Non-functional)
- Appears at the beginning of week 4 in the cervical region
- Represented by 7-10 solid cell groups (nephrotomes) - vestigial excretory units
- Completely non-functional in humans (analogous to the kidney of primitive fish)
- Regresses completely by the end of week 4
- The pronephric duct is critical - it is retained and becomes the mesonephric (Wolffian) duct as development progresses caudally
2. Mesonephros (Weeks 4-8 - Transient functional kidney)
- Derived from intermediate mesoderm from upper thoracic to upper lumbar (L3) segments
- Appears in the early 4th week as the pronephros regresses
- Tubules lengthen, form S-shaped loops, and acquire a tuft of capillaries - forming glomeruli and Bowman capsule - creating renal corpuscles
- These tubules drain laterally into the mesonephric (Wolffian) duct, which drains into the cloaca
- By mid-second month, the mesonephros forms a large ovoid organ on each side of the midline
- Most tubules degenerate by end of the 2nd month
- Remnants in males persist to contribute to the genital system (rete testis, efferent ductules, epididymis, vas deferens, seminal vesicles)
- In females, nearly all mesonephric structures disappear
3. Metanephros - The Permanent Kidney (Week 5 onward)
Initiation
The metanephros appears in the 5th week and develops from two sources:
| Source | Gives rise to |
|---|---|
| Ureteric bud (outgrowth of mesonephric duct) | Collecting system: collecting ducts, calyces, renal pelvis, ureter |
| Metanephric mesoderm (blastema) | Excretory units: nephrons (glomerulus to distal convoluted tubule) |
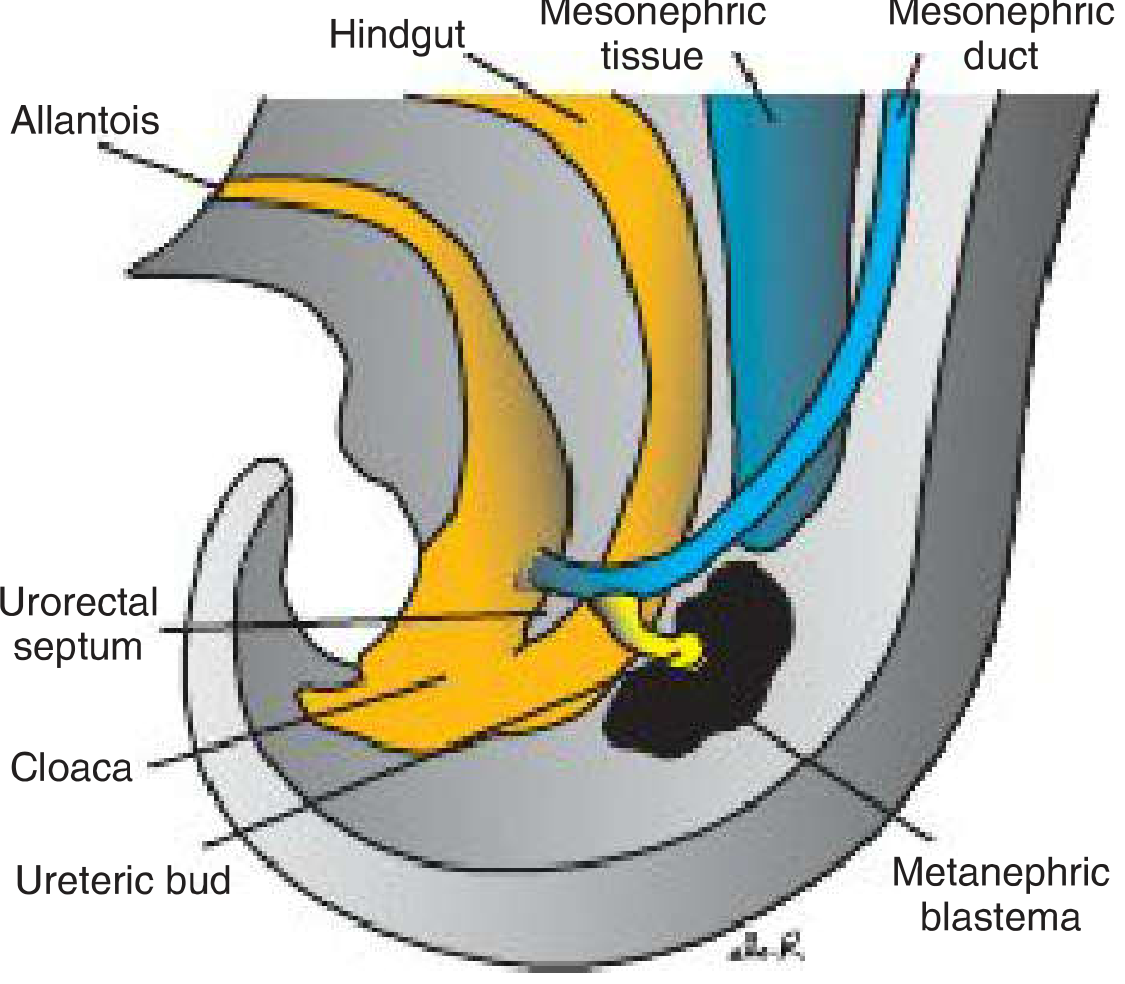
FIGURE: The ureteric bud sprouts from the mesonephric duct near its entrance into the cloaca and penetrates the metanephric mesoderm (blastema).
Collecting System Development (from the Ureteric Bud)
The ureteric bud:
- Sprouts from the caudal mesonephric duct near the cloaca at ~4-5 weeks
- Penetrates the metanephric tissue, which caps its distal end
- Dilates to form the primitive renal pelvis
- Splits into cranial and caudal portions - the future major calyces
- Each major calyx buds into minor calyces, which continue to subdivide until 12 or more generations of tubules form
- Peripheral tubule generation continues until the end of the 5th month
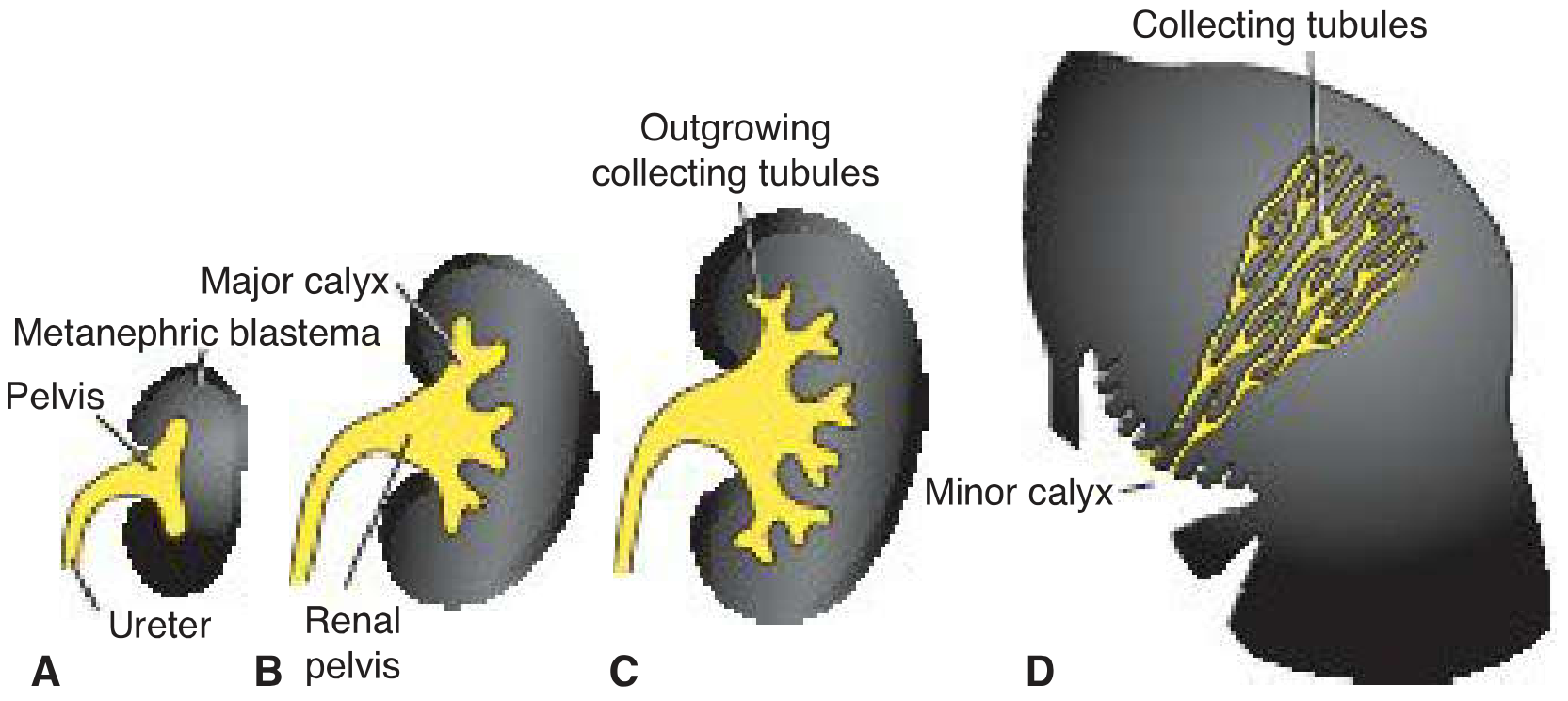
FIGURE: Development of the renal collecting system. (A) 6 weeks - primitive pelvis with major calyces. (B) End of 6th week. (C) 7 weeks. (D) Newborn - pyramid form of collecting tubules entering minor calyces.
Nephron Formation (from Metanephric Mesenchyme)
The ureteric bud's tip (the ampulla) induces the metanephric mesenchyme to:
- Condense around the ampulla as a cap
- Undergo mesenchymal-to-epithelial transition - forming renal vesicles
- Renal vesicles elongate into S-shaped tubules
- Capillaries grow into one end of the S, differentiating into glomeruli
- The tubule elongates to form: Bowman capsule → proximal convoluted tubule → loop of Henle → distal convoluted tubule
- The distal end of each tubule forms an open connection with a collecting tubule from the ureteric bud, establishing continuity from Bowman capsule to the collecting duct system
Key fact: Nephron formation continues until birth, at which time there are approximately 1 million nephrons per kidney. No new nephrons form after birth.
Urine production begins at week 12 following differentiation of glomerular capillaries (which form by week 10).
Reciprocal Inductive Signaling - The Molecular Basis
The ureteric bud and metanephric mesenchyme exert reciprocal inductive effects on each other. Without these signals, the kidney does not develop.
Mesenchyme → Ureteric Bud signals:
- WT1 (Wilms Tumor 1): transcription factor expressed by mesenchyme that makes it competent to respond to ureteric bud induction; also regulates GDNF and HGF production
- GDNF (Glial cell line-Derived Neurotrophic Factor): secreted by metanephric mesenchyme; activates the RET receptor tyrosine kinase on the mesonephric duct/ureteric bud, driving ureteric bud outgrowth and branching
- HGF (Hepatocyte Growth Factor / scatter factor): activates MET receptor on the ureteric bud epithelium
- The GDNF-RET-GFRα1 pathway is the most critical - knockout of any of these three genes in mice causes failure of ureteric bud outgrowth and renal agenesis
Ureteric Bud → Mesenchyme signals:
- FGF2 and BMP7: secreted by ureteric bud; block apoptosis, stimulate proliferation in metanephric mesenchyme, and maintain WT1 expression
- WNT9B and WNT6: secreted by branches of the ureteric bud epithelium; upregulate PAX2 and WNT4 in surrounding mesenchyme
- WNT4 then causes mesenchymal-to-epithelial conversion to form nephrons
Nephric duct formation:
- The transcription factors LIM1, PAX2, and SIM1 are expressed in intermediate mesoderm destined to become nephric ducts
- LIM1 is absolutely essential for nephric duct formation; it activates PAX2 to orchestrate duct development
Position of the Kidney - Ascent
Initially, the metanephros forms in the sacral/pelvic region. It subsequently ascends to its definitive lumbar position:
- Ascent is caused by diminution of body curvature and growth in the lumbar and sacral regions (not by active migration)
- As it ascends, the kidney receives successive arterial branches from the aorta at progressively higher levels
- Lower vessels usually degenerate, but some may persist as accessory renal arteries (a common normal variant)
- Simultaneously, the kidney rotates 90° medially so the hilum faces anteromedially
Summary Timeline
| Week | Event |
|---|---|
| Week 3 (late) | Pronephros appears; begins degenerating |
| Week 4 (early) | Mesonephros tubules appear; mesonephric (Wolffian) duct forms |
| Week 4 (end) | Pronephros completely degenerated |
| Week 5 | Ureteric bud sprouts; metanephros development begins |
| Week 6-7 | Ureteric bud branches; renal pelvis and calyces form |
| Weeks 6-8 | Mesonephros degenerates (except genital remnants in males) |
| Week 10 | Glomerular capillaries begin forming |
| Week 12 | Urine production begins |
| Month 5 | Peripheral nephrogenesis complete |
| Birth | ~1 million nephrons per kidney; lobulated appearance |
| Infancy | Lobulations disappear due to nephron growth (no new nephrons form) |
Congenital Anomalies of Kidney Development
Renal Agenesis
- Bilateral: 1/10,000 births; results in Potter sequence - anuria, oligohydramnios, hypoplastic lungs, Potter facies (flattened face), and club feet
- Due to failure of ureteric bud-metanephric mesenchyme interaction, or mutations in genes regulating this (SALL1 in Townes-Brock syndrome; PAX2 in renal coloboma syndrome; EYA1 in branchiootorenal syndrome)
Horseshoe Kidney
- The lower poles of the kidneys fuse across the midline during ascent; the fused mass gets caught on the inferior mesenteric artery and cannot ascend further
- Results in a kidney located at approximately L3-L5
Polycystic Kidney Disease
- ARPKD (1/5,000): autosomal recessive; cysts from collecting ducts; renal failure in infancy/childhood
- ADPKD (1/500-1/1,000): autosomal dominant; cysts from all nephron segments; renal failure in adulthood
- Both are ciliopathies - caused by mutations in cilia-related proteins; related conditions include Bardet-Biedl syndrome and Meckel-Gruber syndrome
Wilms Tumor (Nephroblastoma)
- Cancer arising from remnant metanephric blastema; peaks before age 5
- Due to mutations in WT1 gene (chromosome 11p13)
- WAGR syndrome: Wilms tumor + Aniridia + Gonadoblastoma + mental Retardation - caused by microdeletion of 11p13 including both WT1 and PAX6 genes
- Denys-Drash syndrome: Wilms tumor + renal failure + ambiguous genitalia
Duplex Collecting System
- Results from early splitting of the ureteric bud - partial or complete duplication of the ureter
- One ureter may open ectopically into the vagina, urethra, or vestibule (in females, causing continuous dribbling of urine)
Sources:
- Langman's Medical Embryology, pp. 275-283 - Three kidney systems, collecting system, nephron formation, molecular regulation, positional changes, clinical correlates
- Campbell-Walsh-Wein Urology, pp. 444-450 - Early events, metanephros, reciprocal inductive signals, molecular mechanisms
- National Kidney Foundation Primer on Kidney Diseases, 8e - Overview and maturation
This is a shared conversation. Sign in to Orris to start your own chat.