Agglutination test in micro
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Now I have comprehensive information to provide a thorough answer. Let me compile everything.
Agglutination Tests in Microbiology
Basic Principle
Agglutination is the visible clumping of particulate antigens (bacteria, RBCs, latex beads) when cross-linked by specific antibodies. Antibody molecules act as bridges between antigen-carrying particles, forming a lattice that precipitates as macroscopically visible aggregates.
- IgM antibodies are far more efficient at producing complete agglutination than IgG due to their larger size and higher valence (10 binding sites).
- When only IgG is involved, enhancement is needed (e.g., lowering ionic strength, adding polymerized albumin, dextran, or PEG).
- The zeta potential (net negative charge on RBCs/bacteria) creates mutual repulsion that must be overcome for agglutination to occur.
- Antigen-to-antibody ratio is critical: extreme excess of either inhibits aggregation (the prozone/hook effect).
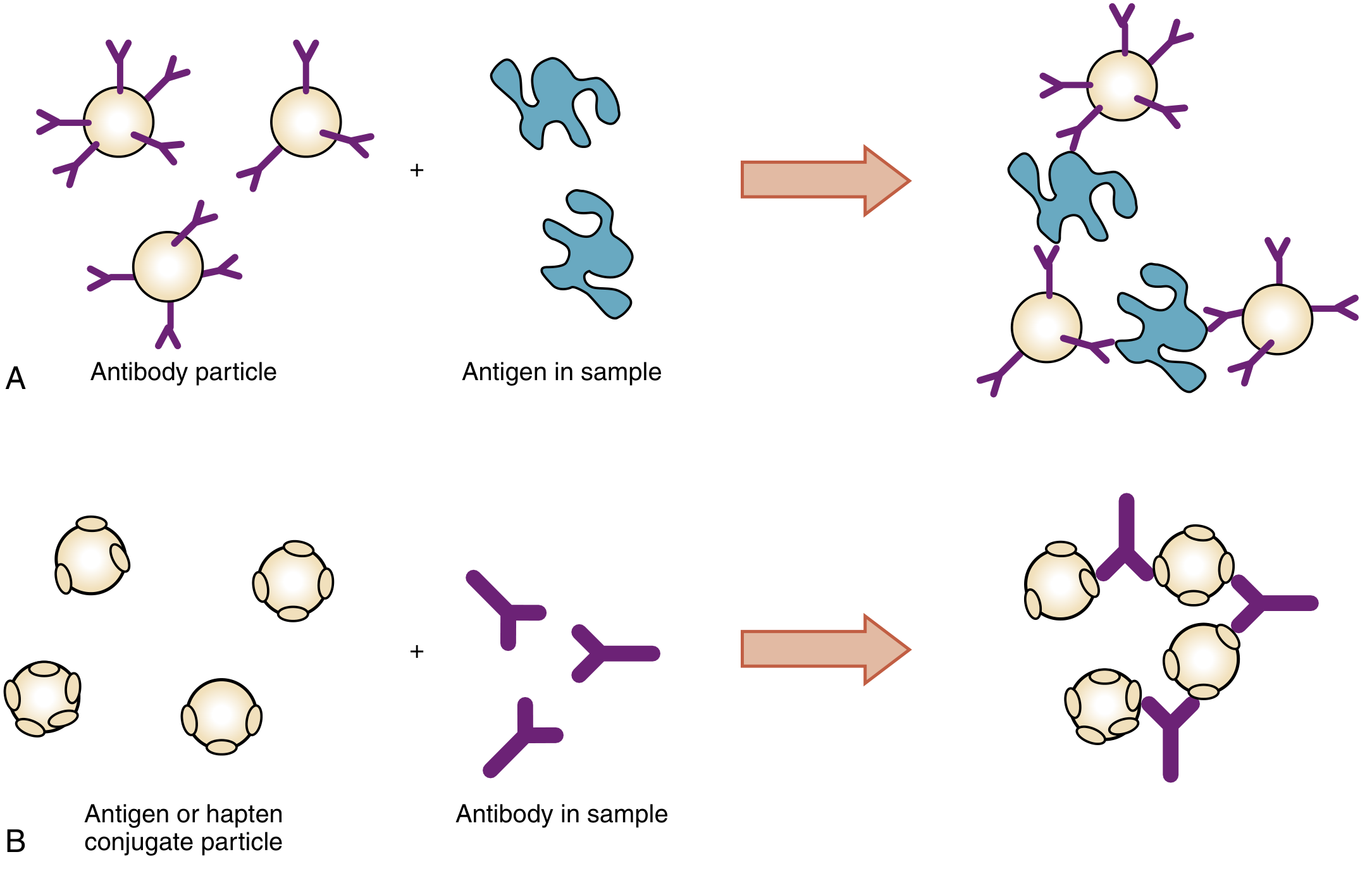
Principles of passive particle agglutination: (A) reverse agglutination - antibody-coated particle detects antigen; (B) passive agglutination - antigen-coated particle detects antibody - Henry's Clinical Diagnosis and Management by Laboratory Methods
Types of Agglutination Tests
1. Direct (Active) Agglutination
The natural surface antigens of a particulate agent (whole bacteria or RBCs) react directly with antibodies in the patient's serum. No prior sensitization of the particle is needed.
Examples:
- Widal test - patient serum is serially diluted and tested against Salmonella O (somatic) and H (flagellar) antigens. A single O antigen titer >1:320 and H antigen titer >1:640 is considered positive. Requires two specimens 7-10 days apart to show a rising titer. - Jawetz Medical Microbiology
- Weil-Felix test - cross-reacting antibodies from Rickettsia infections agglutinate Proteus OX-19 strains.
- Blood grouping (ABO/Rh typing) - direct testing of erythrocytes with known antisera (anti-A, anti-B, anti-D).
2. Indirect (Passive) Agglutination
Soluble antigens are artificially adsorbed or covalently coupled onto a particle carrier (RBCs, latex, gelatin, bentonite). Patient antibody then cross-links these sensitized particles.
Examples:
- TPHA (Treponema pallidum hemagglutination assay) - T. pallidum antigens coated onto fixed sheep RBCs; detects syphilis antibodies.
- HIV antibody detection - sensitized human or avian erythrocytes.
- Passive latex agglutination - soluble antigens coated on latex beads; antibody in specimen agglutinates them.
3. Reverse Passive Agglutination
Here the antibody is fixed to the particle, and the test detects soluble antigen in the specimen.
Examples:
- Latex agglutination for cryptococcal antigen - antibody-coated latex beads agglutinate in the presence of Cryptococcus neoformans polysaccharide antigen in CSF or serum (sensitivity 60-95%).
- Detection of HBsAg - reverse passive hemagglutination.
- Lancefield typing of beta-hemolytic streptococci - latex beads coated with type-specific antibodies agglutinate when exposed to streptococcal group antigens.
- Group A Strep antigen detection (pharyngitis rapid testing).
4. Agglutination Inhibition
A competitive technique for detecting small antigens (haptens) that cannot cross-link particles themselves.
- Principle: A fixed amount of antibody is mixed with the test specimen. If antigen (hapten) is present in the specimen, it occupies the antibody. When the antibody-laden specimen is then mixed with hapten-coated particles, no agglutination occurs - inhibition = positive test.
- Classic example: Pregnancy test (latex agglutination inhibition for hCG) - if hCG is present in urine, it blocks anti-hCG antibody from agglutinating hCG-coated latex beads.
- Also used to identify specific viral hemagglutinins (hemagglutination inhibition test for influenza).
5. Coagglutination
Similar to latex agglutination, but uses Staphylococcus aureus (Cowan I strain) - rich in Protein A - as the carrier particle instead of latex. Protein A binds the Fc region of IgG, leaving the Fab arms free to react with antigen.
Uses:
- Identification of bacterial cultures: Streptococcus pneumoniae, Neisseria meningitidis, N. gonorrhoeae, beta-hemolytic streptococci.
- Less useful for direct antigen detection in specimens compared to latex agglutination.
- Jawetz Medical Microbiology, 28E
6. Hemagglutination and Hemagglutination Inhibition (HI Test)
- Certain viruses (influenza, measles, mumps, rubella, adenoviruses) directly agglutinate RBCs via viral surface proteins (hemagglutinins).
- Hemagglutination Inhibition (HI): Patient antibodies block viral hemagglutinin, preventing RBC agglutination. Inhibition = positive (antibody present). Widely used for serological diagnosis of viral infections and antibody titering.
7. Heterophile Agglutination
Antibodies from one species react with antigens of an unrelated species.
- Paul-Bunnell test / Monospot test: EBV (infectious mononucleosis) induces heterophile antibodies that agglutinate sheep RBCs (Paul-Bunnell) or horse RBCs (Monospot). The monospot test is ~75% sensitive, ~90% specific.
- Scott-Brown's Otorhinolaryngology; Henry's Clinical Diagnosis and Management
Particles Used as Carriers (Summary Table)
| Particle | Method | Key Applications |
|---|---|---|
| Human erythrocytes | Direct hemagglutination | ABO blood typing, HIV antibody |
| Fixed animal erythrocytes | Passive hemagglutination | T. pallidum antibody (TPHA), HBsAg |
| Latex | Reverse passive agglutination | CRP, cryptococcal Ag, Strep Ag, RF |
| Latex (colored) | Immunochromatography | hCG (pregnancy test) |
| Gelatin particles | Passive agglutination | HIV antibody, T. pallidum |
| Staphylococci (Protein A) | Coagglutination | Strep, Neisseria typing |
| Bentonite | Passive agglutination | Trichinella antibody |
Henry's Clinical Diagnosis, Table 45.2
Important Concepts
Prozone Phenomenon (Hook Effect)
When antibody concentration is very high relative to antigen, each antibody molecule binds antigen but cannot form cross-linking lattices, resulting in a falsely negative agglutination test. The solution is to dilute the serum further. This is classically seen with cryptococcal antigen testing and in syphilis serology.
Incomplete Agglutination
Primary antigen-antibody reaction occurs but no visible aggregation results - commonly with IgG antibodies due to insufficient bridging distance to overcome the zeta potential of RBCs. Detected by the Coombs/Antiglobulin test (add anti-human IgG which bridges the IgG-coated cells).
Grading of Agglutination
- 4+: One large clump, clear background
- 3+: Several large clumps, clear background
- 2+: Many medium clumps
- 1+: Small clumps, turbid background
- m+ (microscopic): Visible only under microscope
- Negative: No clumping, smooth suspension
Key Clinical Applications in Microbiology
| Test | Organism/Disease | Type |
|---|---|---|
| Widal test | Enteric fever (Salmonella Typhi) | Direct tube agglutination |
| Weil-Felix test | Rickettsia spp. | Direct (cross-reacting) |
| TPHA | Syphilis (T. pallidum) | Passive hemagglutination |
| Latex agglutination | Cryptococcal meningitis, Strep, meningitis | Reverse passive |
| Monospot/Paul-Bunnell | Infectious mononucleosis (EBV) | Heterophile |
| Blood grouping | ABO/Rh compatibility | Direct |
| HI test | Influenza, rubella, measles | Hemagglutination inhibition |
| Coagglutination | Strep, Neisseria identification | Coagglutination |
| Pregnancy test (latex) | hCG detection | Agglutination inhibition |
Sources: Jawetz, Melnick & Adelberg's Medical Microbiology 28E | Henry's Clinical Diagnosis and Management by Laboratory Methods | Tietz Textbook of Laboratory Medicine 7E | Sherris & Ryan's Medical Microbiology 8E
This is a shared conversation. Sign in to Orris to start your own chat.