How to effectively manage and treat hemorrhagic CVA in ER and ward with limited resources also in best possible sceniorus , how to monitor the patient .. how to decide prognosis .. give mnemonics wherever possible
Reading File
Finding Sources
Finding Sources
Searching PubMed
"intracerebral hemorrhage" management guidelines
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Searching the Web
hemorrhagic stroke management limited resources low income settings 2024 guidelines
Loading Image
I now have comprehensive data from multiple authoritative sources. Let me compile the full, detailed answer.
Hemorrhagic CVA (Intracerebral Hemorrhage): Complete Clinical Management Guide
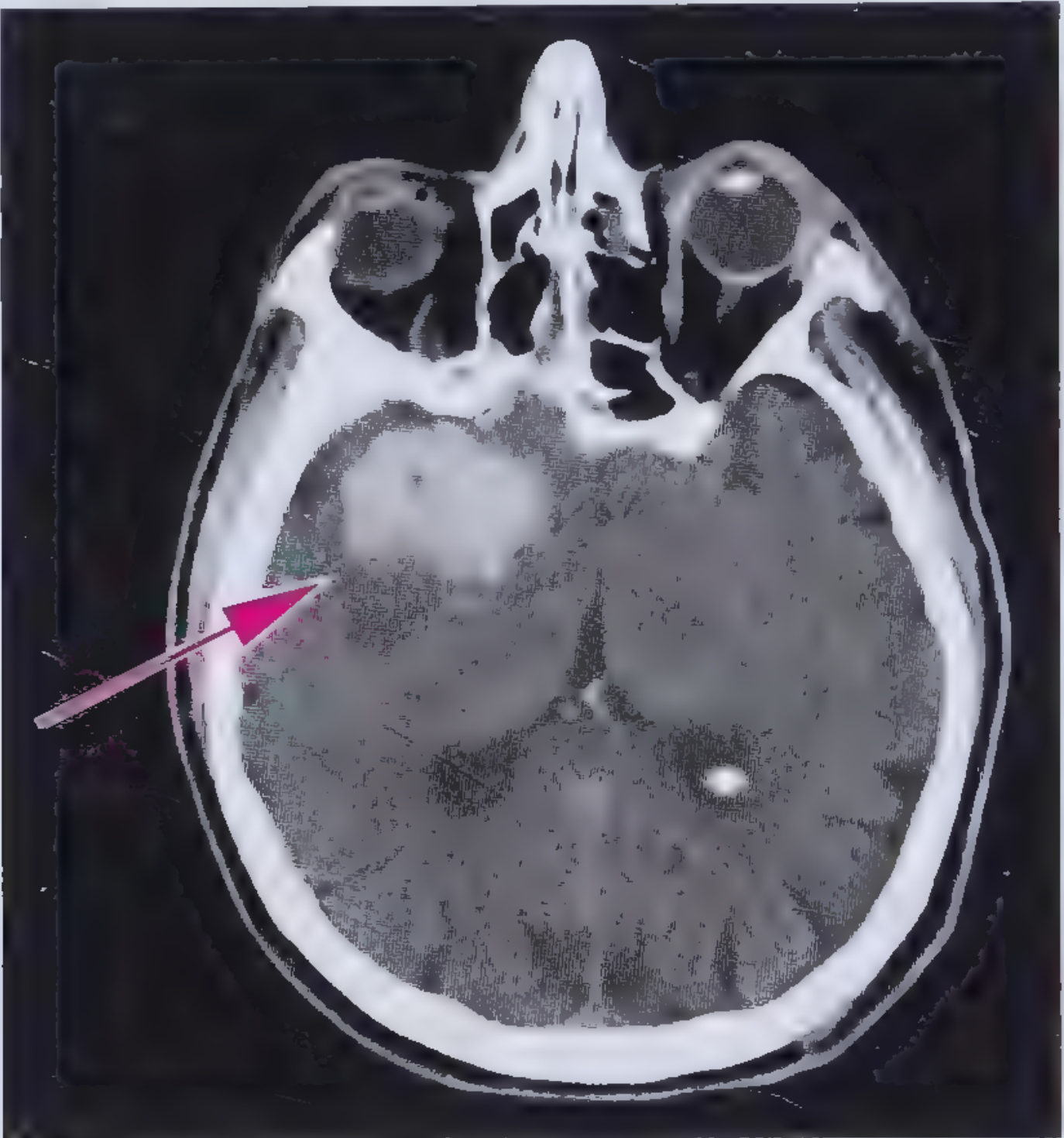
Noncontrast CT: Hyperdense (40-100 HU) round/oval lesion = ICH. CT is the first-line imaging in any ER.
Quick Orientation: Why ICH is Different
Hemorrhagic stroke = ~15% of all strokes, but carries 30-day mortality ~50%, 1-year mortality ~55%. Management is completely different from ischemic stroke - no thrombolytics, and aggressive blood pressure control is the cornerstone. - Tintinalli's Emergency Medicine, p.1156
PART 1: IMMEDIATE ER ASSESSMENT
Mnemonic: "ABCDE-STROKE" (First 10 minutes)
| Letter | Action |
|---|---|
| A | Airway - secure if GCS ≤8 or deteriorating |
| B | Breathing - O2 only if SpO2 <94% (no routine O2) |
| C | Circulation - IV access x2, cardiac monitor |
| D | Disability - GCS, pupils, focal deficits, NIHSS |
| E | Exposure/Extras - glucose, temperature, BP both arms |
| S | Sugar (glucose) - target 140-180 mg/dL |
| T | Temperature - treat fever aggressively |
| R | Reverse coagulopathy - check INR, platelets |
| O | O2 sats continuous monitoring |
| K | Keep head of bed at 30 degrees |
| E | Emergency CT head (noncontrast) IMMEDIATELY |
PART 2: DIAGNOSIS
CT Findings to Know
| Time After Bleed | Appearance | HU |
|---|---|---|
| Acute (hours) | Heterogeneous hyperdense | 40-60 |
| Hours to days | Homogenous, hyperdense | 60-80 |
| Days | Very bright, well-defined | 80-100 |
Minimum workup (even in limited settings):
- Noncontrast CT head (mandatory - cannot distinguish ICH from ischemic clinically)
- Glucose (bedside)
- CBC, PT/INR, aPTT
- BMP/electrolytes, renal function
- ECG (arrhythmias common)
If resources allow:
- CT angiography (CTA): if age <45, no known hypertension, no obvious cause - look for AVM, aneurysm
- MRI with GRE/SWI: superior for underlying structural lesions
Clinical tip: Headache + nausea + vomiting preceding focal deficit + rapid deterioration = ICH until proven otherwise. BUT you cannot diagnose clinically - CT is mandatory. - Tintinalli's, p.1159
PART 3: ER MANAGEMENT - THE "FAST-RICH" MNEMONIC
FAST-RICH = Core ICH ER Management
| Letter | Action |
|---|---|
| F | Fever - treat with paracetamol, target normothermia |
| A | Airway - intubate if GCS ≤8 (RSI, avoid coughing/Valsalva) |
| S | Sugar - tight glucose control 140-180 mg/dL |
| T | Temperature monitoring q4h |
| R | Reverse coagulopathy (see below) |
| I | ICP - manage elevated intracranial pressure |
| C | Control blood pressure (see BP table below) |
| H | Head elevated 30°, prevent aspiration |
PART 4: BLOOD PRESSURE MANAGEMENT
The Key BP Target Table
| Situation | Target | Action |
|---|---|---|
| SBP 150-220 mmHg | 140 mmHg | Safe to lower acutely - improves functional outcome |
| SBP >220 mmHg | Reduce aggressively | Continuous IV infusion |
| SBP <110 mmHg | Maintain - don't lower | May worsen ischemic penumbra |
Important: The ATACH-2 trial showed targeting SBP 110-139 mmHg did NOT improve outcomes vs. 140-179 mmHg, so aggressive reduction below 140 is not indicated. - Tintinalli's, p.1159
Antihypertensive Drugs for ICH (IV preferred)
| Drug | Dose | Notes |
|---|---|---|
| Labetalol | 20-80 mg IV bolus q10min (max 300 mg) OR 0.5-2 mg/min infusion | First-line where available |
| Nicardipine | 5-15 mg/hr IV infusion | Preferred in many guidelines |
| Hydralazine | 10-20 mg IV q4-6h | Use in resource-limited settings |
| Enalaprilat | 1.25 mg IV q6h | Alternative in resource-limited settings |
Avoid: Sublingual nifedipine (unpredictable drop), nitroprusside (increases ICP).
PART 5: REVERSAL OF COAGULOPATHY
Mnemonic: "WARP" (Warfarin/Anticoagulant Reversal Protocol)
| Anticoagulant | Reversal |
|---|---|
| Warfarin (elevated INR) | Vitamin K 10 mg IV slow + 4-factor PCC (preferred) or FFP 10-15 mL/kg |
| Aspirine/Antiplatelet | Platelet transfusion only if on antiplatelet AND going to surgery |
| Rivaroxaban/Apixaban (DOACs) | Andexanet alfa (if available); otherwise 4F-PCC |
| Praxbind (Dabigatran) | Idarucizumab (specific antidote); otherwise dialysis |
In limited resource settings: FFP remains the practical option for warfarin reversal when PCC unavailable. Target INR <1.4 before any procedure.
PART 6: ICP MANAGEMENT
Stepwise ICP Management - "OSLO" Protocol
| Step | Intervention | Notes |
|---|---|---|
| O | Optimize positioning | HOB 30°, head midline, avoid neck compression |
| S | Sedation/analgesia | Morphine or propofol to reduce agitation/Valsalva |
| L | Lower ICP medically | Mannitol 0.25-1 g/kg IV over 20 min OR 3% NaCl (hypertonic saline - preferred, doesn't cause rebound) |
| O | Osmotherapy | Repeat q6h guided by serum osmolality (target <320 mOsm/L for mannitol) |
IMPORTANT - Do NOT use:
- Corticosteroids (dexamethasone/steroids) - no benefit in ICH and increase infectious complications
- Routine hyperventilation (only as bridge to surgery, target pCO2 35-40 mmHg normally)
When to consider ICP monitor:
- GCS ≤8
- Intraventricular hemorrhage (IVH)
- Hydrocephalus on CT
- Target CPP: 50-70 mmHg - Plum & Posner's, p.571
PART 7: SEIZURE MANAGEMENT
- Prophylactic AEDs are NOT recommended routinely
- Treat clinical seizures immediately: IV Lorazepam 0.1 mg/kg → Phenytoin/Levetiracetam
- Consider EEG monitoring in patients who don't improve as expected (non-convulsive status epilepticus)
- Levetiracetam preferred over phenytoin (less drug interactions, no cardiac effects)
PART 8: SURGICAL INDICATIONS
Mnemonic: "CHOP" = When to Call Surgery
| Letter | Indication |
|---|---|
| C | Cerebellar hemorrhage ≥3 cm OR with brainstem compression/hydrocephalus = EMERGENCY surgery |
| H | Hydrocephalus - EVD (external ventricular drain) placement urgently |
| O | OccipitaL / any with rapidly declining GCS despite medical management |
| P | Progressive neurological deterioration not responding to medical therapy |
Supratentorial ICH - no proven benefit from routine craniotomy:
- Large RCTs (STICH I and II) showed no benefit for routine surgical evacuation of supratentorial ICH
- Exception: Superficial lobar hemorrhages <1 cm from cortical surface may benefit
- Novel: Minimally invasive surgery (MISTIE) shows some benefit but limited availability - Goldman-Cecil, p.3487; Miller's Anesthesia
PART 9: WARD MONITORING
Mnemonic: "MONITORS" - What to Track
| Letter | Parameter | Frequency |
|---|---|---|
| M | Mental status / GCS | Q1-2h for first 24h, then Q4h |
| O | O2 saturation | Continuous |
| N | Neurological deficits (pupils, limb power) | Q1-2h |
| I | IV infusion rates (BP meds) | Continuous |
| T | Temperature | Q4h |
| O | Output/Input (urine, fluids) | Hourly ICU, Q4h ward |
| R | Random blood glucose | Q4-6h |
| S | Serum electrolytes, osmolality | Daily (or q12h if on mannitol) |
Danger Signs - "HEADS UP" (Deterioration Alarm)
- H - Headache worsening
- E - Eyes - new anisocoria, gaze deviation
- A - Altered consciousness (GCS drop ≥2)
- D - Drooping - new facial/limb weakness
- S - Seizures (overt or subtle)
- U - Unequal pupils or Cushing's triad
- P - Pulse/BP change (Cushing's triad: HTN + bradycardia + irregular breathing = herniation)
Serial CT head: Repeat at 6-24 hours (hematoma expansion occurs in ~30% within 6 hours). If condition worsens at any time, repeat CT immediately.
PART 10: COMMON LOCATIONS AND THEIR CLINICAL FEATURES
| Location | Clinical Features | Key Concern |
|---|---|---|
| Putamen (most common, ~35%) | Contralateral hemi-paresis, hemisensory loss, dysphasia if dominant | Midline shift |
| Thalamus | Sensory > motor, gaze palsies, miosis | IVH extension |
| Pons | Coma, pinpoint pupils, quadriplegia, hyperthermia | High mortality |
| Cerebellum | Dizziness, truncal ataxia, vomiting, gaze palsy | Obstructive hydrocephalus - emergency |
| Lobar | Depends on lobe; often less severe | Think CAA in elderly |
PART 11: PROGNOSTICATION - THE ICH SCORE
Primary ICH Score (Hemphill et al.)
| Component | Score |
|---|---|
| GCS 13-15 | 0 |
| GCS 5-12 | 1 |
| GCS 3-4 | 2 |
| ICH Volume <30 mL | 0 |
| ICH Volume ≥30 mL | 1 |
| Intraventricular hemorrhage (IVH) | 1 |
| Infratentorial location | 1 |
| Age ≥80 years | 1 |
| Total range | 0-6 |
ICH Score → 30-day Mortality
| ICH Score | 30-Day Mortality |
|---|---|
| 0 | 0% |
| 1 | 13% |
| 2 | 26% |
| 3 | 72% |
| 4 | 97% |
| 5-6 | ~100% |
FUNC Score (predicts 90-day functional independence): Scores range 0-11; higher FUNC = better function. Considers GCS ≥9 (2 pts), ICH volume <30 mL (4 pts), lobar location (2 pts), age <70 (2 pts), no prior cognitive impairment (1 pt). - Plum & Posner's, p.570
Other Prognostic Factors (Mnemonic: "BAD HEMATOMA")
- B - Big volume (>30 mL = poor)
- A - Age ≥80
- D - Deep location (pontine worst)
- H - Herniation signs
- E - Extension into ventricles (IVH)
- M - Midline shift >5 mm
- A - Anticoagulant use
- T - Temperature (fever = worse outcome)
- O - On warfarin (larger hematomas)
- M - Mental status (low GCS = high mortality)
- A - Age-related cognitive baseline
PART 12: RESOURCE-LIMITED SETTINGS - PRACTICAL ADAPTATIONS
| Standard Care | Limited Resource Alternative |
|---|---|
| Nicardipine infusion | IV Labetalol boluses OR oral Nifedipine (regular, NOT sublingual) |
| 4-Factor PCC | Fresh Frozen Plasma (FFP) 10-15 mL/kg |
| CT angiography | Clinical assessment + noncontrast CT |
| ICP monitor | Clinical markers (Cushing's triad, pupils) + serial GCS |
| Levetiracetam | Phenytoin 20 mg/kg IV (load) |
| Hypertonic saline (3%) | Mannitol 20% (0.25-1 g/kg IV q6h) |
| EVD for hydrocephalus | Urgent neurosurgical referral + temporizing mannitol |
| ICU monitoring | Dedicated nurse q1-2h neuro checks, pulse ox, BP cuff |
Key principle in resource-limited settings:
- Noncontrast CT + clinical exam is your foundation
- Labetalol + mannitol + head positioning can be done anywhere
- Early identification of cerebellar hemorrhage for surgical referral
- Prevent secondary injuries: fever, hyperglycemia, aspiration, DVT
PART 13: DVT AND SECONDARY PREVENTION
- DVT prophylaxis: Intermittent pneumatic compression devices from day 1. No pharmacological anticoagulation acutely for DVT prevention in first 24-48h.
- After hemorrhage stability confirmed (repeat CT at 24-72h), low-dose LMWH may be started for DVT prevention
- Restart anticoagulation in AF patients: generally 4-8 weeks post-ICH, after weighing thromboembolic risk vs. re-bleed risk - decision with neurology/cardiology
PART 14: COMPLICATIONS TO ANTICIPATE
Mnemonic: "SHECKED"
| Letter | Complication | Prevention |
|---|---|---|
| S | Seizures | Monitor, treat if occurs |
| H | Hematoma expansion | BP control within 6h |
| E | Edema/herniation | Osmotherapy, surgery |
| C | Cardiac arrhythmias | ECG monitoring, correct electrolytes |
| K | (Re)Bleed | BP control, coagulopathy reversal |
| E | Electrolyte abnormalities (hyponatremia) | Daily electrolytes |
| D | DVT/PE | Mechanical compression, early mobilization |
SUMMARY: "ONE-PAGE PROTOCOL" FOR ANY ER/WARD
ICH PROTOCOL CARD
-----------------
1. CT HEAD (noncontrast) STAT
2. Airway: intubate if GCS ≤8
3. BP: Target SBP 140-160 mmHg
→ Labetalol IV 20mg bolus q10min
→ Nicardipine 5-15mg/hr if available
4. Reverse coagulopathy: Vit K + FFP/PCC
5. Glucose: 140-180 mg/dL
6. Fever: Treat aggressively
7. Seizures: Treat if occur (no prophylaxis)
8. Head elevated 30°
9. NO steroids, NO aspirin, NO tPA
10. Cerebellar hemorrhage → URGENT surgery consult
11. ICH Score for prognosis (0-6)
12. Repeat CT at 24h or if deteriorates
Sources: - Tintinalli's Emergency Medicine, pp. 1156-1165 | - Frameworks for Internal Medicine, p. 436-495 | - Plum & Posner's Diagnosis and Treatment of Stupor and Coma, pp. 570-580 | - Goldman-Cecil Medicine, p. 3485-3487 | AHA/ASA 2022 ICH Guidelines (Greenberg et al., PMID via Harrison's 22E)
Recent evidence note: A 2024 systematic review (PMID 39090364) on thromboprophylaxis timing in ICH supports early (24-48h) mechanical prophylaxis, with pharmacological DVT prophylaxis safe after hemorrhage stability is confirmed. The 2025 International CAA Association statement (PMID 40721902) updates management for CAA-related hemorrhage in elderly patients.
This is a shared conversation. Sign in to Orris to start your own chat.