fluoride release causing antibacterial effect in GIC cement
glass ionomer cement fluoride release antibacterial
fluoride release GIC glass ionomer cement antibacterial mechanism
fluoride release GIC antibacterial mechanism
Fluoride Release and Antibacterial Effect in Glass Ionomer Cement (GIC)
1. Source of Fluoride in GIC
- Calcium fluoride (CaF2)
- Strontium fluoride (SrF2)
- Lanthanum fluoride (LaF2)
- Cryolite (Na3AlF6)
- Aluminium fluoride (AlF3)
2. Mechanisms of Fluoride Release
- Rapidly dissolving fluoride salts from the outer surface of the cement leach into the surrounding aqueous environment (saliva, crevicular fluid)
- This accounts for the large initial spike in fluoride release seen in the first few hours to days after placement
- A continuous and gradual diffusion of free fluoride ions through the cement matrix into the surrounding environment
- This provides the sustained, low-level release over months and years
- Fluoride release is highest in the first 24-72 hours post-placement
- It declines rapidly in the first week
- Stabilizes after approximately 2-3 months at a lower but clinically significant baseline level
- GIC can release fluoride for considerable periods after setting
3. Fluoride Recharge (Reservoir Effect)
- When environmental fluoride concentration is high (e.g., after application of fluoride toothpaste, varnish, or rinse), GIC absorbs fluoride from the oral environment
- This stored fluoride is subsequently released when ambient levels drop
- This makes GIC function as a fluoride reservoir, providing a buffering effect against caries challenges
4. Antibacterial Mechanisms of Released Fluoride
a) Enolase Inhibition (Primary Mechanism)
- Fluoride ions inhibit enolase (phosphopyruvate hydratase), a key glycolytic enzyme in bacteria
- Enolase catalyzes the conversion of 2-phosphoglycerate to phosphoenolpyruvate in the glycolytic pathway
- Inhibition blocks glycolysis, thus disrupting energy metabolism and acid production in cariogenic bacteria such as Streptococcus mutans
- Fluoride forms a magnesium-fluoride-phosphate complex (Mg2+-F--Pi) that competitively inhibits enolase active site
b) Disruption of Proton-Translocating ATPase (H+-ATPase)
- Fluoride inhibits F-type H+-ATPase in the bacterial cell membrane
- This enzyme maintains intracellular pH homeostasis in aciduric organisms
- Inhibition prevents bacteria from pumping out protons, acidifying the bacterial cytoplasm and disrupting normal cellular function
c) Interference with Bacterial Acid Production
- By blocking glycolysis (via enolase inhibition), fluoride reduces lactic acid output from S. mutans and other acidogenic bacteria
- This raises the local pH, reducing demineralization of tooth structure adjacent to the restoration
d) Inhibition of Bacterial Adhesion and Biofilm Formation
- Fluoride interferes with the synthesis of extracellular polysaccharides (EPS) by cariogenic bacteria (particularly glucosyltransferase-mediated EPS production)
- EPS forms the scaffolding of dental biofilm; disrupting its synthesis reduces bacterial adhesion to tooth surfaces and to the restoration margin
e) Cell Membrane Disruption
- At higher concentrations, fluoride can directly disrupt bacterial cell membrane integrity and increase membrane permeability
5. Anticariogenic Action - Net Effect
| Effect | Mechanism |
|---|---|
| Decreased demineralization | Fluoride in biofilm fluid lowers acid production |
| Increased remineralization | Fluoride promotes fluorapatite deposition |
| Enamel acid resistance | Hydroxyapatite converted to fluorapatite (more acid-resistant) |
| Prevention of secondary caries | Sustained release at cavity margins inhibits residual bacteria |
| Cariostatic effect on adjacent tooth | Fluoride diffuses laterally to surrounding tooth structure |
6. Factors Influencing Fluoride Release
- Fluoride content and type in powder
- Matrix composition (glass particle size, powder-liquid ratio)
- Setting and curing mechanism
- Type of GIC (conventional vs. resin-modified GIC)
- Salivary pH - lower pH increases fluoride release
- Plaque and pellicle formation on surface - reduces release
- Amount of exposed surface area
- Covering with adhesive or surface protective agent reduces release by 1.4-4 fold
- Bleaching and toothbrushing do NOT significantly affect release
7. GIC vs. RMGIC (Resin-Modified GIC)
- Reduces the dissolution mechanism significantly (resin repels water)
- Diffusion mechanism still operates but is partially hindered
- Overall fluoride release from RMGIC is generally lower than conventional GIC, though still clinically significant
Clinical Significance
- Patients with high caries risk
- Atraumatic Restorative Treatment (ART)
- Cervical/root caries restorations
- Restorations in areas difficult to keep dry
- Pediatric dentistry (primary teeth)
- Liner/base under composite in deep cavities
give me a image
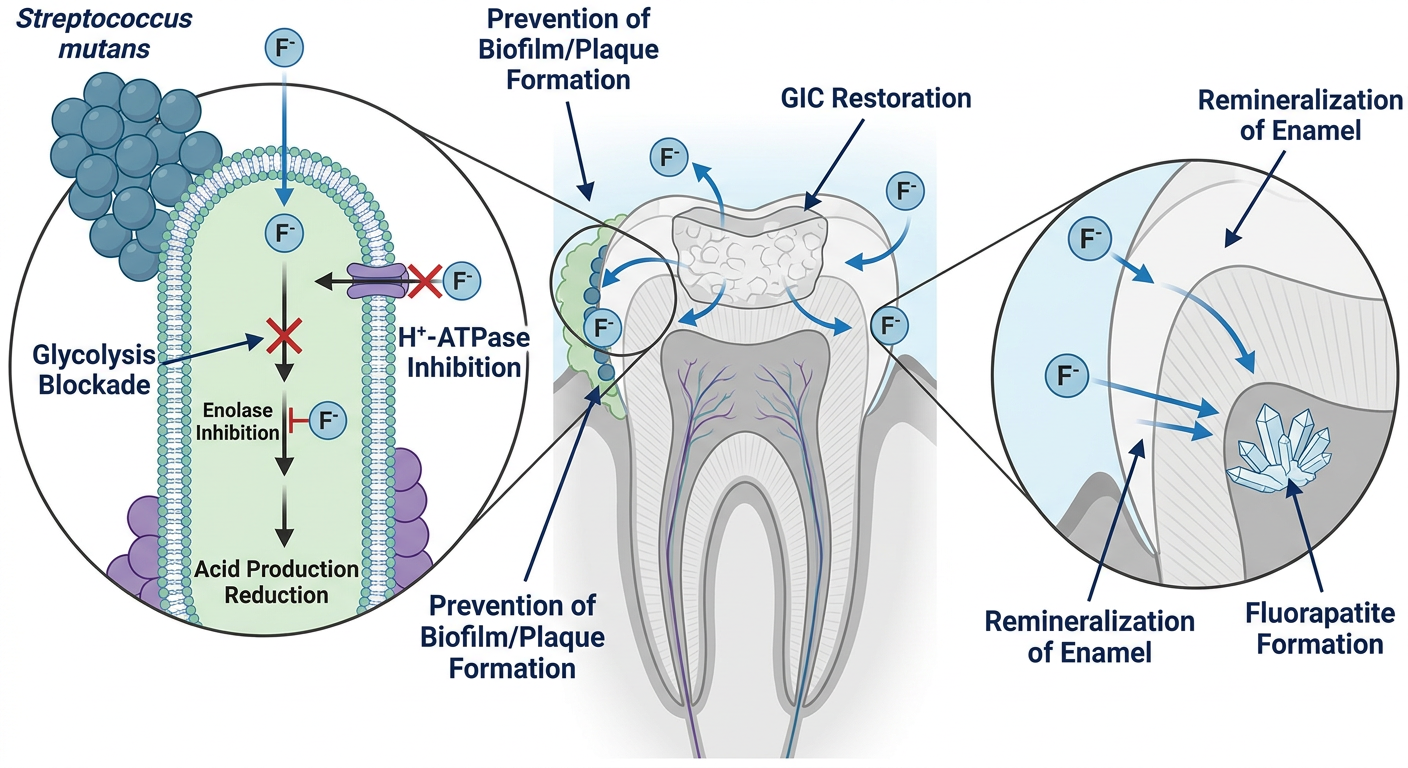
- F- ions released from the set cement via surface dissolution and bulk diffusion
- Enolase inhibition blocking glycolysis in S. mutans - cutting off bacterial energy and acid production
- H+-ATPase disruption - preventing bacteria from maintaining intracellular pH
- Biofilm prevention - fluoride interferes with extracellular polysaccharide synthesis
- Remineralization - fluoride drives conversion of hydroxyapatite to acid-resistant fluorapatite

Glass ionomer cements (GICs) are widely used in restorative dentistry due to their fluoride release and chemical adhesion to dental tissues [1]. GICs offer advantages, such as sustained fluoride release, biocompatibility, esthetic tooth-like appearance, and thermal compatibility with tooth structure [1, 2]. However, their application is limited by low mechanical strength, moisture sensitivity during setting, and poor wear resistance, restricting their use to low-stress clinical areas [2, 3]. To address these shortcomings, several materials have been incorporated into GICs to improve their physical performance [4, 5]. Resin-modified GICs (RMGICs), developed through the addition of resin monomers, show enhanced diametral tensile, flexural, and compressive strength and allow light-curing, providing improved handling and control during placement [6, 7]. The inclusion of resin shortens the setting duration, decreases sensitivity to moisture, provides longer working time, and improves both translucency and overall esthetics [7, 8]. In restorative dentistry, preventing bacterial colonization after caries removal is critical for restoration longevity. Incorporating antibacterial agents into restorative materials helps inhibit bacterial growth and penetration, thereby reducing the risk of recurrent caries [9, 10]. Although, GICs exhibit antibacterial effects attributed to fluoride release and low initial pH, they may not provide sufficient long-term protection against cariogenic bacteria, potentially leading to secondary caries and restoration failure [11]. Consequently, enhancing the antibacterial properties of GICs remains a focus of ongoing research to improve their clinical performance and durability. Zinc oxide (ZnO), known for its antimicrobial properties, is commonly used in dental materials [10, 12]. It is affordable, stable, and biocompatible [10]. Recently, ZnO nanoparticles (ZnO NPs) have gained popularity due to their enhanced antibacterial efficacy [10]. Due to their small size, NPs penetrate dentinal tubules more effectively than larger particles [10]. ZnO NPs show significant antibacterial activity against S. mutans and Lactobacillus, inhibiting biofilm formation when added to dental materials [13]. Moreover, they improve bond strength in enamel and dentin without compromising it during pretreatment [14]. Mesoporous materials, with pore sizes ranging from 2 to 50 nm, have gained significant interest in both medicine and dentistry [15]. These materials are valued for their adjustable pore sizes, biocompatibility, high surface area, and lack of toxicity [16]. Their pore structure can be easily modified, and various synthesis methods enable the optimization of their composition, structure, and porosity [16]. Mesoporous ZnO NPs, characterized by their large surface area, porosity, crystallinity, and antimicrobial properties, show promising potential for a wide range of therapeutic applications [15, 16]. Nanosized materials, particularly mesoporous ZnO NPs, demonstrate significantly enhanced antibacterial properties compared to their bulk counterparts, owing to their increased surface area-to-volume ratio, making them promising candidates as nanofillers for RMGICs [16]. Incorporating nanofillers, such as mesoporous ZnO NPs may enhance antibacterial activity and mechanical performance; however, preserving adequate bond strength is critical and must be thoroughly evaluated. Although, these materials show potential, their influence on the bond strength of resin-modified glass ionomer cement (RMGIC) to enamel and dentin in permanent teeth remains unclear. Therefore, the present study aimed to evaluate and compare the microshear bond strength (µSBS) of RMGIC to enamel and dentin of permanent teeth restored with RMGIC, with and without the incorporation of mesoporous ZnO NPs and ZnO NPs. The null hypothesis proposed that there would be no significant difference in the bond strength of RMGIC to enamel and dentin regardless of the addition of mesoporous ZnO NPs or ZnO NPs.
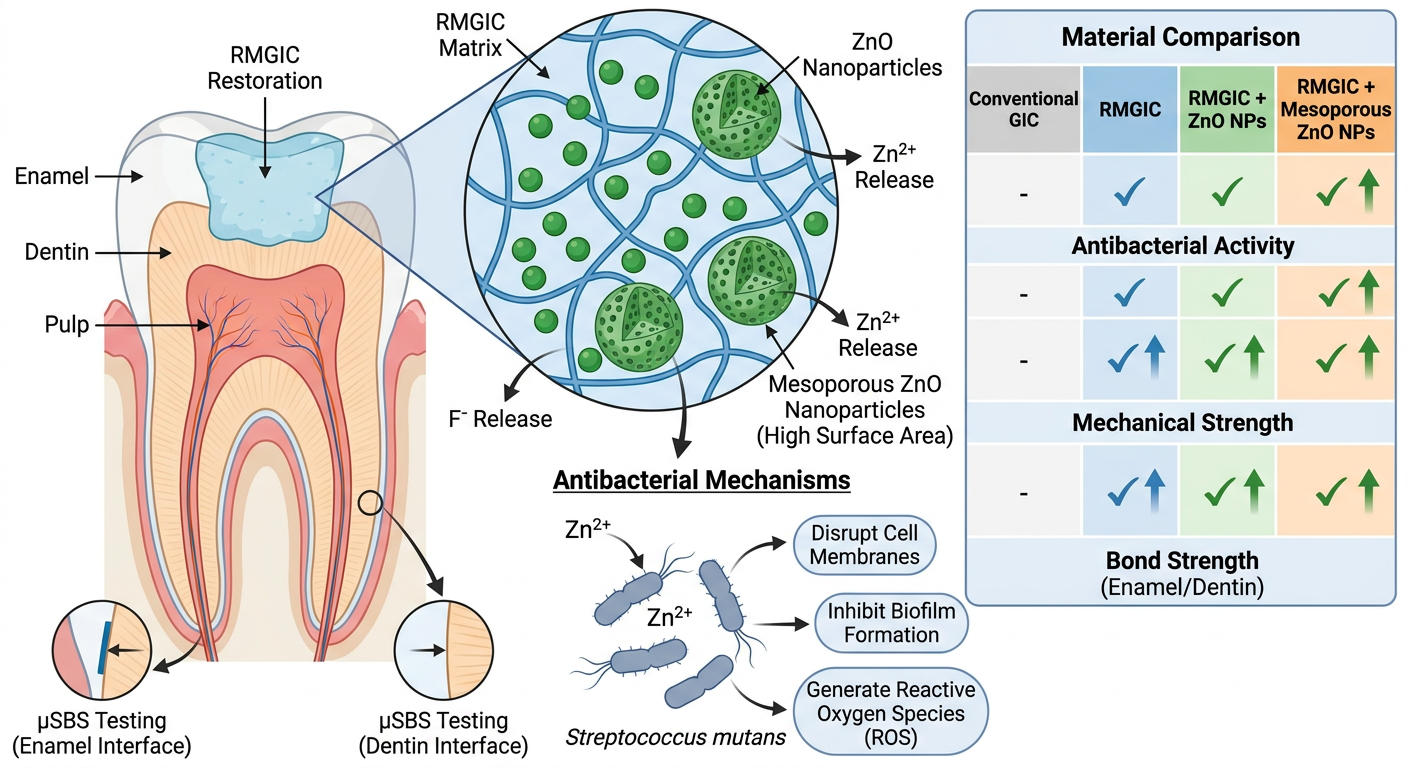
- RMGIC matrix with embedded ZnO NPs and mesoporous ZnO NPs (note the porous structure giving higher surface area)
- Antibacterial mechanisms of ZnO NPs: Zn2+ ion release, reactive oxygen species (ROS) generation, and bacterial membrane disruption targeting S. mutans and Lactobacillus
- Fluoride release from the GIC matrix working alongside ZnO NPs for dual antibacterial action
- Mesoporous advantage: larger surface area-to-volume ratio = enhanced ion release and deeper dentinal tubule penetration
- µSBS testing at enamel and dentin interfaces - the key outcome measure of your study
- Material progression: conventional GIC → RMGIC → RMGIC + ZnO NPs → RMGIC + mesoporous ZnO NPs
GIC fluoride release and bind to tooth structure image
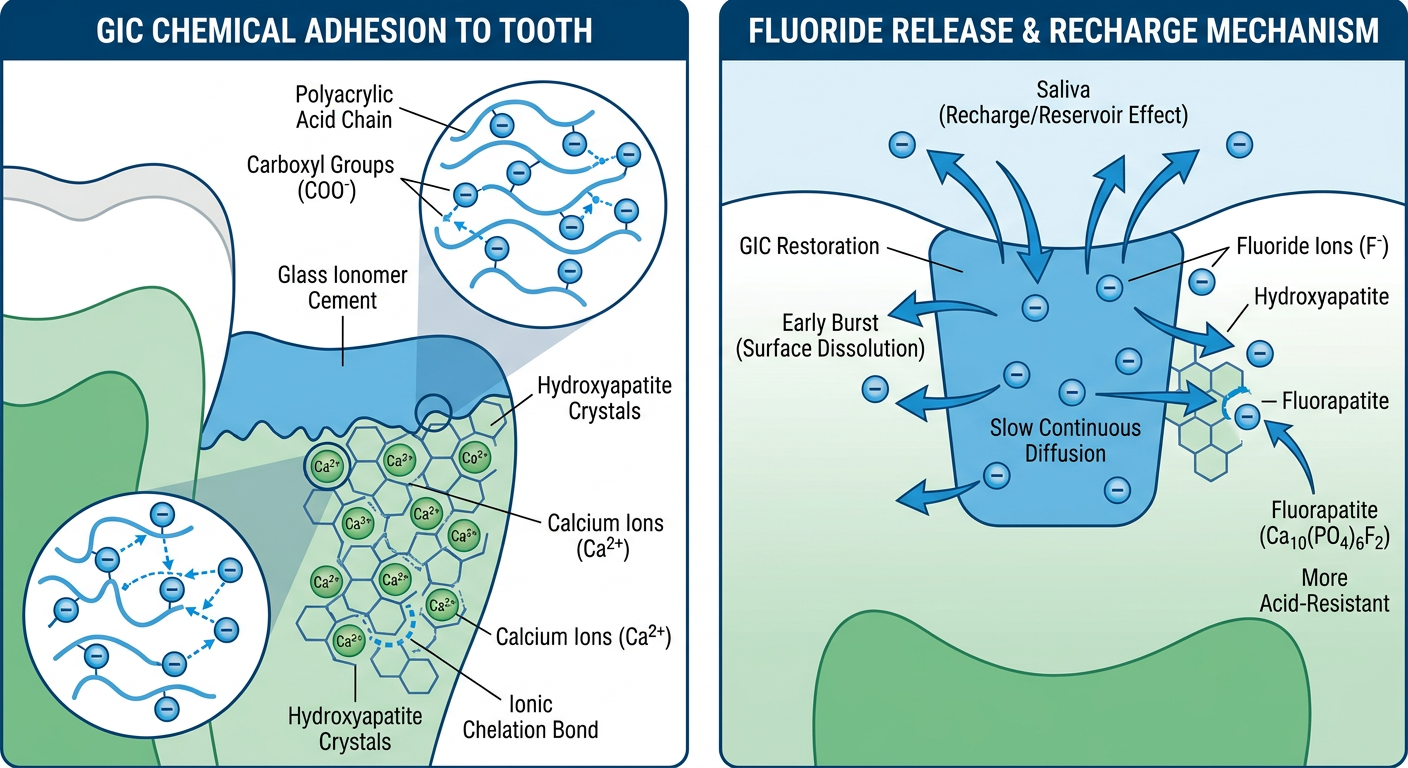
- Polyacrylic acid chains in GIC extend carboxyl groups (-COO-)
- These chelate with Ca2+ ions in the hydroxyapatite of enamel and dentin
- Forms a true ionic chemical bond - unique to GIC among restorative materials
- Bond is stronger to enamel (higher inorganic/hydroxyapatite content) than dentin
- Phase 1 - Early burst: rapid surface dissolution releases a large amount of F- in the first 24-72 hours
- Phase 2 - Sustained diffusion: slow continuous release through the cement matrix over months/years
- Released F- converts hydroxyapatite → fluorapatite (more acid-resistant crystal)
- Reservoir/recharge effect: GIC absorbs F- from fluoride toothpaste/varnish and re-releases it later - acting as a fluoride buffer in the oral environment