Orbit explain in detail for ophthalmology mbbs
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
I now have very comprehensive material. Let me compile the full detailed answer on the orbit for MBBS ophthalmology.
The Orbit - A Complete MBBS Ophthalmology Guide
1. Introduction
The orbits are paired, pyramid-shaped bony cavities in the upper half of the face, positioned below the anterior cranial fossa and anterior to the middle cranial fossa. Each orbit contains the eyeball, optic nerve, extra-ocular muscles, lacrimal apparatus, adipose tissue, fascia, and the nerves and vessels supplying these structures.
Key dimensions (clinical importance):
- Volume: approximately 30 mL
- Shape: pyramid with base facing anteriorly and apex directed posteromedially
- The orbital axis diverges about 23° from the visual axis
2. Bony Orbit - The Seven Bones
Mnemonic: "My Zipper Fell Early Last Summer Pm" (Maxilla, Zygomatic, Frontal, Ethmoid, Lacrimal, Sphenoid, Palatine)
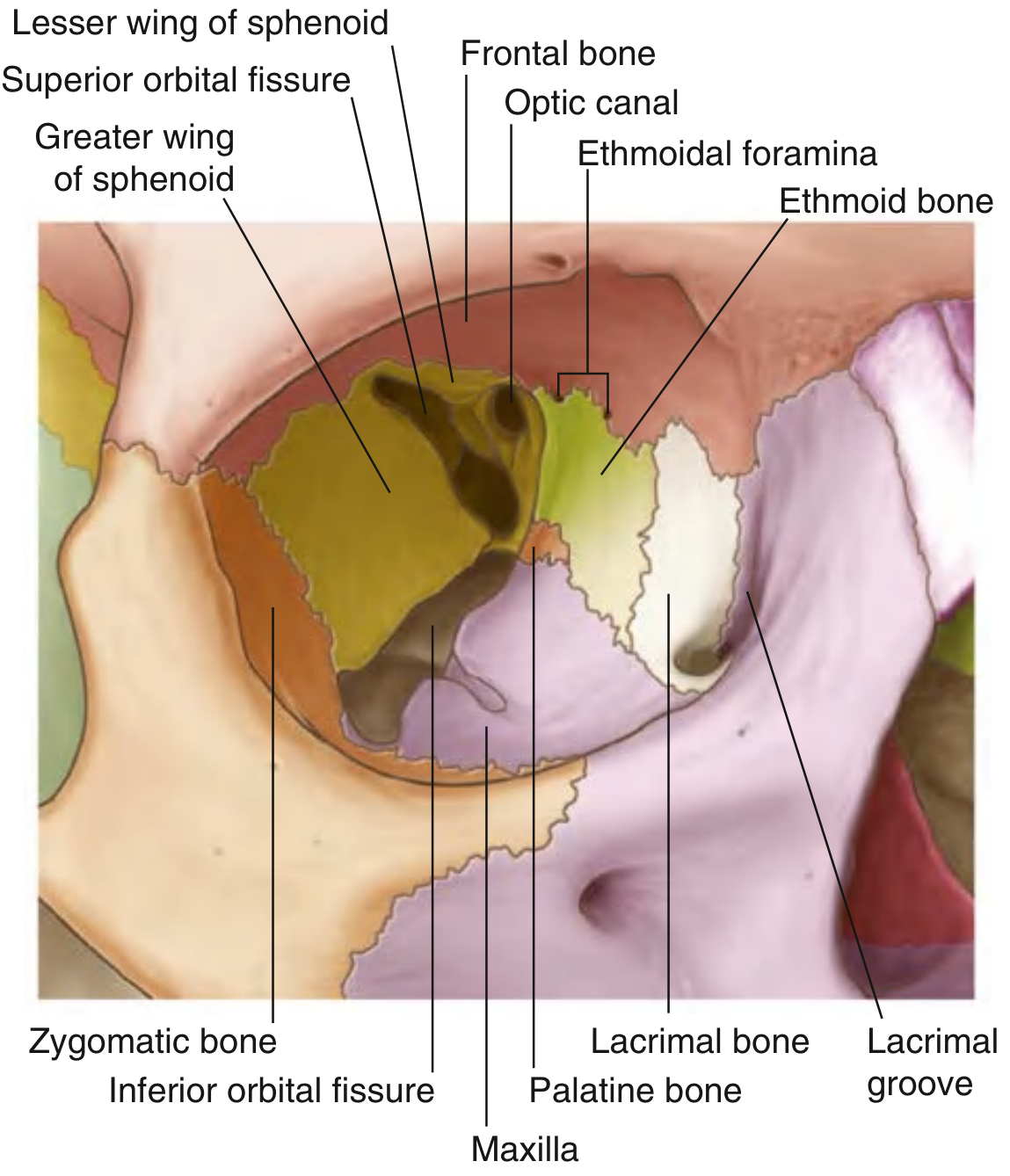
Fig. - Bones of the Orbit (Gray's Anatomy for Students)
The bony orbit takes the shape of a pyramid. The wide base opens anteriorly onto the face; the apex extends posteromedially.
The Orbital Rim (Base of the Pyramid)
| Margin | Bone |
|---|---|
| Superior | Frontal bone |
| Medial | Frontal process of maxilla |
| Inferior | Zygomatic process of maxilla + zygomatic bone |
| Lateral | Zygomatic bone + frontal process of zygoma + zygomatic process of frontal bone |
3. The Four Orbital Walls
Roof (Superior Wall)
- Formed by the orbital part of the frontal bone (mainly) + small contribution from the lesser wing of sphenoid posteriorly
- Thin plate of bone separating the orbit from the anterior cranial fossa and the brain
- Special features:
- Anteromedially: trochlear fovea (pulley for superior oblique muscle) and possible intrusion of the frontal sinus
- Anterolaterally: lacrimal fossa (contains orbital part of lacrimal gland)
- Clinical note: roof fractures are common in children from minor brow trauma
Medial Wall
- Four bones (medial to lateral): Maxilla + Lacrimal + Ethmoid + Sphenoid (mnemonic: "MALES")
- Largest contributor: orbital plate of ethmoid (contains ethmoidal air cells - very thin, "lamina papyracea")
- Junction of roof and medial wall: anterior and posterior ethmoidal foramina (for anterior/posterior ethmoidal nerves and vessels)
- Anterior portion: lacrimal groove formed by lacrimal bone (posterior lacrimal crest) and frontal process of maxilla (anterior lacrimal crest) - contains the lacrimal sac
- Both medial walls are parallel to each other
- Clinical: medial wall is the thinnest wall - fractures allow air from ethmoid sinuses into orbit ("orbital emphysema" - patient feels fullness on blowing nose)
Floor (Inferior Wall)
- Also the roof of the maxillary sinus
- Bones: orbital surface of maxilla (mainly) + contributions from zygomatic and palatine bones
- The inferior orbital fissure begins posteriorly and runs along the lateral boundary of the floor
- Clinical: most commonly fractured wall in blow-out fractures - muscle entrapment causes diplopia
Lateral Wall
- Two bones: zygomatic bone (anterior) + greater wing of sphenoid (posterior)
- The superior orbital fissure lies between the greater and lesser wings of the sphenoid
- This is the thickest, strongest wall - fractures require major force
- Clinical: lateral wall separates the orbit from the middle cranial fossa and temporal lobe
4. Important Orbital Openings (Foramina and Fissures)
| Opening | Location | Contents |
|---|---|---|
| Optic canal | Apex, between lesser wing of sphenoid and body of sphenoid | Optic nerve (CN II), ophthalmic artery, sympathetic fibers |
| Superior orbital fissure (SOF) | Between greater and lesser wings of sphenoid | CN III, IV, V1 (lacrimal, frontal, nasociliary branches), CN VI, superior ophthalmic vein, sympathetic fibers |
| Inferior orbital fissure (IOF) | Between greater wing of sphenoid/maxilla and zygomatic bone | Maxillary nerve (V2), zygomatic nerve, inferior ophthalmic vein (connects to pterygoid plexus) |
| Anterior ethmoidal foramen | Frontoethmoidal suture | Anterior ethmoidal nerve and vessels |
| Posterior ethmoidal foramen | Frontoethmoidal suture, more posterior | Posterior ethmoidal nerve and vessels |
| Lacrimal groove | Medial wall | Nasolacrimal duct (drains to inferior meatus) |
| Infraorbital groove/canal | Floor (anterior) | Infraorbital nerve and artery (branch of V2) |
| Zygomaticotemporal/facial foramina | Lateral wall | Zygomaticotemporal and zygomaticofacial nerves |
5. Orbital Septum - The Key Dividing Structure
The orbital septum is a fibrous sheet that extends from the orbital rim (periosteum) into both eyelids. It is the anatomical boundary separating:
- Pre-septal (preseptal) space - anterior to the septum (eyelid proper)
- Post-septal (orbital) space - posterior to the septum (true orbit)
This distinction is critical in classifying periorbital infections (Chandler classification).
6. Contents of the Orbit
- Eyeball (globe)
- Optic nerve - CN II (from globe to optic canal)
- Extra-ocular muscles (EOMs): 4 rectus muscles (superior, inferior, medial, lateral) + 2 oblique muscles (superior, inferior) + levator palpebrae superioris
- Lacrimal gland - in lacrimal fossa of the frontal bone (anterolateral)
- Cranial nerves: CN III (oculomotor), IV (trochlear), V1 (ophthalmic), VI (abducens)
- Ophthalmic artery and its branches
- Ophthalmic veins (superior and inferior) - drain to cavernous sinus
- Ciliary ganglion - parasympathetic ganglion in posterior orbit (lateral to optic nerve)
- Orbital fat - fills the space and cushions structures
7. Clinical Conditions of the Orbit
7A. Orbital Cellulitis (Bacterial)
Definition: Serious infection of the soft tissues posterior to the orbital septum (post-septal). Sight- and life-threatening.
Common organisms: Streptococcus pneumoniae, Staphylococcus aureus, Streptococcus pyogenes, Haemophilus influenzae
Most common source: Paranasal sinuses (especially ethmoid sinuses in children) - because the thin lamina papyracea allows direct spread
Clinical features:
- Rapid onset pain (worse on eye movement)
- Proptosis (may be non-axial/dystopia if abscess present)
- Painful ophthalmoplegia
- Reduced VA, impaired colour vision
- RAPD (afferent pupillary defect) - suggests optic nerve compression
- Tender, erythematous, warm eyelids + chemosis
- Pyrexia - often marked
- Choroidal folds, optic disc swelling on fundoscopy
Complications:
- Optic neuropathy, exposure keratopathy, raised IOP
- Subperiosteal abscess (most common along medial wall)
- Intracranial: meningitis, brain abscess, cavernous sinus thrombosis
Investigations:
- WBC, blood cultures, nasal swab cultures
- High-resolution CT orbit + sinuses + brain (modality of choice - confirms diagnosis, excludes abscess)
- MRI also used
Treatment:
- Mandatory hospital admission + urgent ENT review
- IV antibiotics: ceftazidime + oral metronidazole (cover anaerobes)
- Continue IV until apyrexial 4 days, then oral 1-3 weeks
- Optic nerve function monitored every 4 hours (VA, color vision, pupil)
- Surgery: drain subperiosteal abscess; drain infected sinuses if not responding
7B. Preseptal (Periorbital) Cellulitis
Definition: Infection anterior to the orbital septum - less severe than orbital cellulitis.
Organisms: Staphylococcus aureus, Streptococcus pyogenes
Key distinguishing features from orbital cellulitis:
- No proptosis, no chemosis
- Normal VA, normal pupillary reactions, normal ocular motility
- Swollen, firm, tender, red eyelid
Treatment: Oral co-amoxiclav (250-500 mg/125 mg 2-3 times daily); IV if severe
7C. Chandler-Hubert Classification of Orbital Complications of Sinusitis
| Stage | Type | Features |
|---|---|---|
| I | Preseptal (periorbital) cellulitis | Anterior to septum; no proptosis |
| II | Post-septal (orbital) cellulitis | Behind septum; proptosis |
| III | Subperiosteal abscess | Collection between periorbita and orbital wall |
| IV | Orbital abscess | Collection within orbital fat |
| V | Cavernous sinus thrombosis | Bilateral signs, severe; most dangerous |
7D. Blow-out Fractures of the Orbit
Mechanism: A blunt object larger than the orbital aperture (fist, tennis ball, etc.) strikes the periorbital area. Sudden increase in intraorbital pressure is transmitted to the bony walls - the thinnest walls fracture preferentially.
Most commonly fractured wall: floor (over infraorbital canal) > medial wall
Orbital Floor Fracture
Clinical features:
- Periocular ecchymosis and oedema
- Subcutaneous emphysema (crackling on palpation - air from maxillary sinus)
- Infraorbital nerve anaesthesia: numbness of lower lid, cheek, side of nose, upper lip, upper teeth and gums (infraorbital canal frequently involved)
- Diplopia - mechanisms:
- Haemorrhage/oedema restricting inferior rectus/oblique movement (temporary)
- Mechanical entrapment of inferior rectus or inferior oblique within the fracture - diplopia in upgaze and downgaze
- Contusion of extraocular muscles
- Orbital haemorrhage
- Enophthalmos (sunken eye) - due to increased orbital volume; may be masked initially by oedema
Investigations: CT scan (coronal views are best); "teardrop sign" (herniated orbital fat hanging into maxillary sinus)
Treatment:
- Most resolve with observation if no entrapment/significant diplopia
- Surgery (repair of orbital floor) indicated for:
- Persistent diplopia with motility restriction
- Enophthalmos >2 mm
- Large fracture with significant tissue prolapse
- Infraorbital anaesthesia (relative indication)
Medial Wall Fracture
- Usually associated with floor fractures; rarely isolated
- Signs: periorbital ecchymosis, subcutaneous emphysema (nose blowing)
- Medial rectus entrapment: defective abduction and adduction
- Treatment: release entrapped tissue, repair bony defect
Roof Fracture
- Rare; more common in children
- Haematoma/ecchymosis of upper eyelid
- Large fractures: globe pulsation (CSF pressure transmission)
- Exclude CSF leak (meningitis risk)
Orbital Haemorrhage (Retrobulbar)
- Can cause acute orbital compartment syndrome with compressive optic neuropathy - can cause irreversible blindness
- Causes: trauma, iatrogenic (peribulbar/retrobulbar block), vascular anomalies
- Emergency management: lateral canthotomy and cantholysis to decompress the orbit
7E. Idiopathic Orbital Inflammatory Disease (Orbital Pseudotumour)
Also called: Non-specific orbital inflammation (NSOI)
Definition: Non-neoplastic, non-infective, space-occupying orbital infiltration with inflammatory features. Histology shows pleomorphic inflammatory cell infiltration + reactive fibrosis.
Key features:
- Usually unilateral in adults; bilateral in children
- Acute/subacute onset of ocular and periocular redness, swelling, and pain
- Congestive proptosis
- Mild to severe ophthalmoplegia
- Features of optic nerve dysfunction (esp. posterior orbit involvement)
- Choroidal folds possible
Course:
- Spontaneous remission after a few weeks
- Intermittent episodes with eventual remission
- Severe prolonged inflammation → progressive fibrosis → "frozen orbit" (ophthalmoplegia + ptosis + visual impairment)
Investigations:
- CT: ill-defined orbital opacification and loss of definition of orbital contents
- Biopsy: often required to confirm diagnosis and exclude lymphoma, neoplasia, sarcoidosis, granulomatosis with polyangiitis
Treatment: Oral/IV corticosteroids (highly responsive - "steroid test"); biopsy if no response
7F. Thyroid Eye Disease (Graves' Orbitopathy / Dysthyroid Orbitopathy)
Most common cause of unilateral and bilateral proptosis (exophthalmos) in adults
Activity is graded using the Clinical Activity Score (CAS):
- One point each for: pain on eye movement, eye pain at rest, eyelid erythema, conjunctival injection, chemosis, eyelid swelling, caruncle/plica inflammation
- Score ≥3/7 = active disease requiring immunosuppression
Systemic steroids are the mainstay for moderate-severe active disease:
- Oral prednisolone 60-80 mg/day initially, tapered by response
- IV methylprednisolone preferred (better tolerability, superior outcomes):
- Lower-intensity regimen: 0.5 g once weekly x 6 weeks, then 0.25 g once weekly x 6 weeks
- Acute compressive optic neuropathy: pulsed IV methylprednisolone 0.5-1 g (3 successive days or alternate days)
- Contraindications to IV: significant hepatic dysfunction, cardiovascular disease, uncontrolled hypertension/diabetes
Orbital decompression (removing orbital walls) indicated for:
- Compressive optic neuropathy unresponsive to steroids
- Intractable corneal exposure
- Cosmetically disabling proptosis
Orbital radiotherapy: Low-dose fractionated; second-line therapy; used with or instead of steroids; response in 6 weeks, max by 4 months; ~40% do not respond. Adverse effects: cataract, radiation retinopathy, optic neuropathy.
7G. Rhino-Orbital Mucormycosis
Setting: Uncontrolled diabetic ketoacidosis, immunocompromised patients (post-COVID, haematological malignancies, transplant)
Features:
- Rapid spread from nasal/sinus mucosa → orbit → intracranially
- Black eschar on nasal mucosa
- Orbital cellulitis signs + severe proptosis
- Very high mortality if untreated
Treatment:
- Correct underlying metabolic defect (control DKA)
- IV antifungal (amphotericin B)
- Daily packing/irrigation with antifungal agent
- Wide surgical excision of devitalized/necrotic tissue; exenteration in unresponsive cases
- Adjunctive hyperbaric oxygen
8. Differential Diagnosis of an Acutely Inflamed Orbit
(From Kanski's Clinical Ophthalmology)
| Category | Conditions |
|---|---|
| Infection | Bacterial orbital cellulitis, fungal orbital infection (mucormycosis), dacryocystitis, infective dacryoadenitis |
| Vascular | Acute orbital haemorrhage, cavernous sinus thrombosis, carotid-cavernous fistula |
| Neoplasia | Rhabdomyosarcoma, leukaemia, neuroblastoma (children); lacrimal gland tumour; lymphoma; metastasis; retinoblastoma |
| Endocrine | Thyroid eye disease (rapid onset) |
| Non-neoplastic inflammation | Orbital pseudotumour (IOID), Tolosa-Hunt syndrome, orbital myositis, sarcoidosis, granulomatosis with polyangiitis, scleritis, ruptured dermoid cyst |
9. Key Mnemonics and Memory Aids
Seven bones of the orbit: "My Zipper Fell Early Last Summer (at) Pompeii"
- Maxilla, Zygomatic, Frontal, Ethmoid, Lacrimal, Sphenoid, Palatine
Contents of the Superior Orbital Fissure: "LFT SO COLD"
- Lacrimal nerve, Frontal nerve, Trochlear nerve (CN IV), Superior ophthalmic vein, Oculomotor nerve (CN III), Ciliary nerve (nasociliary), Abducens (CN VI)
Chandler classification: "Pre-Post-Sub-Orb-Cave" (I to V)
Thinnest orbital wall: Medial (lamina papyracea of ethmoid) - most common site of subperiosteal abscess in orbital cellulitis
Most commonly fractured floor: Blow-out fracture → inferior rectus entrapment → upgaze diplopia
10. Summary Table - Quick Revision
| Feature | Preseptal Cellulitis | Orbital Cellulitis |
|---|---|---|
| Location | Anterior to septum | Posterior to septum |
| Proptosis | Absent | Present |
| Chemosis | Absent | Present |
| Ocular motility | Normal | Reduced (painful) |
| VA | Normal | May be reduced |
| Pupil | Normal | RAPD possible |
| Management | Oral antibiotics (outpatient usually) | IV antibiotics, hospital admission |
| Risk | Low | Sight/life-threatening |
Sources: Gray's Anatomy for Students; Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Edition
This is a shared conversation. Sign in to Orris to start your own chat.