Hi
Hey! How can I help you today?
Tell mee about telmisartan
Reading File
Searching PubMed
telmisartan hypertension cardiovascular
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Here is a detailed overview:
Telmisartan (Micardis)
Drug Class
Telmisartan is an Angiotensin II Receptor Blocker (ARB) - a nonpeptide, noncompetitive antagonist at the AT1 receptor. Chemically, it is a nonbiphenyl tetrazole derivative that incorporates a carboxylic acid as the biphenyl acidic group, distinguishing it from other ARBs like losartan.
Mechanism of Action
Telmisartan blocks AT1 receptors with high specificity and receptor affinity, preventing angiotensin II from:
- Causing vasoconstriction
- Stimulating aldosterone secretion
- Promoting sodium and water retention
Unlike ACE inhibitors, ARBs like telmisartan block AT1 regardless of how angiotensin II was generated (including via chymase and other ACE-independent pathways). They also permit ongoing AT2 receptor activation, which may have vasodilatory and anti-proliferative benefits.
Telmisartan also has partial PPAR-gamma agonist activity, which may offer metabolic advantages (insulin sensitization, improved glucose/lipid metabolism).
Pharmacokinetics
| Parameter | Telmisartan |
|---|---|
| Peak plasma levels | 0.5 - 1 hour after oral dosing |
| Half-life (t½) | ~24 hours (longest among ARBs) |
| Protein binding | Very high (>99%) |
| Elimination | Mainly by biliary secretion of intact drug |
| Renal insufficiency | No dose adjustment needed |
| Hepatic insufficiency | Plasma clearance is reduced - use with caution |
| Dialyzable | No |
| Sex differences | Women achieve plasma levels 2-3x higher than men, but BP response is similar |
- Goodman & Gilman's Pharmacological Basis of Therapeutics; Brenner and Rector's The Kidney
Dosing
- Starting dose: 40 mg once daily
- Usual dose: 40-80 mg once daily
- Onset of action: ~3 hours (dose-dependent)
- Duration: 24 hours; the drug's effect may persist up to 7 days after stopping
- The uniquely long half-life makes telmisartan one of the most effective ARBs for 24-hour BP control, including nocturnal blood pressure.
Indications
- Hypertension - first-line treatment; once-daily dosing provides full 24-hour coverage
- Cardiovascular risk reduction - the landmark ONTARGET trial showed telmisartan had similar efficacy to ramipril (an ACE inhibitor) in reducing cardiovascular events (MI, stroke, cardiovascular death) in high-risk vascular patients, with less angioedema
- Diabetic nephropathy / kidney protection - the INNOVATION trial showed ARB-based regimens (including telmisartan) reduced progression from micro- to macroalbuminuria in type 2 diabetes
- ACE inhibitor intolerance - preferred alternative when ACE inhibitors cause cough or angioedema
- Antipsychotic-associated hypertension - Maudsley Prescribing Guidelines note specific evidence for telmisartan in this setting
Comparison with ACE Inhibitors (ONTARGET)
- Telmisartan = ramipril for cardiovascular and kidney outcomes in high-risk patients
- ARBs cause no cough (unlike ACE inhibitors) and rarely cause angioedema
- Both drug classes show similar efficacy in type 2 diabetic nephropathy
- Combination of ARB + ACE inhibitor is NOT recommended - increases adverse effects (hypotension, renal failure, hyperkalemia) without adding benefit
Adverse Effects (Class Effects)
| Effect | Notes |
|---|---|
| Hyperkalemia | Due to reduced aldosterone; caution with K+ supplements or K+-sparing diuretics |
| Hypotension | Especially first dose in volume-depleted patients |
| Renal impairment | Acute kidney injury, especially in bilateral renal artery stenosis |
| Fetotoxicity / Teratogenicity | Contraindicated in pregnancy (causes fetal renal dysgenesis, oligohydramnios, neonatal anuria) |
| Dizziness, headache | Generally well tolerated |
| No dry cough | Advantage over ACE inhibitors |
| No angioedema | Rare, unlike ACE inhibitors |
Key Contraindications
- Pregnancy (Category D/X - absolute contraindication in 2nd and 3rd trimesters)
- Bilateral renal artery stenosis
- Concurrent use with aliskiren in patients with diabetes or renal impairment
- Combination with another RAAS blocker (ACE inhibitor or aliskiren)
Special Points
- Hepatic disease: Use with caution - telmisartan is cleared almost entirely by the liver/bile; hepatic insufficiency raises plasma levels
- Renal disease: No dose adjustment required, making it convenient in CKD patients
- Telmisartan is not dialyzable, so no supplement dose is needed after dialysis
- Among ARBs, azilsartan is superior to telmisartan for BP lowering at equivalent doses, but telmisartan's long half-life gives it an edge in nocturnal/early-morning BP control
Recent Evidence (2024-2026)
A 2026 GRADE-assessed meta-analysis (PMID: 41222871) found that a low-dose triple-pill of telmisartan + amlodipine + indapamide is effective and well-tolerated as initial hypertension therapy, supporting its use in combination regimens. A 2024 meta-analysis on ARBs and nocturnal BP (PMID: 38830046) highlighted that long-acting ARBs like telmisartan are particularly effective for reducing overnight blood pressure.
Sources: Brenner & Rector's The Kidney; Goodman & Gilman's Pharmacological Basis of Therapeutics; National Kidney Foundation Primer on Kidney Diseases; Lippincott Illustrated Reviews: Pharmacology; Maudsley Prescribing Guidelines
Management of dka
Reading File
Searching PubMed
diabetic ketoacidosis management treatment
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive data from multiple authoritative sources. Here is the complete, structured guide to DKA management:
Management of Diabetic Ketoacidosis (DKA)
Diagnostic Criteria (ADA - Adults)
| Severity | Glucose (mg/dL) | pH | HCO3 (mmol/L) | Ketones | Mental Status |
|---|---|---|---|---|---|
| Mild | >250 | 7.25-7.30 | 15-18 | Positive | Alert |
| Moderate | >250 | 7.00-7.24 | 10-15 | Positive | Alert/Drowsy |
| Severe | >250 | <7.00 | <10 | Positive | Stupor/Coma |
B-hydroxybutyrate >3.0 mmol/L confirms DKA (more reliable than urine ketones, which can be falsely low as nitroprusside does not detect beta-hydroxybutyrate).
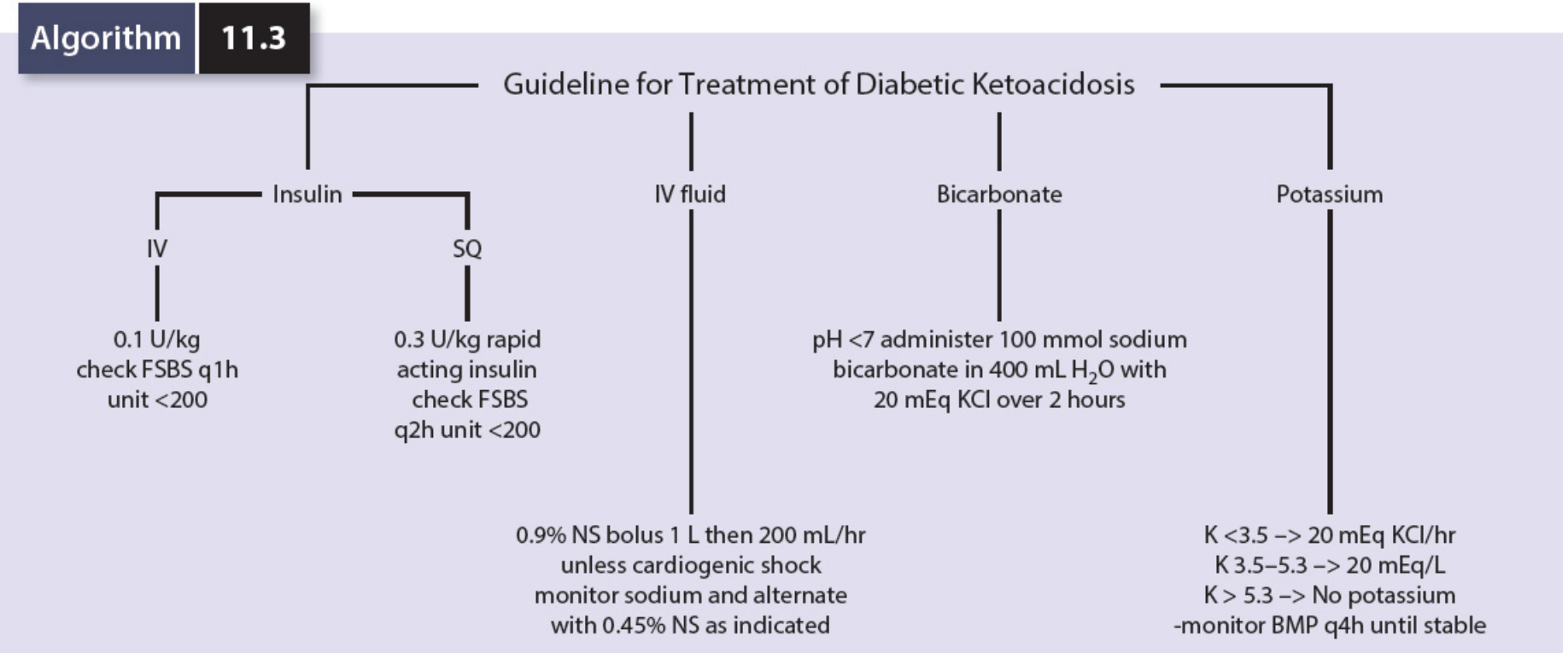
DKA Treatment Algorithm
1. Initial Assessment & Monitoring
- IV access, continuous cardiac monitoring (ICU/HDU admission)
- Hourly blood glucose, q2-4h electrolytes, VBG
- Catheterize if oliguria/no urine output
- Check for precipitating cause (infection, missed insulin, MI, etc.)
- Typical deficits: 5-10 L fluid, 5-10 mmol/kg sodium, up to 7 mmol/kg potassium
2. IV Fluid Resuscitation
- First choice: 0.9% Normal Saline (even if serum osmolality is high - NS is relatively hypotonic)
- Rate: 2-4 L in the first 2-4 hours in DKA
- Once glucose falls to <250 mg/dL, add 10% dextrose as a substrate for continued insulin infusion
- Alternate with 0.45% NS as guided by sodium levels
- Caution: Slow the rate in ischemic heart disease, heart failure, or renal impairment
Large volumes of 0.9% NS can cause hyperchloremic normal anion gap acidosis - this is expected and self-corrects over days as the kidneys restore bicarbonate. - Goldman-Cecil Medicine
3. Insulin Therapy
| Route | Dose | Monitoring |
|---|---|---|
| IV infusion (standard) | 0.1 units/kg/hour | Check blood glucose hourly |
| Subcutaneous (alternative) | 0.3 units/kg rapid-acting insulin, then 0.2 units/kg q2h | Check blood glucose q2h |
Key rules:
- Do NOT start insulin if K+ <3.5 mEq/L - correct potassium first to avoid fatal hypokalemia
- Once glucose falls to <250 mg/dL AND ketones <1.0 mmol/L, reduce insulin infusion to 0.05 units/kg/hour
- If patient was already on background long-acting insulin subcutaneously, continue it alongside IV insulin
- Transition to subcutaneous insulin: Once patient can eat. Overlap SC and IV insulin by 1-2 hours before stopping the infusion to prevent rebound ketosis
Blood glucose falls ~10% per hour; acidosis corrects more slowly. - Goodman & Gilman's
4. Potassium Replacement
| Serum K+ | Action |
|---|---|
| <3.5 mEq/L | Give 20-40 mEq KCl/hr IV; hold insulin until K+ ≥3.5 |
| 3.5-5.3 mEq/L | Add 20-40 mEq KCl per liter of IV fluid |
| >5.3 mEq/L | No potassium; monitor BMP every 4 hours |
| >5.5 mEq/L | Hold potassium entirely |
Why: Initial hyperkalemia is common (K+ shifts extracellularly in acidosis), but total body potassium is always depleted. Insulin drives K+ back into cells, causing rapid and potentially life-threatening drops.
5. Bicarbonate
- Generally NOT recommended - risks paradoxically worsening CNS pH, volume overload, hypernatremia, and rebound alkalosis
- Consider only if:
- pH <7.0 (some guidelines use <7.1) AND
- Patient not responding to insulin and fluids
- If given: 100 mmol NaHCO3 in 400 mL water + 20 mEq KCl over 2 hours
6. Phosphate & Magnesium
- Measure and monitor levels
- Routine IV replacement is not recommended
- Replace only if phosphate <1.0 mg/dL with profound muscle weakness or respiratory compromise
7. Identify & Treat the Precipitating Cause
Common precipitants (the "6 I's"):
- Infection (most common - pneumonia, UTI, cellulitis)
- Insulin omission/non-compliance
- Ischemia (MI, stroke)
- Intoxication
- Iatrogenic (steroids, SGLT2 inhibitors)
- Initial presentation of new T1DM
Note: Elevated WBC and amylase in DKA do NOT necessarily indicate infection or pancreatitis - these are often direct effects of metabolic acidosis. - Goldman-Cecil Medicine
8. Resolution Criteria
DKA is considered resolved when ALL of the following are met:
- Blood glucose <200-250 mg/dL
- Serum bicarbonate ≥15 mmol/L
- Venous pH >7.3
- Anion gap closed (<12)
- Serum/capillary beta-hydroxybutyrate <1.0 mmol/L
9. Complications to Watch For
| Complication | Notes |
|---|---|
| Hypokalemia | Most dangerous; from insulin + fluids driving K+ intracellularly |
| Hypoglycemia | Monitor hourly; add dextrose when glucose <250 mg/dL |
| Cerebral edema | Occurs in ~1% - mainly children. Caused by rapid rehydration/osmotic shifts. Prevent with gradual rehydration over 48 hours and avoiding hypotonic fluids. Treat with mannitol, fluid restriction, hyperventilation |
| Hyperchloremic acidosis | From large NS volumes - self-corrects |
| Thrombosis | DKA is a prothrombotic state; stroke risk is elevated |
Recent Evidence (2024-2026)
- A 2026 meta-analysis (PMID: 41208563) found that adding early subcutaneous basal insulin alongside IV insulin infusion in DKA management reduces time to DKA resolution and facilitates earlier transition off IV insulin without increasing hypoglycemia risk.
- A 2025 consensus report (PMID: 40032308) reviewing the 2024 ADA/EASD consensus on hyperglycemic crises highlights updated guidance on fixed-rate IV insulin, ketone monitoring using beta-hydroxybutyrate, and expanded SGLT2-inhibitor-associated euglycemic DKA recognition.
Sources: Goldman-Cecil Medicine; Comprehensive Clinical Nephrology 7e; Goodman & Gilman's Pharmacological Basis of Therapeutics; Bradley & Daroff's Neurology in Clinical Practice; Mulholland & Greenfield's Surgery 7e
This is a shared conversation. Sign in to Orris to start your own chat.