Sequence of bone erosion by cholestetaoma
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive data from multiple authoritative ENT textbooks. Here is a complete, well-sourced answer.
Sequence of Bone Erosion by Cholesteatoma
Cholesteatoma erodes bone in a fairly predictable medial-to-lateral and inferior-to-superior pattern as it expands from its point of origin (usually the Prussak space in pars flaccida cholesteatoma). The osteolytic process is driven by osteoclast activation stimulated by cytokines (TNF-α, IL-1a, IL-1b, IL-6) and lipopolysaccharides from bacteria colonizing the sac.
Classic Sequence (Pars Flaccida / Attic Cholesteatoma)
| Step | Structure Eroded | Clinical Consequence |
|---|---|---|
| 1 | Scutum (lateral wall of epitympanum) | Earliest CT finding; classic notch sign |
| 2 | Ossicular chain - long process of incus first, then malleus handle, then stapes suprastructure | Conductive hearing loss (most common presenting symptom) |
| 3 | Tegmen tympani / tegmen mastoideum (roof of middle ear / mastoid) | Risk of brain hernia, CSF leak, meningitis, temporal lobe abscess |
| 4 | Fallopian canal (facial nerve canal) - most commonly at the second genu | Facial nerve palsy (acute with infection, or insidious) |
| 5 | Otic capsule - lateral (horizontal) semicircular canal first (~98% of labyrinthine fistulas), then posterior SCC, then cochlea | Labyrinthine fistula → sensorineural hearing loss + vertigo (Tullio phenomenon) |
| 6 | Sigmoid sinus plate / dural plates | Sigmoid sinus thrombosis, epidural/subdural empyema |
| 7 | Cochlea (rare, late) | Profound SNHL, suppurative labyrinthitis |
Key Points
Why the incus long process erodes first:
- It has the poorest blood supply among the ossicles, making it most susceptible to osteoclastic resorption. Pars flaccida cholesteatoma also directly contacts it as it expands medially.
Why the lateral SCC is the most common site of labyrinthine fistula:
- It protrudes furthest into the mastoid antrum and is directly in the path of a posteriorly expanding cholesteatoma. Labyrinthine fistula occurs in approximately 7-10% of cholesteatoma cases (K.J. Lee's Essential Otolaryngology).
Mechanisms of erosion (two distinct pathways):
- Direct pressure from the expanding cholesteatoma sac
- Enzymatic/inflammatory mediators from the cholesteatoma matrix (activated macrophages, monocytes, multinucleated osteoclasts) - Shambaugh Surgery of the Ear
Note on pars tensa cholesteatoma: These arise medial to the ossicular chain and tend to cause earlier erosion of inner ear structures (lateral SCC), while pars flaccida cholesteatomas tend to erode the ossicles first - Scott-Brown's Otorhinolaryngology, Vol 2
Imaging - Coronal CT of Right Lateral Epitympanic Cholesteatoma

Axial CT temporal bone - middle ear opacification with bone erosion. Early ossicular erosion is visible.
Complications Arising from Bone Erosion
- Conductive hearing loss - ossicular erosion (most common)
- Facial palsy - fallopian canal erosion
- Labyrinthine fistula - SNHL + vertigo
- Meningitis / brain abscess - tegmen erosion
- CSF otorrhea - tegmen erosion
- Sigmoid sinus thrombosis - posterior fossa plate erosion
Sources: Shambaugh Surgery of the Ear, p. 453 | Cummings Otolaryngology, p. 140 | K.J. Lee's Essential Otolaryngology, p. 453 | Scott-Brown's Otorhinolaryngology Vol 2, p. 1234
Attic cholestetaoma photo
Finding Sources
Searching the Web
attic cholesteatoma otoscopy clinical photo
Loading Image
Loading Image
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have three high-quality images from authoritative textbooks. Here is the complete answer:
Attic Cholesteatoma - Images & Clinical Features
Attic cholesteatoma arises from a pars flaccida retraction pocket in the Prussak space (lateral epitympanum). Keratin debris accumulates in the attic, and the hallmark on otoscopy is a crust or perforation in the attic (superior part of the tympanic membrane) - which can be easily missed if mistaken for wax.
1. CT Temporal Bone - Left Attic Cholesteatoma (Cummings Otolaryngology)
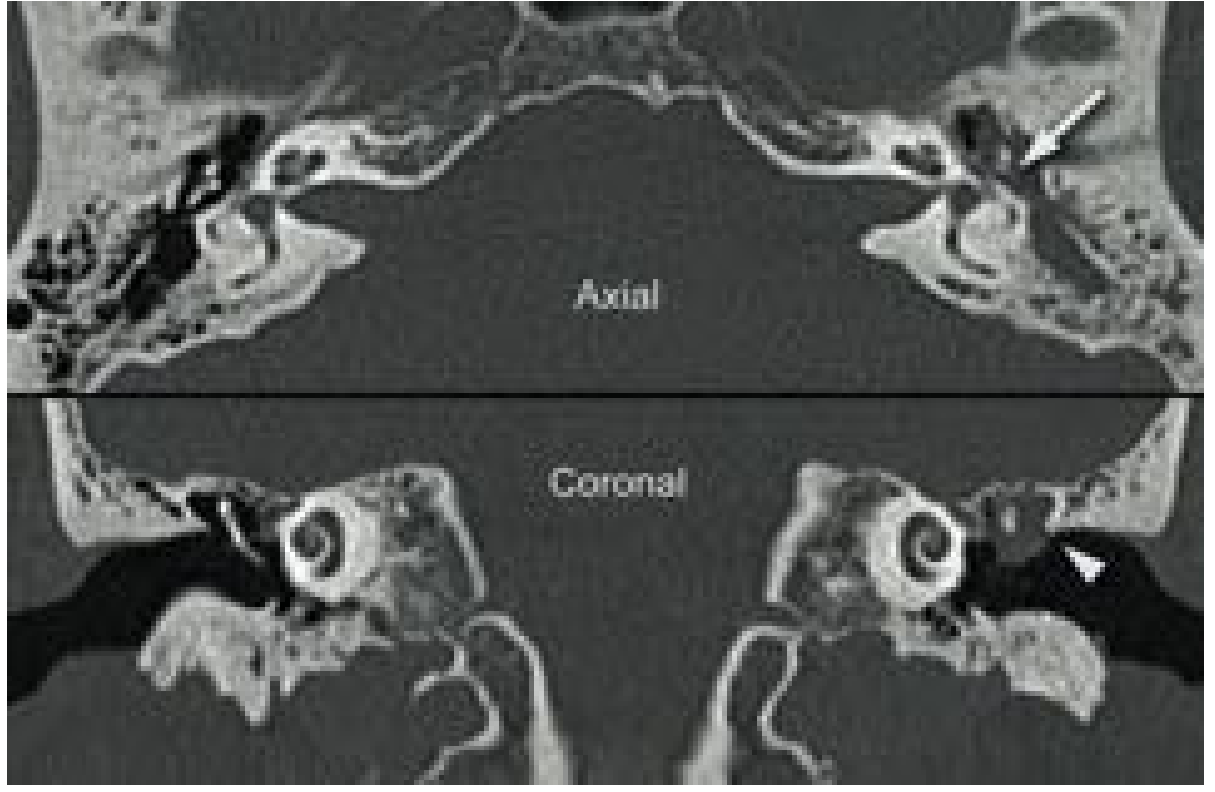
Axial (top) and Coronal (bottom) CT temporal bone - Left attic cholesteatoma. The white arrow points to the eroded incus; the arrowhead marks scutum erosion. Soft tissue opacification fills the epitympanum. - Cummings Otolaryngology, Fig. 140.10
2. Coronal CT - Right Pars Flaccida Cholesteatoma with Ossicular Erosion (Scott-Brown's)

Coronal CT temporal bone - 4 mm right lateral epitympanic pars flaccida cholesteatoma. The white arrow points to the soft tissue mass with early ossicular erosion in the attic. - Scott-Brown's Otorhinolaryngology Vol 2, Fig. 97.8
3. Histopathology - Active Squamous COM / Cholesteatoma (Scott-Brown's)
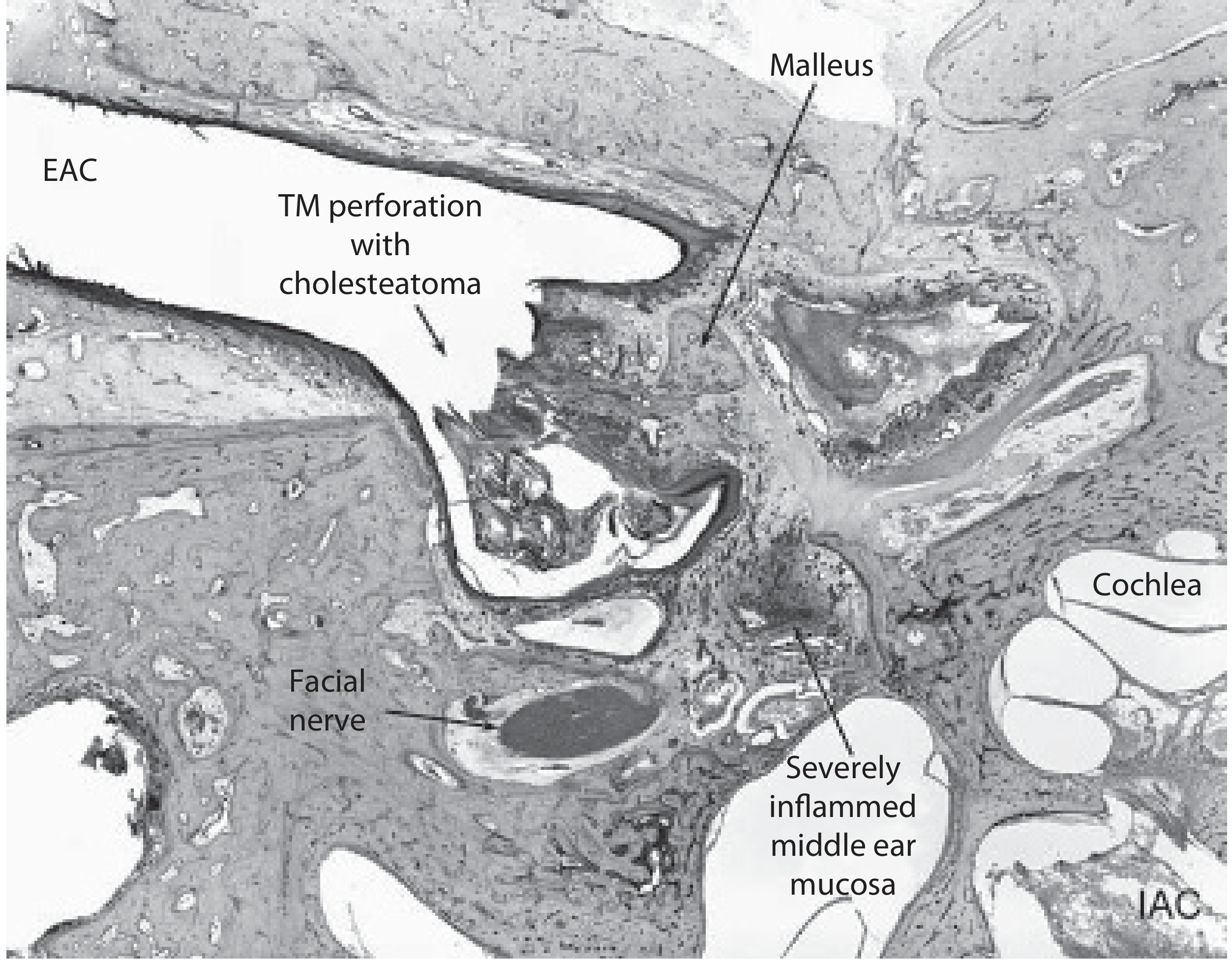
Axial temporal bone section (18-year-old female, ×8 magnification) showing:
- TM perforation with cholesteatoma - squamous epithelium growing through the pars tensa perforation into the middle ear
- Retained keratin within the cholesteatoma sac
- Severely inflamed middle ear mucosa surrounding the sac
- Proximity to the facial nerve and cochlea - Scott-Brown's Otorhinolaryngology Vol 2, Fig. 83.36
Key Otoscopic Features of Attic Cholesteatoma (to recognize clinically)
| Feature | Description |
|---|---|
| Attic crust/perforation | Crust or retraction pocket in the pars flaccida (superior TM), often mistaken for wax |
| Foul-smelling discharge | Characteristic keratin debris odour |
| Pars tensa | Often appears normal - a common reason the diagnosis is missed |
| Aural polyp | If protruding from the attic, assume cholesteatoma until proven otherwise |
| Scutum notch | Loss of the sharp bony overhang of the scutum visible on careful otoscopy |
"An attic or pars flaccida perforation (actually an invagination) always means a cholesteatoma." - Shambaugh Surgery of the Ear
Source: Cummings Otolaryngology | Scott-Brown's Otorhinolaryngology Vol 2 | Shambaugh Surgery of the Ear
Endoscopic photo of attic cholestetaoma
Finding Sources
Searching the Web
endoscopic otoscopy attic cholesteatoma clinical photo pars flaccida
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Reading File
I have all the images needed. Here is the complete answer with the textbook endoscopic photos:
Endoscopic Photos of Attic Cholesteatoma
All images below are from Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 2 (Figure 15.3 and 15.8).
Image 1 - Active Attic Cholesteatoma (Right Ear)
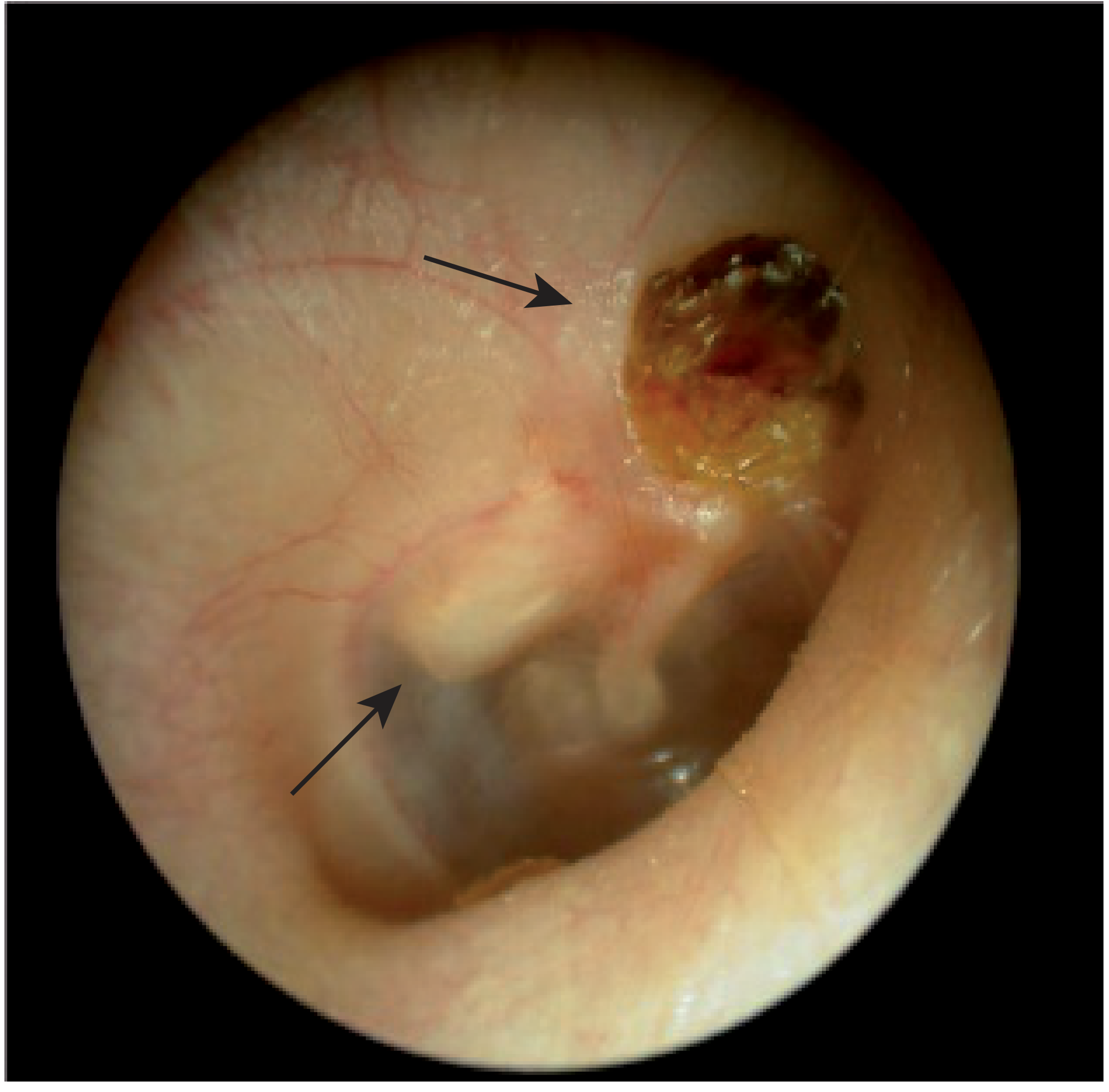
Figure 15.3 - Endoscopic photo of the right ear:
- Thick arrow (upper right) = Oxidized keratin of the cholesteatoma in the attic - the brown/amber crust of desquamated keratin debris, characteristic of attic cholesteatoma. This is what is seen in the superior (pars flaccida) region.
- Thin arrow (lower left) = Cholesteatoma sac extending into the posterior middle ear - visible as a grey-white pearlescent mass behind the tympanic membrane.
This is the classic endoscopic appearance: a crusted attic defect with a white/grey sac visible behind the drum.
Image 2 - Recurrent Attic Cholesteatoma Post-CWU Surgery (Right Ear)
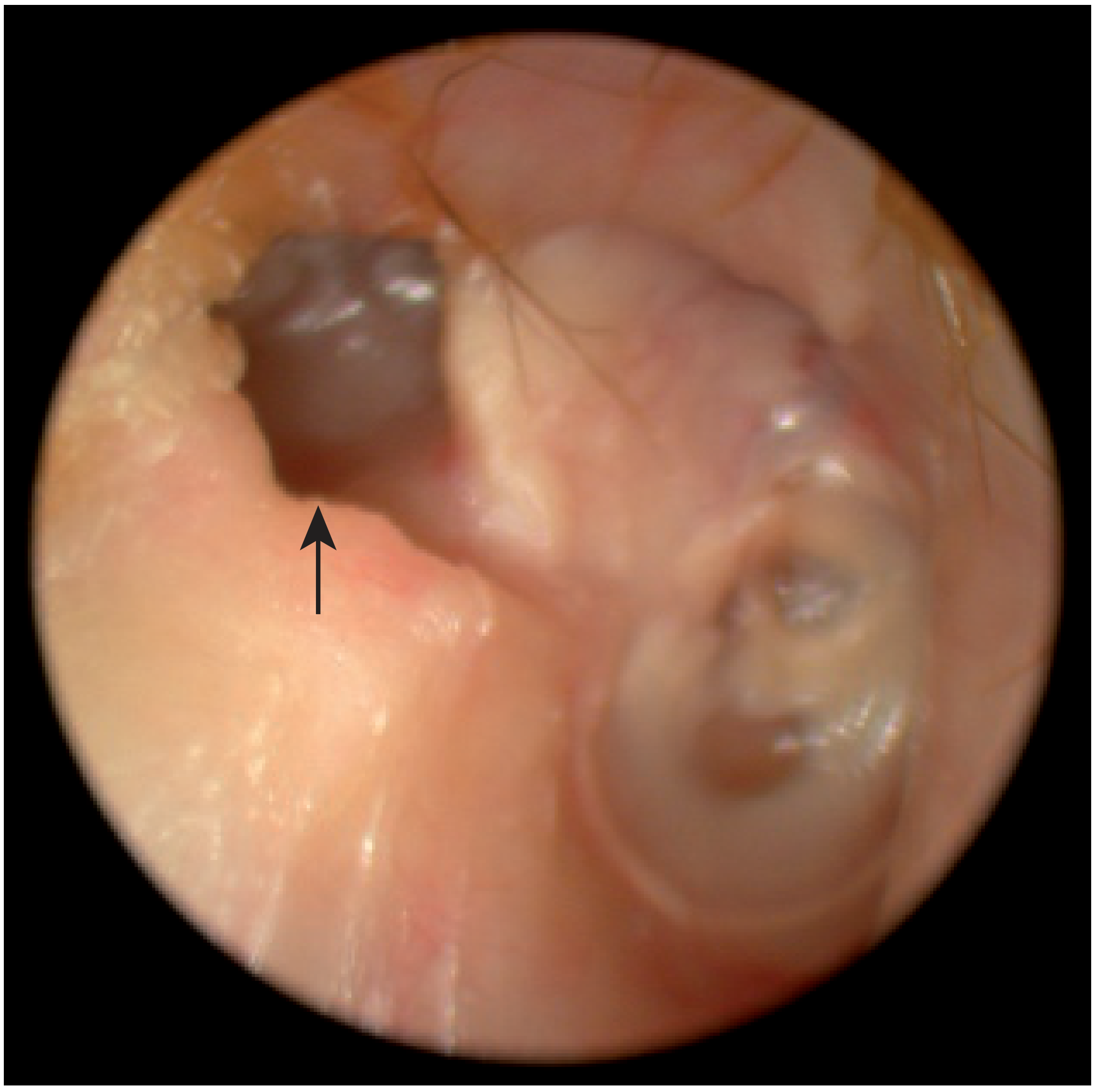
Figure 15.8 - Endoscopic photo of right ear years after canal wall up (CWU) surgery for attic cholesteatoma:
- The attic has been reconstructed with cartilage (visible as the white firm area in the superior canal)
- Arrow = Recurrent retraction cholesteatoma posterior to the cartilage graft - appears as a dark retraction pocket with the characteristic grey-white pearlescent surface
- Illustrates how cholesteatoma can recur even after surgical repair, driven by persistent Eustachian tube dysfunction
What to Look for Endoscopically in Attic Cholesteatoma
| Feature | Appearance |
|---|---|
| Attic crust | Brown/amber oxidized keratin in the pars flaccida region |
| Sac | White/grey pearlescent mass ("mother of pearl") |
| Scutum notch | Loss of the sharp bony lateral attic wall |
| Retraction pocket | Superior TM drawn inward, with debris trapped |
| Discharge | Foul-smelling, may partially obscure the view |
The superior part of the TM (pars flaccida) should always be specifically examined - the pars tensa often appears completely normal even when a significant attic cholesteatoma is present.
Source: Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 2, p. 202 - Figs. 15.3 & 15.8
Give endoscopic photo of attic retraction
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Excellent! I now have a rich set of high-quality clinical images from four authoritative textbooks. Here is the complete answer:
Endoscopic / Otoscopic Photos of Attic Retraction
Image 1 - Pars Flaccida Retraction Pocket (without cholesteatoma)
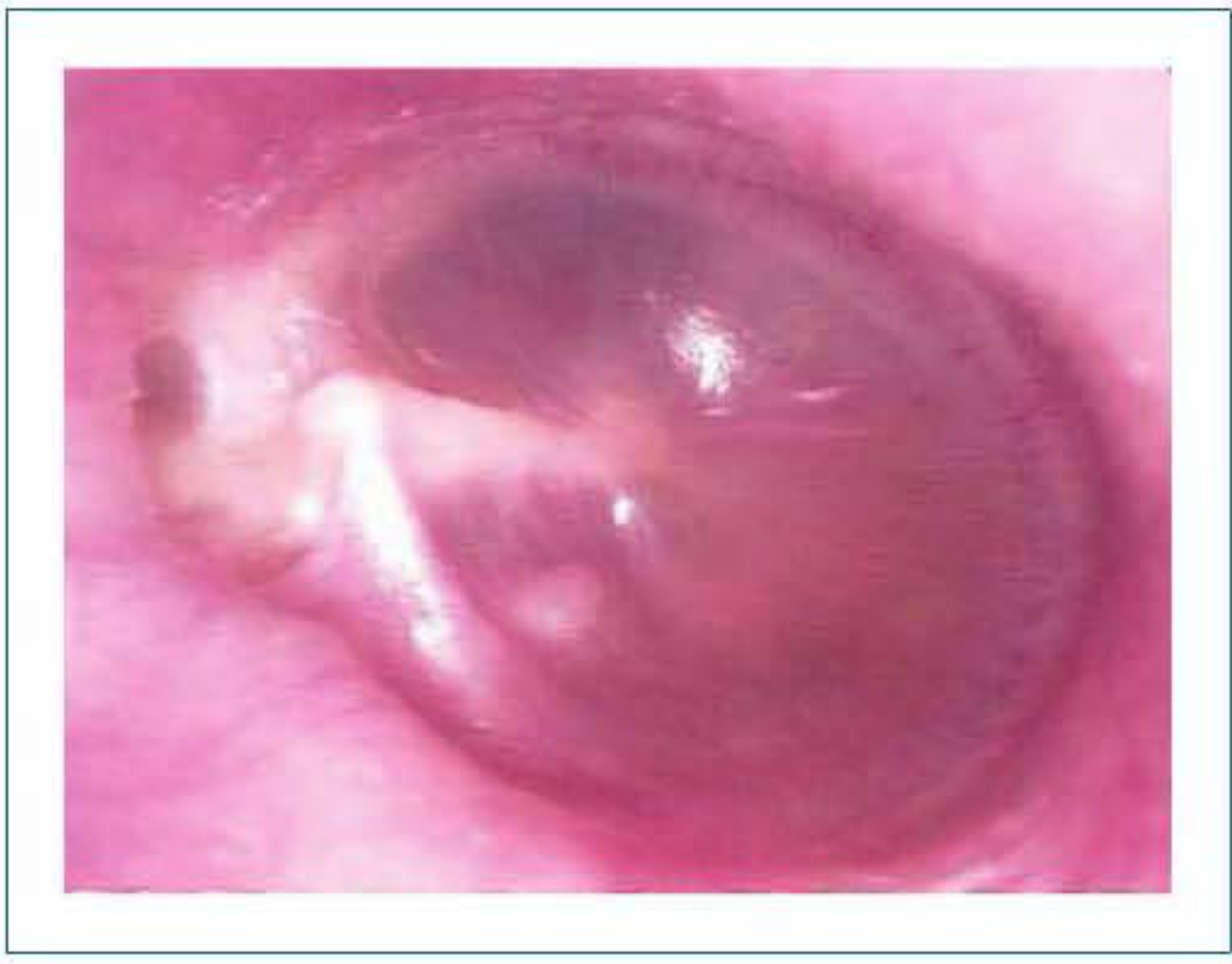
Pure attic retraction pocket (no cholesteatoma yet). The pars flaccida is retracted medially down onto the neck of the malleus (visible as the white handle-like structure) and onto the incudostapedial joint. The pars tensa appears otherwise normal and translucent. Importantly - no keratin debris is collecting, which distinguishes this from cholesteatoma.
Source: Shambaugh Surgery of the Ear, Fig. 25-9, p. 456
Image 2 - Attic Retraction with Established Cholesteatoma (Otoscopy + CT)
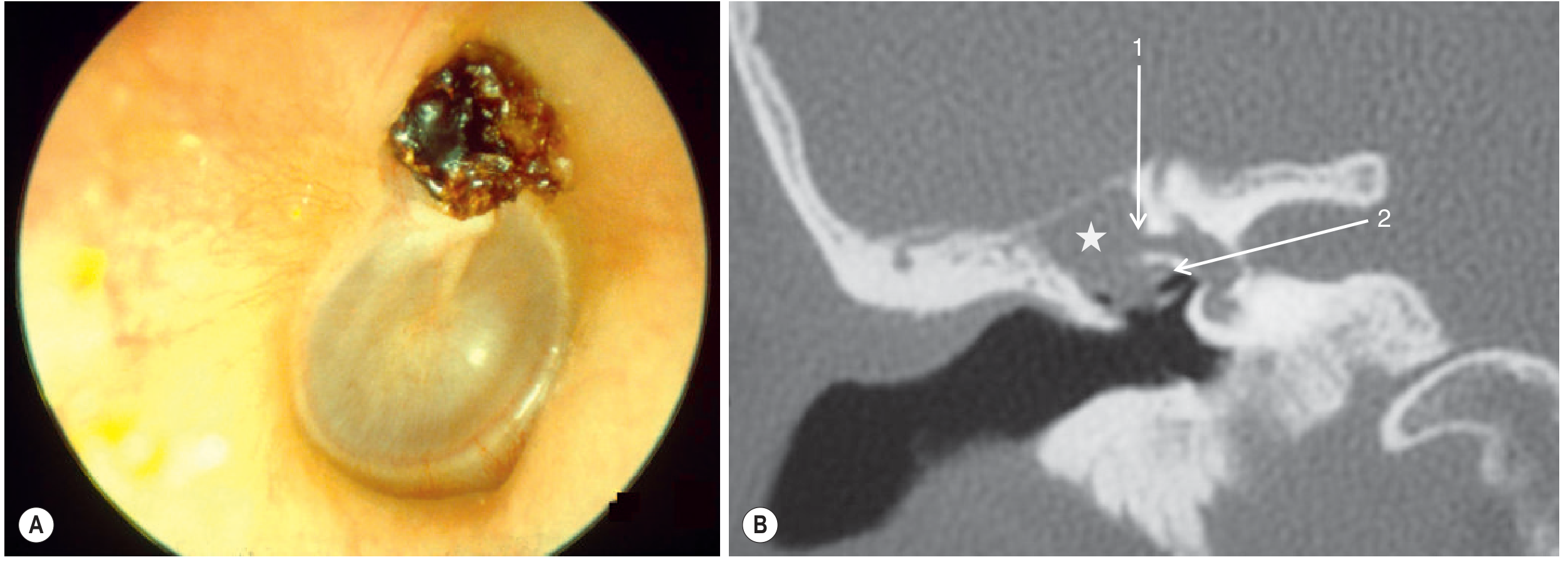
Panel A (left) - Otoscopic view: The dark brown/amber crust in the superior (attic / pars flaccida) region of the tympanic membrane is the classic appearance of a retraction pocket that has filled with oxidized keratin - this has now progressed to attic cholesteatoma. The pars tensa below remains intact and glistening.
Panel B (right) - Coronal CT: The star (★) marks the cholesteatoma in the attic. Arrow 1 = eroded otic capsule overlying the lateral semicircular canal (labyrinthine fistula). Arrow 2 = facial nerve (tympanic segment).
Source: Grainger & Allison's Diagnostic Radiology, Fig. 61.10, p. 1593
Image 3 - Posterior-Superior Retraction Pocket with Cholesteatoma (Surgical View)
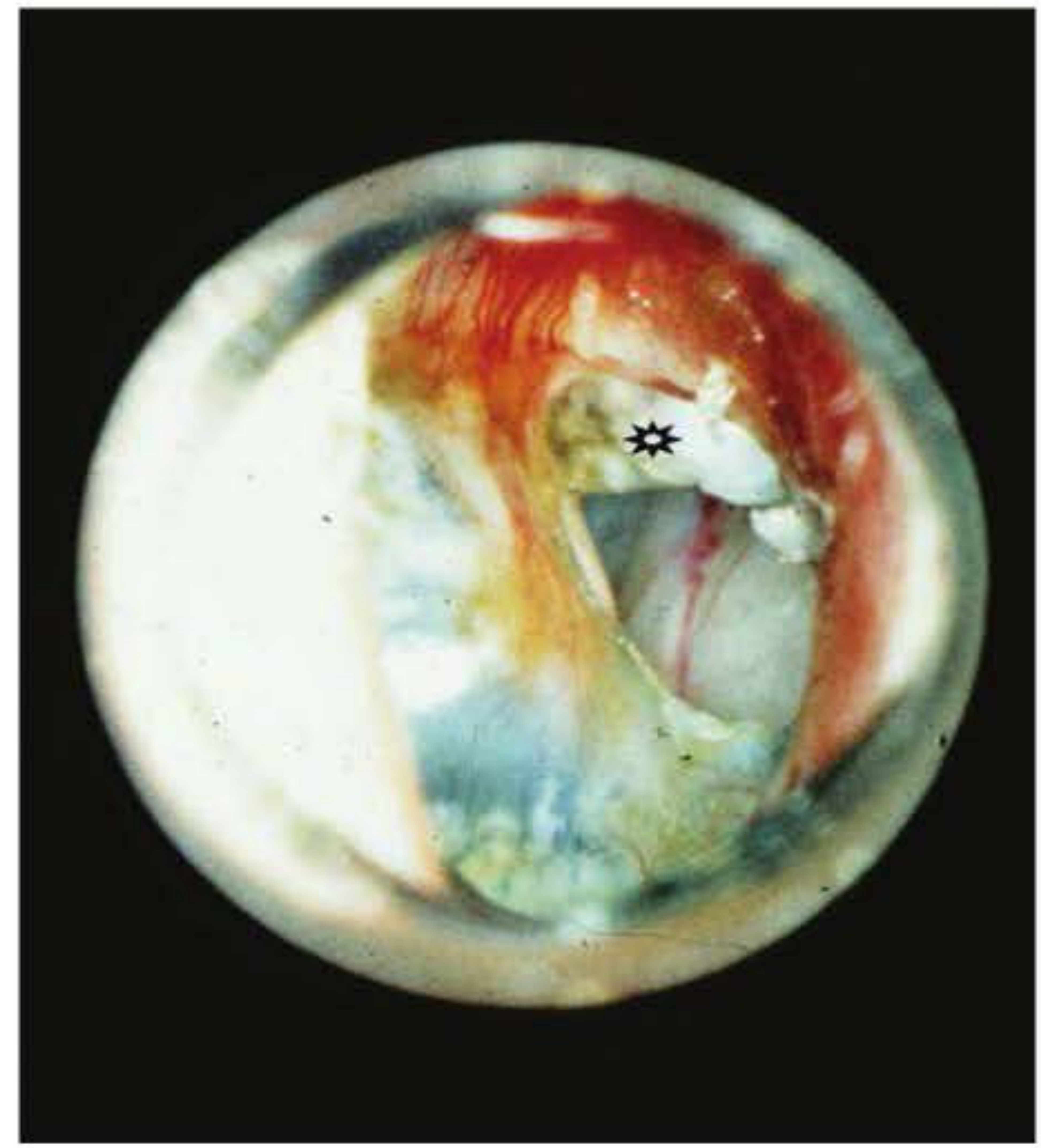
Posterior-superior quadrant retraction pocket with cholesteatoma (★). This is a more advanced view showing the retracted, inflamed TM with the white pearlescent cholesteatoma sac visible through the retraction. The granulation tissue and hyperaemia around the pocket indicate active disease.
Source: Shambaugh Surgery of the Ear, Fig. 26-11, p. 467 (Courtesy of Dr. Richard Buckingham)
Key Differences: Retraction Pocket vs Cholesteatoma
| Feature | Attic Retraction Pocket | Attic Cholesteatoma |
|---|---|---|
| TM appearance | Pars flaccida drawn inward | Pars flaccida defect / perforation |
| Debris | None - self-cleaning | Keratin debris present (brown/amber crust) |
| Mass | No sac | White "mother of pearl" sac |
| View depth | Fundus may or may not be visible | Usually extends beyond view |
| Management | Observe if self-cleaning; surgery if beyond view | Surgery always indicated |
Once a retraction pocket extends beyond clinical view, observation alone is deemed unwise as progression can go undetected - Shambaugh Surgery of the Ear, p. 456
This is a shared conversation. Sign in to Orris to start your own chat.