psychiatric disorders
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
Here is a comprehensive overview of the major categories of psychiatric disorders, drawing from Kaplan & Sadock's Synopsis of Psychiatry and the Comprehensive Textbook of Psychiatry.
Psychiatric Disorders: Overview of Major Categories
Classification Framework
Psychiatric disorders are classified using the Diagnostic and Statistical Manual of Mental Disorders (DSM), currently in its 5th edition (DSM-5-TR), published by the American Psychiatric Association. The DSM uses a purely descriptive, symptom-based approach — it defines disorders by their observable clinical features rather than presumed cause.
The parallel international system is the ICD-11 (WHO), which is used more widely outside North America.
Major DSM-5 Categories
1. Neurodevelopmental Disorders
Onset in early life; involve deficits in development of the brain and CNS.
- Intellectual Disability (ID) — deficits in intellectual and adaptive functioning
- Autism Spectrum Disorder (ASD) — impaired social communication, restricted/repetitive behaviors
- ADHD — inattention and/or hyperactivity-impulsivity
- Specific Learning Disorders — reading, writing, arithmetic
- Tic Disorders / Tourette's
2. Schizophrenia Spectrum & Other Psychotic Disorders
Characterized by positive symptoms (hallucinations, delusions, disorganized speech/behavior) and negative symptoms (flat affect, alogia, avolition).
- Schizophrenia — ≥6 months of symptoms; most severe and chronic
- Schizophreniform Disorder — 1–6 months
- Brief Psychotic Disorder — <1 month
- Schizoaffective Disorder — psychosis + mood episode
- Delusional Disorder — fixed, non-bizarre delusions without other psychotic features
African Americans and Latinos have been found to have over 3× higher odds of being diagnosed with schizophrenia compared to Whites — likely reflecting diagnostic bias and social determinants of health, not true biological difference. — Kaplan & Sadock's Comprehensive Textbook of Psychiatry
3. Bipolar & Related Disorders
Characterized by episodes of elevated or expansive mood.
- Bipolar I — at least one full manic episode (with or without depression)
- Bipolar II — hypomania + major depressive episodes (no full mania)
- Cyclothymic Disorder — chronic fluctuating hypomania and depressive symptoms for ≥2 years
4. Depressive Disorders
Defined by persistent low mood, anhedonia, and neurovegetative symptoms.
- Major Depressive Disorder (MDD) — ≥5 symptoms for ≥2 weeks including depressed mood or anhedonia
- Persistent Depressive Disorder (Dysthymia) — chronic low-grade depression ≥2 years
- Premenstrual Dysphoric Disorder (PMDD)
- Disruptive Mood Dysregulation Disorder (DMDD) — children with recurrent severe temper outbursts
5. Anxiety Disorders
Excessive fear (response to immediate threat) and anxiety (anticipation of future threat).
- Generalized Anxiety Disorder (GAD) — chronic, uncontrollable worry about multiple domains
- Panic Disorder — recurrent unexpected panic attacks + anticipatory anxiety
- Social Anxiety Disorder (Social Phobia)
- Specific Phobia
- Agoraphobia
- Separation Anxiety Disorder
6. Obsessive-Compulsive & Related Disorders (OCD Spectrum)
- OCD — intrusive obsessions + compulsive rituals to reduce distress
- Body Dysmorphic Disorder
- Hoarding Disorder
- Trichotillomania (hair-pulling)
- Excoriation Disorder (skin-picking)
7. Trauma- & Stressor-Related Disorders
- PTSD — re-experiencing, avoidance, negative cognitions, hyperarousal after trauma
- Acute Stress Disorder — similar to PTSD but lasting 3 days – 1 month
- Adjustment Disorders — emotional/behavioral symptoms in response to identifiable stressor
8. Dissociative Disorders
- Dissociative Identity Disorder (DID)
- Dissociative Amnesia
- Depersonalization/Derealization Disorder
9. Somatic Symptom & Related Disorders
- Somatic Symptom Disorder — excessive distress/preoccupation with physical symptoms
- Illness Anxiety Disorder (Hypochondriasis)
- Conversion Disorder (Functional Neurological Symptom Disorder)
10. Feeding & Eating Disorders
- Anorexia Nervosa — restriction + intense fear of gaining weight
- Bulimia Nervosa — binge-purge cycles
- Binge-Eating Disorder
- ARFID (Avoidant/Restrictive Food Intake Disorder)
11. Sleep-Wake Disorders
- Insomnia Disorder, Hypersomnolence, Narcolepsy, OSA, Parasomnias (REM sleep behavior disorder, sleepwalking), Circadian Rhythm disorders
12. Substance Use & Addictive Disorders
- Alcohol, cannabis, stimulant, opioid, sedative, hallucinogen, tobacco, gambling disorder
- Defined by impaired control, social impairment, risky use, and pharmacological criteria (tolerance, withdrawal)
13. Neurocognitive Disorders
- Delirium — acute, fluctuating disturbance in attention and cognition
- Major Neurocognitive Disorder (Dementia) — Alzheimer's, Lewy body, frontotemporal, vascular
- Mild Neurocognitive Disorder (MCI)
14. Personality Disorders
Enduring, inflexible patterns of inner experience and behavior deviating from cultural norms, causing distress or impairment. Grouped into three clusters:
| Cluster | Character | Disorders |
|---|---|---|
| A — "Odd/Eccentric" | Distorted thinking | Paranoid, Schizoid, Schizotypal |
| B — "Dramatic/Erratic" | Emotional dysregulation | Antisocial, Borderline, Histrionic, Narcissistic |
| C — "Anxious/Fearful" | Anxiety-driven | Avoidant, Dependent, Obsessive-Compulsive |
15. Other Notable Categories
- Paraphilic Disorders (Voyeuristic, Exhibitionistic, Pedophilic, etc.)
- Disruptive, Impulse-Control & Conduct Disorders (ODD, Conduct Disorder, Intermittent Explosive Disorder, Pyromania, Kleptomania)
- Gender Dysphoria
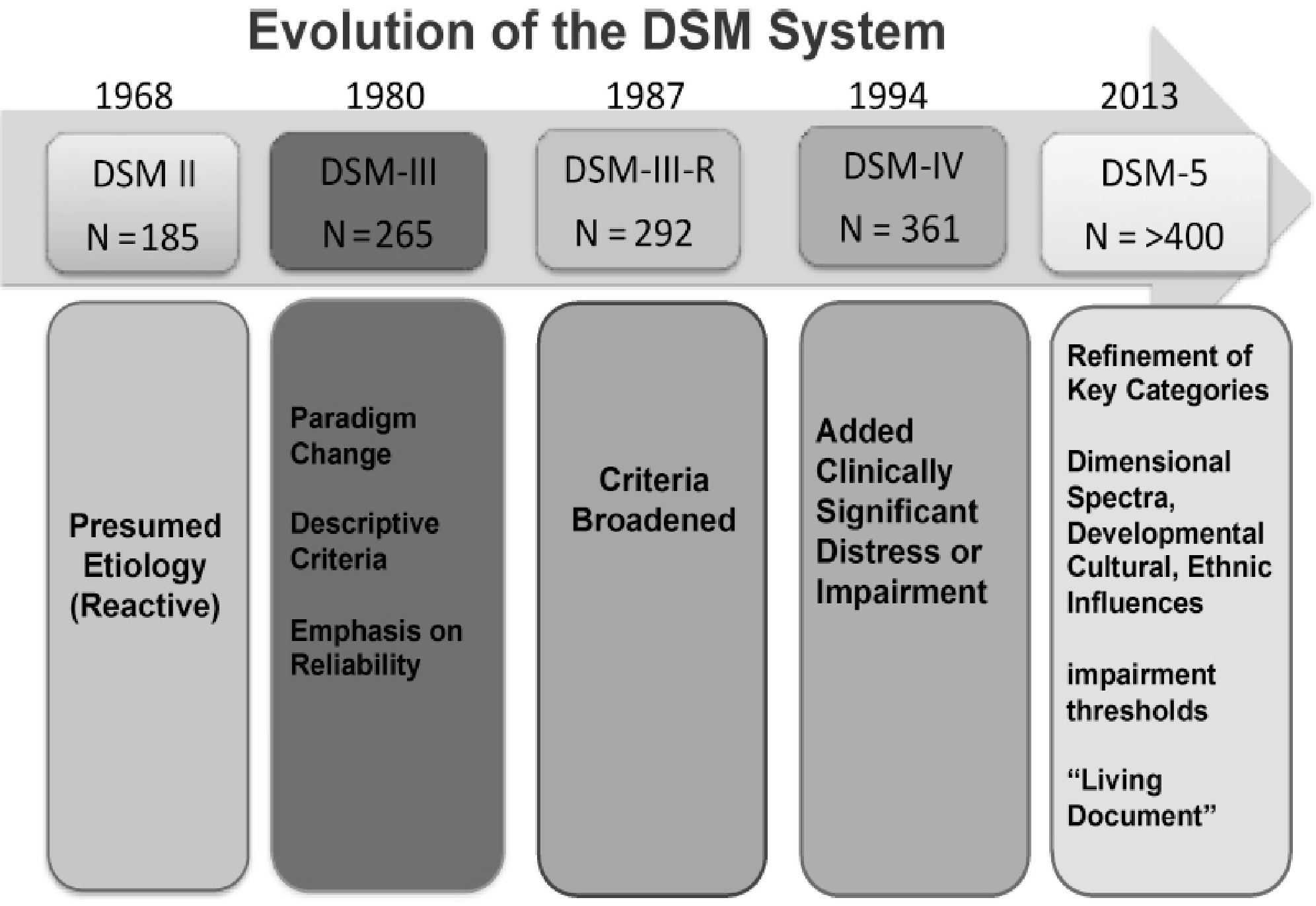
Key Historical Context
The DSM-III (1980) was a turning point — it eliminated assumed etiology and introduced symptom-based, operationalized criteria for reliability. This enabled rigorous clinical research and the predominance of CBT and pharmacotherapy as evidence-based treatments. DSM-5 (2013) added dimensional spectra, cross-cutting symptom measures, and cultural/developmental sensitivity.
"Most psychiatric disorders are very complex disorders that require multifaceted solutions... including attention to psychosocial treatments as well as pharmacologic." — Kaplan & Sadock's Synopsis of Psychiatry
Would you like a deeper dive into any specific category — its diagnosis, neurobiology, or treatment?
This is a shared conversation. Sign in to Orris to start your own chat.