Enumerate the phvsiological changes during 1st stage Iabour.
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have rich, comprehensive data from multiple authoritative textbooks. Let me compile the complete answer.
Physiological Changes During the 1st Stage of Labour
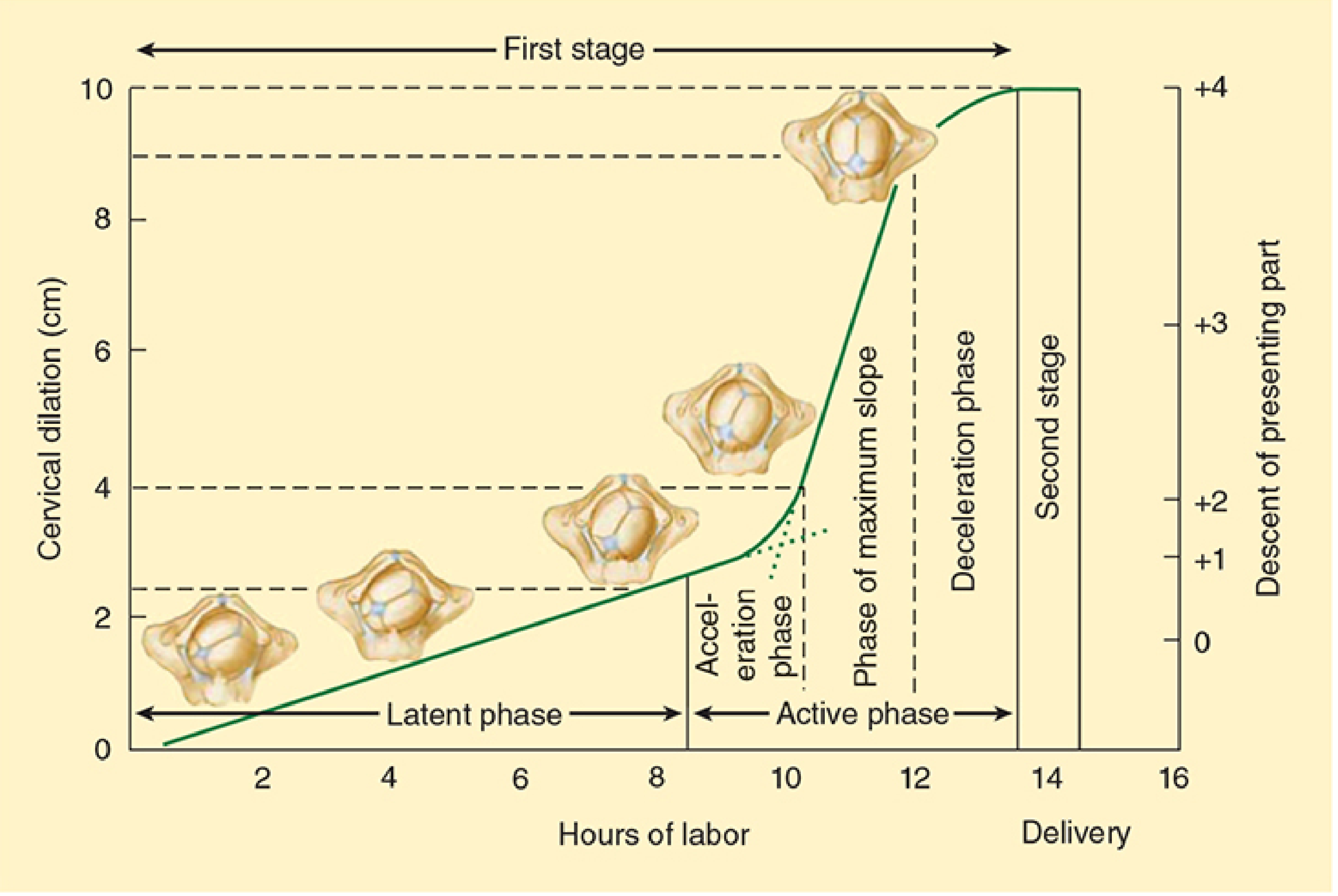
The first stage of labour begins with the onset of true (regular, painful) uterine contractions and ends when the cervix is fully dilated to 10 cm. It is divided into two phases:
I. Uterine Changes
A. Uterine Contractions
- True labour begins when irregular Braxton Hicks contractions become coordinated, rhythmic, and progressive in strength and frequency.
- Early first stage (latent phase): contractions every 15-30 minutes, mild intensity (~25 mm Hg).
- As labour advances (active phase): contractions increase to every 3-5 minutes, with intensities of 25-60 mm Hg, and duration of 30-60 seconds.
- Contractions originate at the fundus and spread downward - the fundus and body contract strongly while the lower uterine segment remains relatively passive.
- Combined uterine and (later) abdominal muscular forces generate ~25 pounds of downward pressure per strong contraction on the fetus.
- Contractions are intermittent by necessity - continuous strong contractions would impede placental blood flow and cause fetal compromise. - Guyton & Hall Textbook of Medical Physiology
B. Lower Uterine Segment Formation
- The lower uterine segment (isthmus) progressively thins and stretches as labour advances.
- A physiological retraction ring (Bandl's ring) may be felt between the thicker upper segment and the thinner lower segment.
C. Uterine Blood Flow
- Each contraction transiently reduces uteroplacental blood flow. Recovery occurs during the relaxation interval - this is why adequate inter-contraction intervals are physiologically essential.
II. Cervical Changes
A. Effacement (Cervical Ripening)
- Preceded by cervical softening weeks before labour onset - mediated by inflammatory cells (neutrophil infiltration) and local cytokines causing collagen remodelling and water content increase.
- The cervix shortens (effaces) from a thick, closed tube ~3-4 cm long to a paper-thin, flush structure.
- In nulliparas: effacement precedes dilation. In multiparas: they may occur simultaneously.
B. Dilation
- Latent phase: slow progressive effacement and minor dilation up to 4-6 cm over 6-12 hours (nullipara up to 20 hours is still considered normal). - Miller's Anesthesia
- Active phase: rapid dilation from 6 cm to 10 cm (or classically from 4 cm in older Friedman's model). Dilation rate in active phase should be at least 1-1.2 cm/hour in nulliparas and 1.5 cm/hour in multiparas.
- The full transition marks the end of the first stage. Typically, first stage lasts 8-12 hours in nulliparas and 5-8 hours in multiparas. - Morgan & Mikhail's Clinical Anesthesiology
III. Fetal Descent
- During the first stage, the presenting part (usually vertex) engages in and descends through the pelvis.
- The head acts as a wedge, progressively dilating the birth canal.
- Fetal station (level of presenting part relative to ischial spines) advances during the active phase.
IV. Membrane Changes
- The intact fetal membranes form a "forewaters" bag that transmits hydrostatic pressure evenly to help dilate the cervix.
- Membranes may rupture spontaneously (SROM) before or during the first stage - when this occurs, the amniotic fluid is lost and the fetal head directly presses on the cervix (more efficient pressure transmission).
V. Maternal Cardiovascular Changes
- Each uterine contraction displaces 300-500 mL of blood from the uterus into the central circulation, acting like an autotransfusion.
- Cardiac output rises approximately 45% above third-trimester baseline during active labour.
- Heart rate and blood pressure rise slightly with each painful contraction.
- The greatest cardiovascular strain occurs immediately after delivery (not during the first stage), when uterine involution relieves IVC compression and cardiac output rises 80% above third-trimester values. - Morgan & Mikhail's Clinical Anesthesiology
VI. Maternal Respiratory Changes
- Pain and anxiety during contractions cause maternal hyperventilation.
- Minute ventilation may increase by up to 300% during intense contractions.
- Oxygen consumption rises by ~60% above third-trimester values.
- Excessive hyperventilation can drive PaCO2 below 20 mm Hg, causing maternal and fetal hypoxaemia between contractions, reduced uterine blood flow, and fetal acidosis. - Morgan & Mikhail's Clinical Anesthesiology
VII. Pain Pathways During the First Stage
- Pain arises from myometrial hypoxia during contractions, progressive cervical dilation, and stretching of the lower uterine segment.
- The first stage produces predominantly visceral pain, carried by afferent fibres travelling with sympathetic nerves via the uterovaginal plexus -> inferior hypogastric plexus -> T10-L1 spinal roots.
- Latent phase: pain referred to T11-T12 dermatomes (lower abdomen, suprapubic).
- Active phase: pain expands to T10-L1 dermatomes, and is increasingly referred to the lumbosacral area, gluteal region, and thighs.
- Pain intensity correlates with cervical dilation and contraction frequency/intensity. Nulliparas typically experience greater first-stage pain than multiparas.
- At the end of the first stage, onset of perineal pain signals the beginning of fetal descent (transition to second stage). - Morgan & Mikhail's Clinical Anesthesiology
VIII. Hormonal and Biochemical Changes
- Oxytocin receptor upregulation: even though circulating oxytocin levels may not rise markedly at the onset of labour, the number of myometrial oxytocin receptors rapidly increases, sensitising the uterus.
- Prostaglandins (PGE2, PGF2α): synthesised by fetal membranes and decidual tissues, they enhance myometrial contractility and promote cervical ripening.
- Progesterone withdrawal (functional): reduced progesterone dominance allows pro-contractile pathways to predominate.
- Cortisol and fetal adrenal steroids: contribute to the initiation of labour signalling.
- Catecholamines: maternal stress and pain elevate adrenaline/noradrenaline, which can reduce uterine blood flow. - Morgan & Mikhail's Clinical Anesthesiology
IX. Prodromal Events Preceding True Labour (0-4 weeks before)
| Event | Timing |
|---|---|
| Lightening (fetal head engaging) | 2-4 weeks before (nullipara) |
| Increased Braxton Hicks frequency | Last few weeks |
| Cervical softening and effacement | Last 1-2 weeks |
| Bloody show (mucous plug expulsion) | 1 week to 1 hour before true labour |
Summary Table: Latent vs Active Phase of First Stage
| Feature | Latent Phase | Active Phase |
|---|---|---|
| Cervical dilation | 0 to 4-6 cm | 6 to 10 cm |
| Contraction frequency | Every 15-20 min | Every 3-5 min |
| Contraction intensity | Mild (~25 mm Hg) | Moderate-strong (25-60 mm Hg) |
| Rate of dilation | Slow | Rapid (>1 cm/hr) |
| Duration (nullipara) | Up to 14-20 hrs | 4-6 hrs |
| Pain distribution | T11-T12 | T10-L1 |
Sources: Guyton & Hall Textbook of Medical Physiology; Morgan & Mikhail's Clinical Anesthesiology, 7e; Miller's Anesthesia, 10e; Creasy & Resnik's Maternal-Fetal Medicine.
This is a shared conversation. Sign in to Orris to start your own chat.