Advances in design of modern ultrasound transducers in detail
ultrasound transducer design advances
modern ultrasound transducer technology advances 2024 2025 CMUT PMUT matrix array
advances ultrasound transducer CMUT PMUT design fabrication wearable
matrix array transducer 3D ultrasound beamforming
Advances in the Design of Modern Ultrasound Transducers
1. Fundamental Architecture (Classical Baseline)
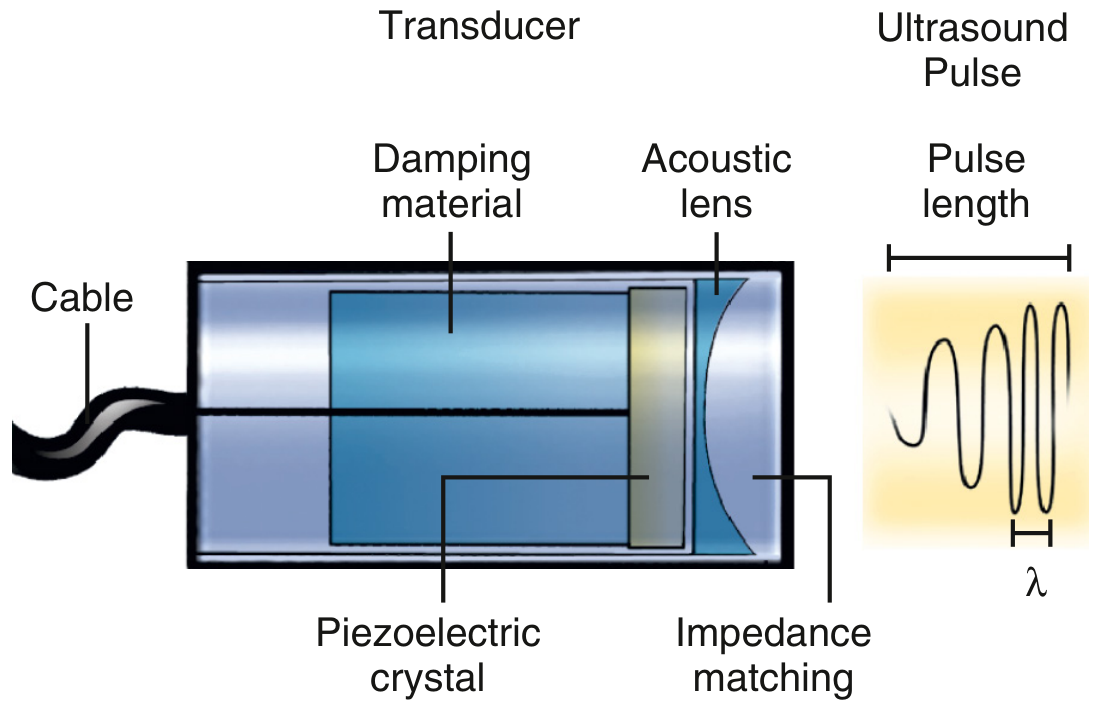
- Piezoelectric crystal: converts electrical current → mechanical compression (transmit) and pressure wave → electrical signal (receive). Common materials: lead zirconate titanate (PZT), barium titanate, quartz.
- Damping (backing) material: absorbs rearward energy; shortens pulse length → improves axial resolution.
- Acoustic lens: converges the beam to a focal zone.
- Impedance matching layer: λ/4-thick layer that reduces acoustic mismatch between the crystal (~30 MRayl) and soft tissue (~1.5 MRayl), maximizing energy transfer.
- Frequency: determined by crystal thickness — thinner crystal = higher frequency. Higher frequency = better resolution, less penetration. Clinical range: 2.5 MHz (cardiac TTE) to ≥20 MHz (intravascular).
- Bandwidth: range of frequencies in the pulse; wider bandwidth = better axial resolution and better reception of harmonic frequencies. — Textbook of Clinical Echocardiography
2. Array Architectures
Linear & Phased Arrays
1.5D Arrays
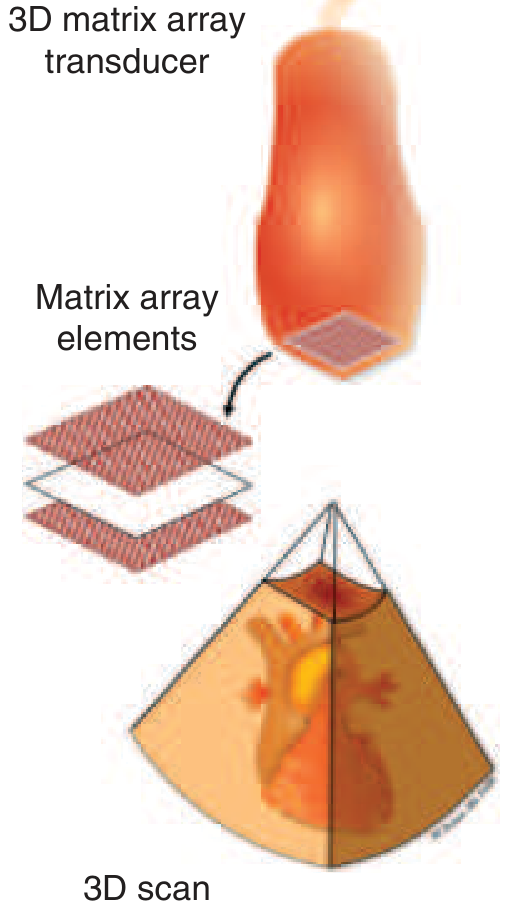
Full 2D Matrix Arrays (for 3D imaging)
3. Micromachined Ultrasound Transducers (MUTs)
- Batch (wafer-scale) fabrication → dramatically lower cost
- Integration with CMOS electronics on the same chip
- High element density — 2D arrays with pitches as small as 20 µm
- Miniaturization for catheter-based and wearable applications
- High-frequency operation (tens of MHz for IVUS)
a. Capacitive Micromachined Ultrasound Transducers (CMUTs)
- Exceptional bandwidth (up to 175%), enabling broadband imaging and multi-frequency operation
- High electromechanical coupling (kT² ~0.85 at optimal bias)
- Wide dynamic range
- CMOS-compatible → on-chip signal processing and beamforming
- Require large DC bias near "collapse voltage" (risk of membrane failure)
- Separate cavity heights may be needed for transmit vs. receive
- CMUT fabrication uses either sacrificial layer release (etch away a sacrificial material to form the air gap) or wafer bonding (bond a pre-thinned silicon wafer over a patterned cavity)
b. Piezoelectric Micromachined Ultrasound Transducers (PMUTs)
- No DC bias required (simpler drive electronics, safer)
- Operate on standard CMOS-compatible low voltages
- Flexible substrate compatibility for wearable/conformable devices
- Mass-producible via standard photolithography
- PZT (Lead zirconate titanate): highest coupling coefficients, but lead-based (environmental concern)
- AlN (Aluminum nitride): CMOS-compatible, lead-free, moderate coupling
- ScAlN (Scandium-doped AlN): significantly higher piezoelectric response than AlN, emerging standard
- ZnO: biocompatible, used in flexible devices
4. Bandwidth and Broadband Design
- Matching layer optimization: multiple λ/4 matching layers between crystal and tissue, reducing acoustic impedance mismatch
- Composite piezoelectrics (1-3 composites): PZT pillars embedded in polymer matrices — reduces lateral coupling, lowers acoustic impedance, broadens bandwidth
- Heavy damping backing: sacrifices sensitivity but greatly shortens pulse and broadens bandwidth
- Apodization: applying non-uniform voltage weighting across array elements to reduce side-lobe artifacts
5. High-Frequency and Intravascular Transducers (IVUS)
- Transducer diameter: ≤1 mm (to fit within 3–3.5 Fr catheters)
- Very high frequency: 40–60 MHz for atherosclerotic plaque characterization
- Single-element rotating design (mechanical) or solid-state phased array
- PVDF (polyvinylidene fluoride) and P(VDF-TrFE) polymer transducers — better acoustic impedance match to tissue, high-frequency response, flexible
- PMN-PT and PIN-PMN-PT single crystal piezoelectrics — higher coupling coefficients than PZT for superior sensitivity at small apertures
- CMUT-IVUS catheters — forward-looking (not just side-viewing) imaging of vessel bifurcations; improved bandwidth for multimodality integration
- IVUS + OCT hybrid catheters — co-registered optical coherence tomography and ultrasound on the same catheter — Peng et al., Sensors 2021 [PMID: 34069613]
6. Conformable and Wearable Transducers
- Substrate: polyimide, PDMS, or other polymer films replace rigid PCBs
- Active layer: PZT thin films, PVDF, or flexible PMUT membranes on polymer substrates
- Interconnects: serpentine copper traces allow stretching without fracture
- Fabrication: spin-coating piezoelectric films on flexible substrates; laser lift-off for substrate release; ICP-CVD silicon nitride structural layers
7. ASIC Integration and On-Chip Beamforming
- Micro-beamforming ASICs: custom integrated circuits placed immediately behind the transducer array (in the probe head) perform partial beamforming on subgroups of elements, reducing the cable count from thousands to tens
- CMUT/PMUT + CMOS monolithic integration: transducer fabricated directly on top of CMOS read-out circuitry, minimizing parasitic capacitance and maximizing sensitivity
- Deep learning beamforming: neural networks replace delay-and-sum algorithms to reconstruct images from sparse receive data, enabling high-frame-rate 3D imaging at reduced channel count (PMID: 36253231)
- Row-column addressed (RCA) arrays: instead of N×N individual element addressing, only N+N connections needed — drastically simplifying wiring while retaining volumetric imaging capability
8. Advanced Acoustic Design Features
| Feature | Mechanism | Clinical Benefit |
|---|---|---|
| Acoustic lens | Converges near-field beam | Fixed focal zone |
| Electronic multi-focus | Sequential transmissions at different focal depths | Improved lateral resolution across depth |
| Dynamic receive focusing | Continuously adjusts receive focus as echoes return | Near-optimal lateral resolution at all depths |
| Apodization | Tapered element weighting | Reduced side lobes, fewer artifacts |
| Coded excitation | Chirp/Golay sequences instead of single pulses | Higher SNR, deeper penetration, or lower output power |
| Diverging wave / plane wave transmit | Full aperture unfocused transmission | Ultrafast imaging (>10,000 frames/sec) enabling shear wave elastography and ultrasound localization microscopy |
9. Specialized Transducer Types
| Transducer | Frequency Range | Design Specifics |
|---|---|---|
| Adult TTE (transthoracic echo) | 2–5 MHz | Phased array, small footprint for intercostal access |
| TEE (transesophageal echo) | 5–7 MHz | Miniaturized array on flexible endoscope tip |
| Intracardiac echo (ICE) | 5–10 MHz | Array on 8–10 Fr catheter; rotational or phased array |
| IVUS | 20–60 MHz | Single element rotational or solid-state array on coronary catheter |
| Vascular / linear array | 5–15 MHz | Flat array for near-surface structures |
| Endocavitary (transvaginal, transrectal) | 5–10 MHz | Curved array, small probe diameter |
| High-frequency small-parts | 12–20 MHz | Linear array, thyroid, skin, superficial masses |
| Intraoperative 3D TEE | 5–7 MHz | Full matrix array in miniaturized TEE scope |
10. Emerging and Future Directions
- Single-crystal piezoelectrics (PMN-PT, PIN-PMN-PT): electromechanical coupling kT ≥ 0.9, enabling high-sensitivity transducers with bandwidth exceeding 100%
- Lead-free piezoelectrics: KNN (potassium sodium niobate), BaTiO₃-based — driven by RoHS environmental regulations
- Large-area PMUT arrays on display-compatible processes: imec's 4×4 cm² arrays point toward ultrasound imaging patches worn like a band-aid
- Volumetric ultrasound localization microscopy (vULM): matrix array transducers performing super-resolution vascular imaging by tracking individual microbubbles in 3D — resolution below the diffraction limit (PMID: 39453807)
- Internet-of-Medical-Things (IoMT) integration: wearable USoP patches transmitting continuous hemodynamic data wirelessly
- Photoacoustic ultrasound hybrids: same transducer receives both ultrasound echoes and laser-excited photoacoustic signals for simultaneous anatomical + molecular imaging
- AI-assisted adaptive beamforming: neural networks optimizing transmit sequences in real time based on tissue characteristics
Key References
- Textbook of Clinical Echocardiography — Piezoelectric Crystal, Types of Transducers, Beam Shape and Focusing
- Harrison's Principles of Internal Medicine 22E — Echocardiography, 3D matrix array transducer
- Miller's Anesthesia 10e — Harmonic Imaging, 3D Image Acquisition, Matrix Array
- Fuster & Hurst's The Heart 15e — Three-Dimensional Echocardiography
- He Y et al. Piezoelectric Micromachined Ultrasound Transducer Technology. Biosensors 2022 [PMID: 36671890]
- Herickhoff CD & van Schaijk R. cMUT technology developments. Z Med Phys 2023 [PMID: 37316428]
- Zhang L et al. Conformable Ultrasound Electronics. Adv Mater 2024 [PMID: 37792426]
- Lin M et al. Wearable ultrasound system-on-patch. Nat Biotechnol 2024 [PMID: 37217752]
- Peng C et al. Advances in IVUS Transducers. Sensors 2021 [PMID: 34069613]
- Denis L et al. Volumetric Ultrasound Localization Microscopy. IEEE TUFFC 2024 [PMID: 39453807]
Doppler spectral analysis and display in detail , give me in such a way in gain full marks in exam as msc student
Doppler spectral analysis ultrasound FFT spectral broadening aliasing MSc medical physics
Doppler spectral analysis FFT display aliasing spectral broadening waveform indices
Doppler spectral waveform display aliasing pulsed wave continuous wave
Doppler Spectral Analysis and Display — Complete MSc Exam Guide
SECTION 1: THE DOPPLER EFFECT — Fundamental Physics
1.1 The Doppler Principle
1.2 The Doppler Equation
| Symbol | Meaning |
|---|---|
| $f_d$ | Doppler frequency shift (Hz) |
| $f_0$ | Transmitted ultrasound frequency (Hz) |
| $v$ | Velocity of the moving target (blood) (m/s) |
| $\theta$ | Angle between ultrasound beam and direction of flow |
| $c$ | Speed of sound in tissue ≈ 1540 m/s |
| Factor of 2 | Because the beam travels to and from the moving target |
1.3 Angle Dependence — Critical Exam Point
| Angle θ | cos θ | Effect |
|---|---|---|
| 0° (parallel) | 1.0 | Maximum Doppler shift; ideal |
| 20° | 0.94 | 6% underestimation — clinically acceptable |
| 45° | 0.71 | 29% underestimation |
| 60° | 0.50 | 50% underestimation — maximum acceptable clinical angle |
| 90° (perpendicular) | 0 | Zero Doppler shift — no velocity can be measured |
Exam rule: Always use θ ≤ 60°. The empirical method to ensure near-parallel alignment is to examine from multiple acoustic windows and use the highest measured velocity as the closest to true (i.e., most parallel alignment). — Textbook of Clinical Echocardiography
SECTION 2: GENERATING THE SPECTRAL DISPLAY
2.1 The Fast Fourier Transform (FFT)
- Input: A short time window of the received Doppler signal (typically 5–10 ms)
- Output: The amplitude (power) at each frequency within that window
- Display: A single vertical column of the spectrogram at that time point
2.2 The Spectral Display — Axes and Conventions
VELOCITY
(m/s or cm/s)
↑
| ████ ████ ← Flow TOWARD transducer (positive)
| ████ ████
|────────────────────────────────── BASELINE (zero velocity)
|
| ▓▓▓▓ ▓▓▓▓ ← Flow AWAY from transducer (negative)
|
└────────────────────────────────── TIME (seconds)
| Display Element | Meaning |
|---|---|
| Y-axis | Velocity (m/s or cm/s) — proportional to frequency shift after angle correction |
| X-axis | Time, scrolling left to right; ECG trace usually displayed simultaneously |
| Above baseline | Flow toward transducer (positive Doppler shift) |
| Below baseline | Flow away from transducer (negative Doppler shift) |
| Brightness (grayscale) | Amplitude (power/intensity) of the Doppler signal — proportional to the number of RBCs moving at that velocity at that instant |
| Spectral envelope | Outer edge of the brightest signals = peak (maximum) velocity |
| Spectral window | Clear area beneath the peak velocity envelope in laminar flow |
SECTION 3: TYPES OF SPECTRAL DOPPLER
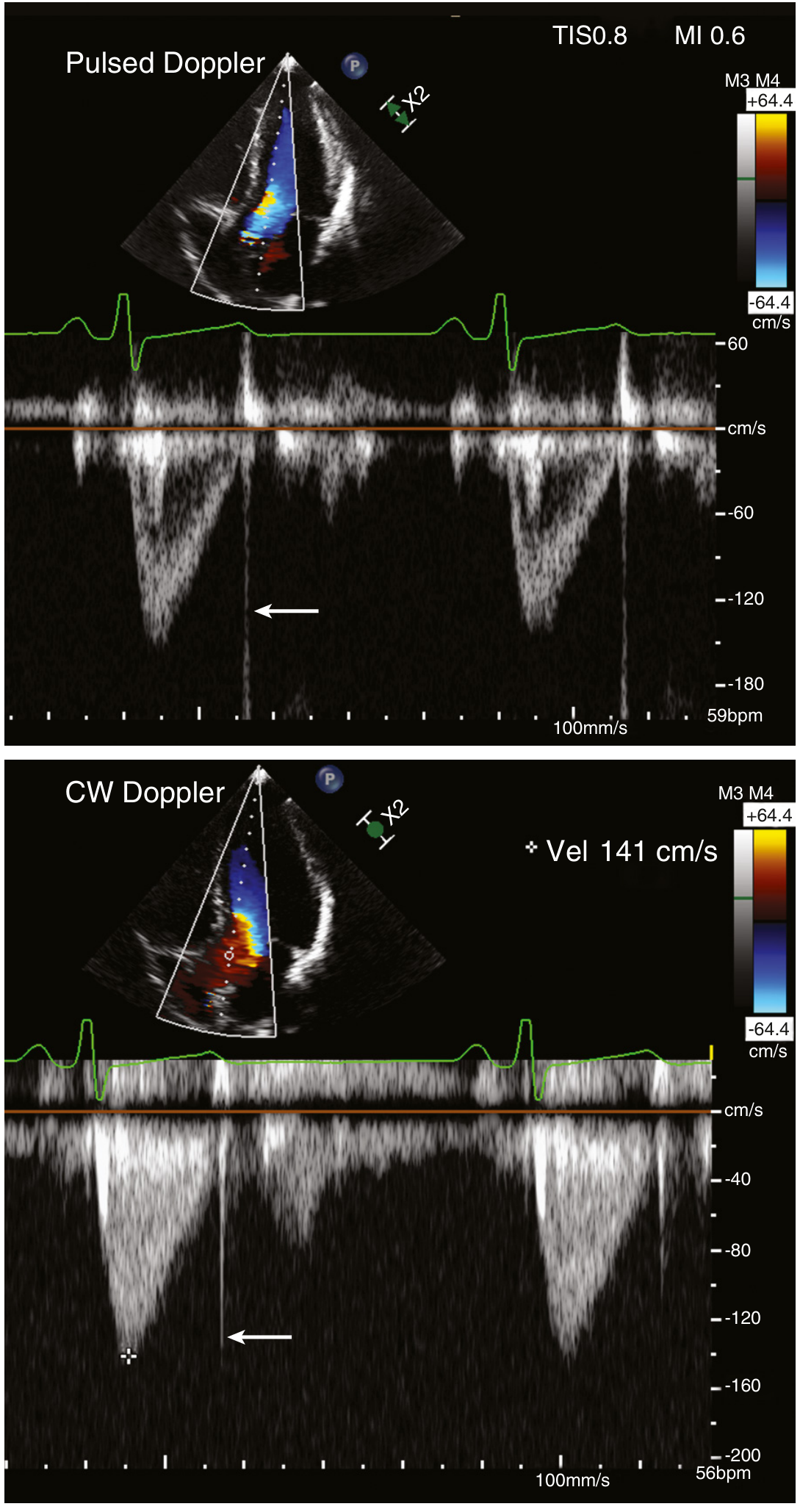
3.1 Pulsed Wave (PW) Doppler
- Depth = set by the operator (position of gate on B-mode image)
- Length = determined by the duration of the receive window (typically 3 mm; adjustable 1–10 mm)
- Width = determined by beam geometry
3.2 Continuous Wave (CW) Doppler
3.3 PW vs. CW — Head-to-Head Comparison Table
| Feature | Pulsed Wave (PW) | Continuous Wave (CW) |
|---|---|---|
| Depth selectivity | ✅ Yes — range-gated | ❌ No — entire beam |
| Maximum velocity | Limited by Nyquist | Unlimited |
| Aliasing | Yes | No |
| Spectral appearance | Hollow envelope (window) | Filled-in waveform |
| Mechanism | Pulsed transmit/receive | Continuous separate Tx/Rx crystals |
| Best use | Low-to-moderate velocities, site-specific | High-velocity jets (stenosis, regurgitation) |
| Display | Velocity at sample volume | All velocities along beam |
SECTION 4: THE NYQUIST LIMIT AND ALIASING
4.1 Nyquist Theorem Applied to PW Doppler
4.2 What Aliasing Looks Like
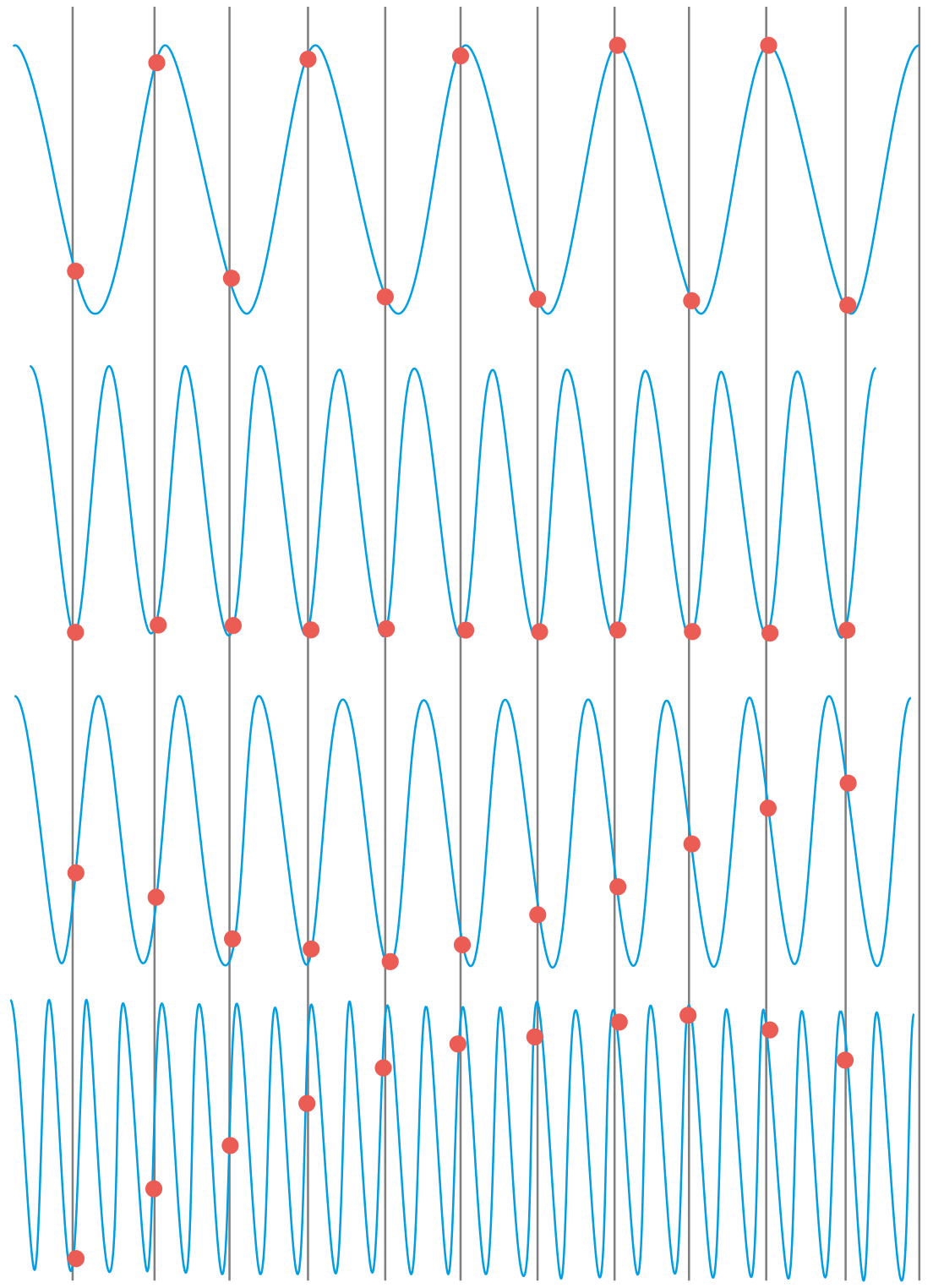
- Mild aliasing: Waveform appears "cut off" at the top, with the peak appearing in the reverse channel
- Severe aliasing: Repeated wrap-around; undifferentiated band of velocities — appears visually and aurally similar to turbulent flow
4.3 Methods to Resolve Aliasing
| Method | Mechanism | Limitation |
|---|---|---|
| Use CW Doppler | No sampling → no Nyquist limit | Loses depth information |
| Baseline shift | Electronic "cut and paste" — moves baseline to edge, extends velocity range in one direction | Only doubles usable range |
| Increase PRF (to maximum for that depth) | Higher PRF → higher Nyquist | PRF limited by depth (c/2d) |
| High-PRF mode | Multiple gates along beam at multiples of PRF | Range ambiguity (multiple sample volumes) |
| Lower transducer frequency | Lower f₀ → larger velocity for same frequency shift | Reduced image resolution |
| Reduce depth | Greater PRF allowed | May not always be possible |
| Reduce Doppler angle | Lower cos θ at 0° → signals closer to Nyquist for same true velocity | Geometry dependent |
Exam tip: CW Doppler is always the most reliable solution for aliasing when high-velocity jets must be quantified accurately.
SECTION 5: SPECTRAL BROADENING
5.1 Definition
5.2 Causes
- Turbulent flow: In turbulent flow (e.g., downstream of a stenosis), RBCs travel with chaotic, multi-directional velocities — producing a wide range of Doppler shifts simultaneously. Spectral window is filled or obliterated.
- Flow separation/recirculation: At stenotic segments, post-stenotic recirculation adds reverse-velocity components to the display.
- Beam geometry: Linear and phased array transducers use multiple elements, producing a range of insonation angles across the beam width. Different path angles → different cos θ values → range of Doppler shifts even from cells moving at the same true velocity.
- Large sample volume: A large sample gate captures RBCs with different velocities (velocity profile effect — slower near walls, faster at center in laminar flow).
- Excessive gain: Electronic noise broadens the spectrum toward the baseline.
- High transducer frequency: Larger aperture angle subtended → more angular spread → more intrinsic broadening.
- Near-field sampling: Superficial vessels experience greater intrinsic broadening due to wider angular spread of the beam.
5.3 Clinical Significance
| Spectral Feature | Interpretation |
|---|---|
| Clear spectral window | Laminar flow, normal |
| Mild broadening (near baseline) | Normal parabolic velocity profile (slower RBCs near wall) |
| Filled-in window with high velocities | Turbulent flow — stenosis, regurgitation, AVM |
| Broadening at low velocities only | Large sample volume artifact, not pathological |
SECTION 6: SPECTRAL DISPLAY SETTINGS — OPERATOR CONTROLS
6.1 Gain
- Controls amplification of the received Doppler signal
- Too high: noise fills the display, mimics spectral broadening or high velocities
- Too low: weak signal, poor waveform definition
- Optimal: Maximum signal without background noise at the margins
6.2 Scale (Velocity Range / PRF)
- Sets the Y-axis maximum velocity displayed
- Equivalent to selecting the PRF
- Too low: aliasing of normal velocities
- Too high: waveform compressed; low-velocity components not visible
- Optimal: Waveform fills ~75% of scale
6.3 Baseline Position
- Moves the zero-velocity line up or down
- Allows the operator to shift more of the display to one direction
- Used to: (1) prevent aliasing by giving the main waveform more room, (2) display forward and reverse flows asymmetrically
- Effective electronic equivalent of extending the Nyquist limit in one direction
6.4 Wall Filter (High-Pass Filter)
- Removes low-frequency, high-amplitude signals from slow-moving structures (vessel walls, valve leaflets, myocardium)
- Set too high: eliminates low-velocity diastolic flow or venous flow
- Set too low: wall-motion "thump" artifact masks near-baseline velocities
- Typical setting: 100–200 Hz for cardiac; 50–100 Hz for low-flow venous studies
6.5 Sweep Speed
- Sets the X-axis time scale (mm/s)
- Slow sweep: more cardiac cycles visible, good for rhythm
- Fast sweep: individual waveform morphology better resolved, good for measurement
6.6 Sample Volume Size (PW Only)
- Longer gate: more signal, broader spectral broadening artifact
- Shorter gate: better range resolution, less ISB, but weaker signal
- Standard: 3 mm; can reduce to 1–2 mm for precise interrogation
6.7 Insonation Angle Correction (Angle θ)
- Available on duplex vascular scanners
- Operator manually aligns cursor with vessel axis on B-mode image
- System applies cos θ correction to convert frequency shift → velocity
- Not used in cardiac Doppler (assumes beam aligned with flow)
SECTION 7: DOPPLER WAVEFORM ANALYSIS — QUALITATIVE
7.1 Normal Arterial Waveform
- Systolic peak — rapid forward flow during cardiac systole
- Early diastolic reversal — brief reverse flow as elastic recoil closes peripheral arterioles (increased peripheral resistance)
- Late diastolic forward flow — small forward component from aortic valve recoil
7.2 Abnormal Waveforms — Disease Patterns
| Finding | Pattern | Cause |
|---|---|---|
| Monophasic waveform | Single forward peak, no reversal | Proximal stenosis or occlusion reducing pulsatility; or intrinsically low-resistance bed |
| Tardus–parvus | Low-amplitude, delayed peak, rounded upstroke | Upstream high-grade stenosis — damped waveform |
| Increased diastolic flow | High diastolic-to-systolic ratio | Low-resistance distal bed (e.g., organ hyperemia, AVM) |
| Absent diastolic flow | Flow returns to baseline before systole | High peripheral resistance, critical ischemia |
| Reversed diastolic flow | Diastolic component below baseline | Severe aortic regurgitation (diastolic reversal in aorta), high peripheral resistance |
| High-velocity jet + spectral broadening | Aliased peak with filled-in window | Stenosis |
7.3 Venous Doppler
- Normal veins: phasic with respiration (flow varies with respiratory cycle)
- Loss of phasicity: suggests proximal obstruction (DVT upstream)
- Augmentation: compression of distal limb → increase in venous Doppler signal; absent augmentation = DVT between probe and compression site
SECTION 8: QUANTITATIVE SPECTRAL ANALYSIS — WAVEFORM INDICES
8.1 Peak Systolic Velocity (PSV)
8.2 End-Diastolic Velocity (EDV)
8.3 Resistive Index (RI) — Pourcelot Index
- Normal: 0.5–0.7 (organ-dependent)
- RI → 1.0: high resistance (absent or reversed diastolic flow)
- RI → 0: low resistance (very high diastolic flow)
- Angle-independent (numerator and denominator both scaled by cos θ, which cancels)
8.4 Pulsatility Index (PI) — Gosling Index
- Wider range than RI; more sensitive to upstream flow resistance changes
- Higher PI → higher pulsatility → higher resistance
- Normal carotid: PI ~1.5–1.8; Umbilical artery: PI used in obstetric assessment
8.5 Systolic/Diastolic (S/D) Ratio
8.6 Velocity-Time Integral (VTI)
8.7 Acceleration Time (AT) and Deceleration Time (DT)
- AT: Time from onset of flow to peak velocity
- DT: Time from peak velocity to return to baseline
- Shortened AT: Seen in pulmonary hypertension (RVOT AT < 100 ms)
- Prolonged DT: Seen in mitral stenosis pressure half-time (PHT) analysis
8.8 Pressure Half-Time (PHT) — Mitral Valve Area
SECTION 9: SPECTRAL DOPPLER ARTIFACTS — SYSTEMATIC CLASSIFICATION
| Artifact | Appearance | Mechanism | Clinical Implication |
|---|---|---|---|
| Aliasing | Waveform "wraps" to opposite side of baseline | Nyquist limit exceeded | Cannot measure true peak velocity — switch to CW |
| Spectral mirror image | Identical waveform above and below baseline simultaneously | Gain too high or Doppler angle ≈ 90° causing ISB to produce signals in both channels | Reduce gain; adjust angle |
| Range ambiguity | Signals from more than one depth recorded simultaneously | High-PRF mode or very high PRF — pulse repeats before previous echo returns | Occurs with high-PRF; know which sample volume is active |
| Beam width artifact | Superimposed signals from different flows | Beam wide enough to encompass adjacent vessels or valves | CW especially prone; use PW to isolate depth |
| Electronic interference | Horizontal bands or noise across display | Electrical interference from adjacent equipment | Shielding; common in ICU/OR |
| Transit-time effect | Slight velocity overestimation | Change in ultrasound propagation speed through moving medium | Minor effect; "blurring" on velocity axis |
| Wall thump | Low-frequency, high-amplitude artifact near baseline | Valve/wall motion detected | Increase wall filter |
| Intrinsic spectral broadening (ISB) | Artificially widened spectrum | Multiple beam angles across aperture produce range of cos θ | Reduces spectral window; can mimic turbulence |
SECTION 10: COLOR FLOW DOPPLER — RELATIONSHIP TO SPECTRAL DOPPLER
- For each scan line: 8 pulses (burst length) are transmitted and the received signals autocorrelated
- Autocorrelation (not FFT): calculates mean velocity at each depth along each scan line — much faster than FFT, enabling real-time 2D display
- Trade-off: Color Doppler measures mean velocity only, not the full spectral distribution — this is why spectral (PW/CW) Doppler is needed for quantitative velocity measurements
- Color encoding: Flow toward transducer = red; away = blue; turbulence/aliasing = mosaic of green/yellow
| Mode | Analysis Method | Output | Velocity info |
|---|---|---|---|
| Spectral PW/CW | FFT | Spectrogram (velocity vs. time) | Full velocity spectrum |
| Color Doppler | Autocorrelation | 2D color map | Mean velocity only |
| Power Doppler | Amplitude-based | 2D map of signal strength | Direction only; no velocity |
SECTION 11: CLINICAL APPLICATIONS BY SYSTEM
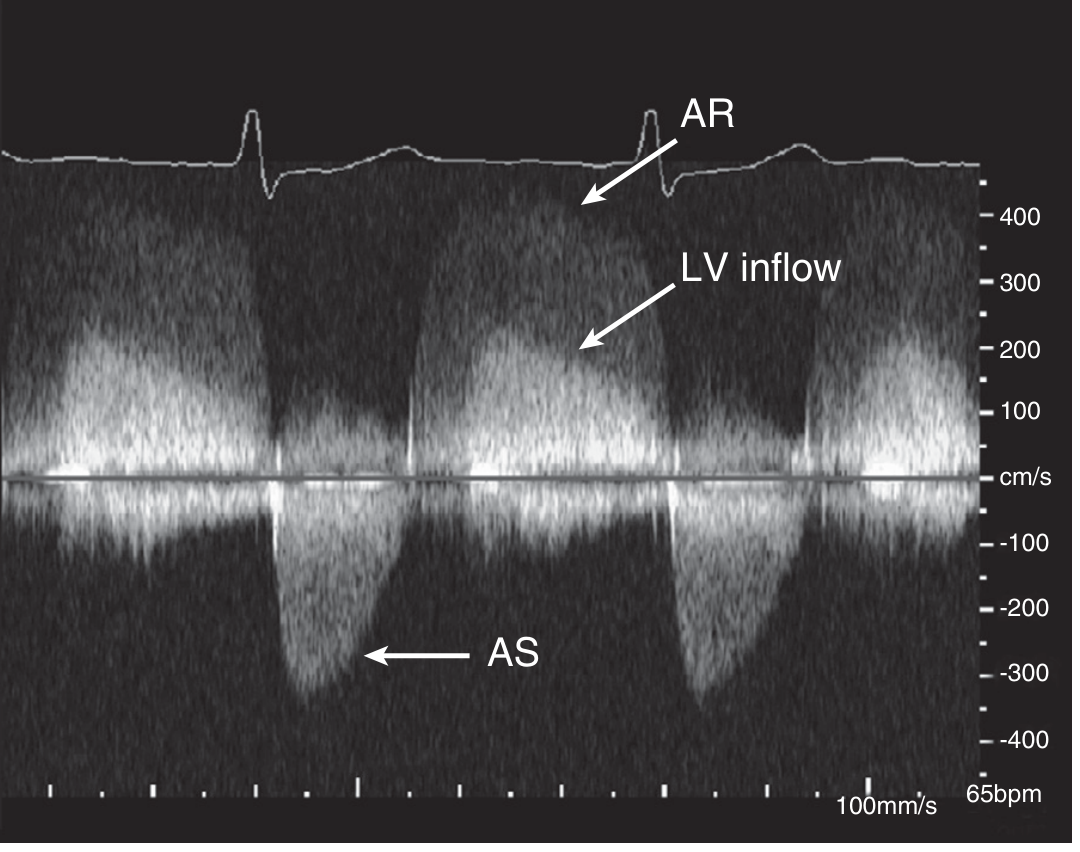
Cardiac (Echocardiography)
- Aortic stenosis: CW Doppler across valve → peak velocity → modified Bernoulli: ΔP = 4v²
- Mitral inflow: PW at mitral leaflet tips → E wave (early filling), A wave (atrial contraction), E/A ratio for diastolic function
- LVOT VTI: PW in LVOT → VTI × CSA = stroke volume; track changes in cardiac output
- Pulmonary hypertension: TR jet velocity by CW → RVSP = 4v² + RAP; RVOT AT by PW
Vascular (Peripheral)
- Carotid stenosis: PSV >125 cm/s = ≥50% stenosis; PSV >230 cm/s + ICA/CCA ratio >4 = ≥70% stenosis
- Renal artery stenosis: PSV >180–200 cm/s; RI >0.70 in intrarenal arteries suggests distal disease
- Ankle-Brachial Index (ABI): CW hand-held Doppler + sphygmomanometer; normal 0.9–1.4; <0.9 = significant arterial disease; <0.4 = critical limb-threatening ischemia — Bailey & Love's Surgery 28e
Obstetric
- Umbilical artery: S/D ratio; absent or reversed end-diastolic flow = severe fetal compromise
- Middle cerebral artery (MCA): Peak PSV > 1.5 MoM for gestational age indicates fetal anemia (brain-sparing)
- Uterine artery: RI, PI; early diastolic notch = abnormal placentation
SECTION 12: HIGH-YIELD EXAM SUMMARY TABLE
| Topic | Key Fact |
|---|---|
| Doppler equation | $f_d = 2f_0 v \cos\theta / c$ |
| Maximum angle | 60° (cos 60° = 0.5; 50% underestimation) |
| At 90° | cos 90° = 0; no Doppler shift measured |
| Nyquist limit | PRF/2 |
| Aliasing appearance | Waveform wraps to opposite side of baseline |
| CW advantage | No aliasing; unlimited velocity range |
| CW disadvantage | No depth selectivity (entire beam recorded) |
| PW advantage | Depth-selective (range-gated) |
| PW disadvantage | Aliasing at high velocities |
| Spectral window | Clear area under peak = laminar flow |
| Spectral broadening causes | Turbulence, large sample volume, ISB, gain artifact |
| FFT role | Decomposes received signal into component frequencies for each time window |
| Color Doppler analysis | Autocorrelation (not FFT); gives mean velocity only |
| RI formula | (PSV − EDV) / PSV |
| PI formula | (PSV − EDV) / TAMV |
| VTI clinical use | × CSA = stroke volume |
| Bernoulli equation | ΔP = 4v² (simplified; v in m/s, ΔP in mmHg) |
| PHT formula for MVA | MVA = 220 / PHT |
| ABI normal range | 0.9–1.4 |
| ISB — what is it | Artificial spectral broadening from beam geometry (range of angles) |
| Wall filter purpose | Remove low-frequency wall-motion signals |
SECTION 13: WORKED EXAMPLE — COMPLETE DOPPLER CALCULATION
References
- Textbook of Clinical Echocardiography — CW Doppler, PW Doppler, Aliasing, Spectral Analysis, Color Flow, Artifacts
- Miller's Anesthesia 10e — Harmonic Imaging, 3D Imaging, Perioperative Echo
- Fuster & Hurst's The Heart 15e — Doppler Ultrasound, Carotid DUS
- Bailey & Love's Short Practice of Surgery 28e — Doppler Blood Flow Detection, ABI
- Principles of Doppler ultrasound and emerging blood flow imaging — PMC 2025 Review
- Brett Gerrard — Doppler Ultrasound Physics (spectral broadening, ISB)
3d ultrasound imaging , acquisition, visualisation, display methods in detail and instrumentation
3D ultrasound imaging acquisition methods visualization display voxel volume rendering instrumentation
3D ultrasound acquisition freehand mechanical matrix array reconstruction voxel interpolation volume rendering surface rendering
3D ultrasound volume rendering surface rendering multiplanar reconstruction
3D Ultrasound Imaging: Acquisition, Reconstruction, Visualisation, Display Methods, and Instrumentation
SECTION 1: CONCEPTUAL OVERVIEW — FROM 2D TO 3D
1. ACQUISITION → 2. RECONSTRUCTION → 3. VISUALISATION/DISPLAY
SECTION 2: INSTRUMENTATION — THE 3D TRANSDUCER
2.1 Matrix Array Transducer — The Key Hardware
- Element count: 2,500–9,000+ elements (e.g., 50×50, 60×60, or 72×72 grids)
- Transmit elements: may be a subset; receive elements: fully sampled
- Aperture: typically 25–30 mm × 25–30 mm
- Frequency: 2–7 MHz (cardiac TTE/TEE)
- Element pitch: ~0.2–0.3 mm (approximately λ/2 at operating frequency)
2.2 ASIC Integration in 3D Probes
- Micro-beamforming: The ASIC groups elements into sub-apertures (patches of ~16 elements) and performs partial beamforming within each patch, reducing the cable count from thousands to ~128–256 signal channels transmitted to the system
- Time-delay control: Precise sub-nanosecond delay chips in the ASIC for each element
- Transmit/receive switching: High-voltage transmit multiplexers and low-noise receive amplifiers on chip
- Power management: On-chip bias and power-supply regulation within the probe handle
2.3 Probe Variants
| Probe Type | Design | Application |
|---|---|---|
| Transthoracic 3D (xMATRIX) | Large matrix array, handheld | Cardiac TTE, 3D echo |
| 3D TEE (miniaturized matrix) | Miniaturized matrix in TEE endoscope tip | Intraoperative, valve assessment |
| 3D Intracardiac Echo (ICE) | Matrix array on catheter | Structural heart interventions |
| 3D Abdominal/OB probe | Mechanical or electronic matrix | Fetal, gynecology, abdominal |
| Mechanical 3D probe | Motor-driven 1D array | Abdominal, musculoskeletal |
| Freehand 3D system | Conventional 2D probe + position sensor | Research, vascular |
SECTION 3: DATA ACQUISITION METHODS
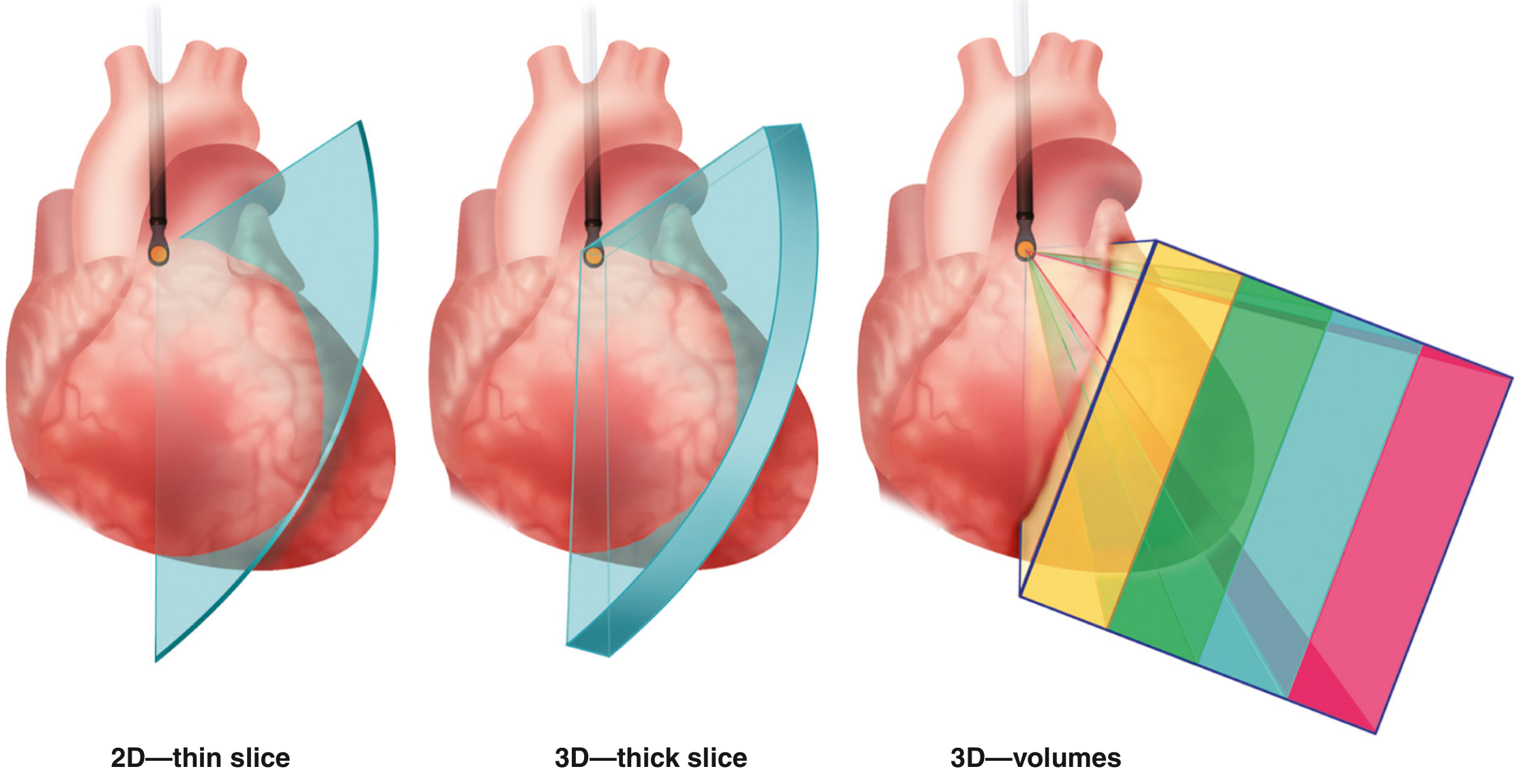
3.1 Method 1: Real-Time Matrix Array (Electronic Steering) — Gold Standard
- The matrix array transmits a diverging wavefront (or series of focused beams) covering the full pyramidal sector in both lateral dimensions
- Line-by-line (or plane-by-plane) data is collected by sequential beam-steering
- A complete volumetric dataset is assembled within a single or few cardiac cycles
- Volume rate (temporal resolution)
- Pyramid size (field of view)
- Spatial resolution (number of scan lines per volume)
3.2 Method 2: Mechanical 3D Scanning
- Linear sweep: Array translates along the elevation axis in fixed step increments → parallel 2D slices stacked to form a rectangular volume (used in fetal/abdominal 3D)
- Tilt/fan sweep: Array pivots about a central axis → radially arranged 2D slices forming a fan-shaped volume (used in transvaginal 3D, small-parts)
- Rotational sweep: Array rotates about the beam axis → cone-shaped volume (used in transvaginal 3D; basis of STIC acquisition)
3.3 Method 3: Freehand 3D Scanning
- Electromagnetic tracking (most common): small coils on the probe measure position and orientation within an external magnetic field (6 degrees of freedom — 3 translational + 3 rotational)
- Optical (infrared) tracking: retroreflective markers on probe tracked by overhead camera
- Acoustic arm: rigid mechanical arm with joint encoders (3 DOF) — accurate but restricts probe movement
- Sensorless (speckle tracking): decorrelation of RF speckle patterns between frames used to estimate relative probe displacement — no external hardware needed but less accurate
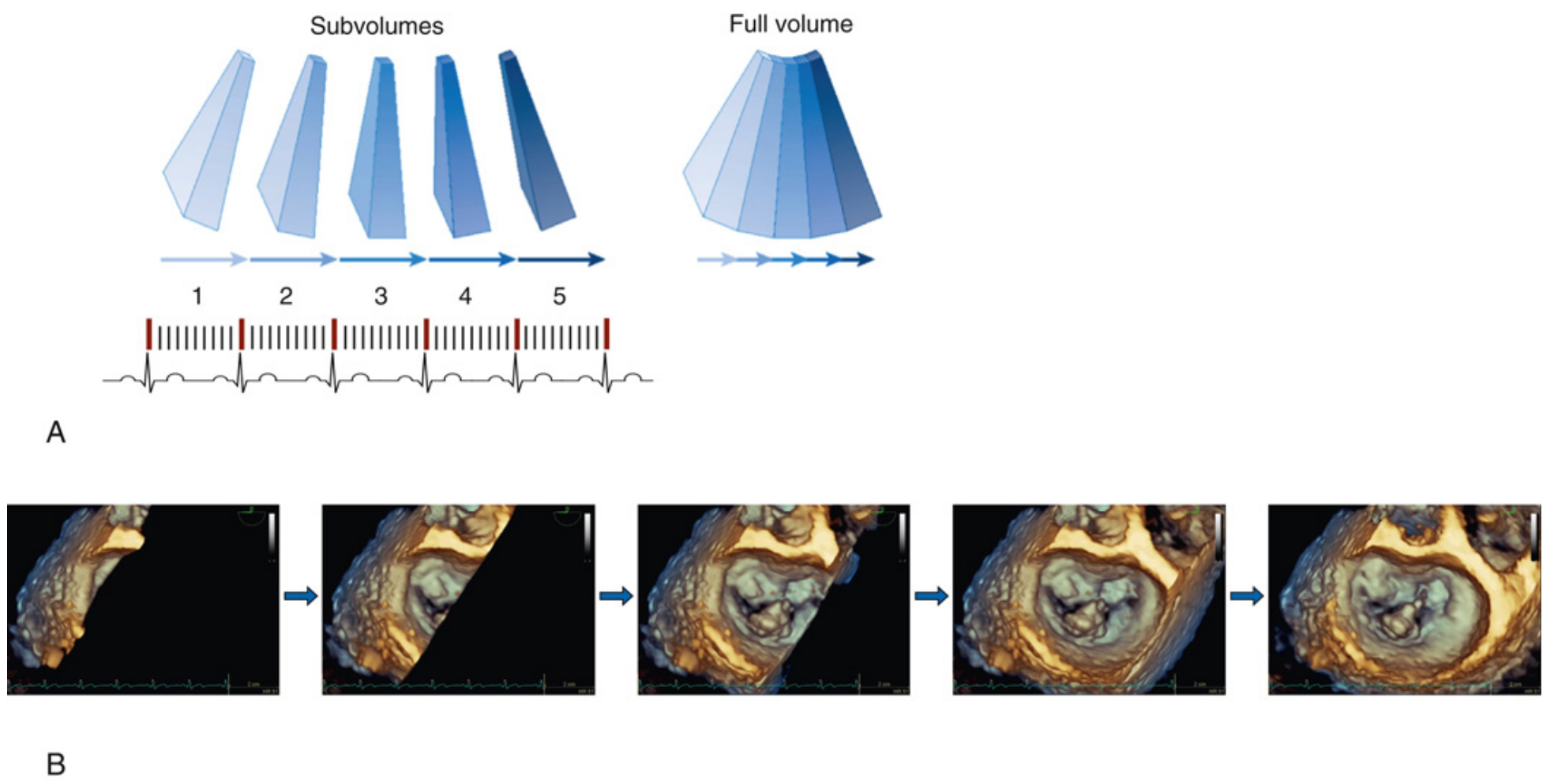
3.4 Method 4: ECG-Gated Multi-Beat Acquisition (Cardiac — Most Important Clinically)
Beat 1: Subvolume 1 (left wedge of pyramid)
Beat 2: Subvolume 2 (adjacent wedge)
Beat 3: Subvolume 3
Beat 4: Subvolume 4
↓
Offline stitching → Full pyramidal volume
- Irregular heart rhythm (atrial fibrillation)
- Respiratory motion
- Patient body movement
- Significant beat-to-beat variation in stroke volume
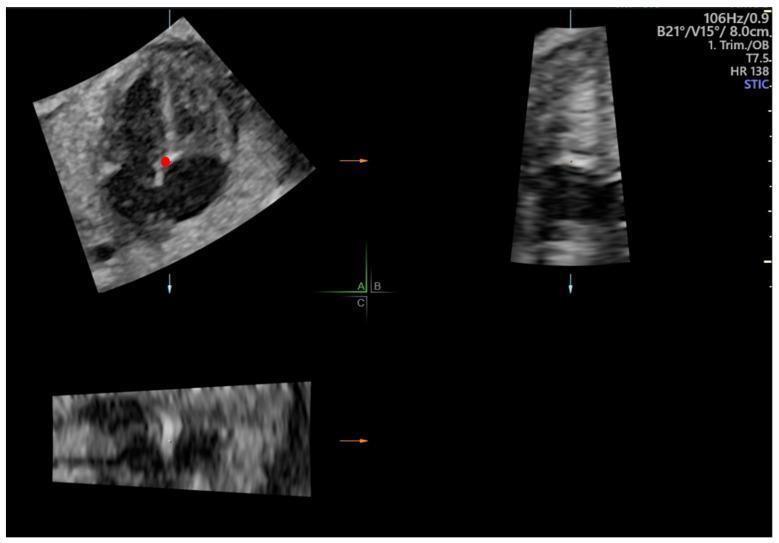
3.5 Spatiotemporal Image Correlation (STIC) — Fetal Cardiac Imaging
- A slow linear or rotational sweep acquires ~150–400 2D frames over ~7.5–15 seconds
- The system automatically detects the fetal heart rate from the temporal periodicity in the acquired frames (by detecting pulsations) — no ECG leads required
- Frames are retrospectively sorted by their phase within the cardiac cycle
- Results in a 4D cine loop of the fetal heart — a complete volumetric cardiac dataset cycling through systole and diastole
- Can be combined with B-mode, colour Doppler, power Doppler, or HD-Flow for vascular mapping
SECTION 4: VOLUME RECONSTRUCTION (2D → 3D Dataset)
4.1 Voxel-Based Methods (VBMs) — Most Common
4.2 Pixel-Based Methods (PBMs) — Forward Projection
4.3 Function-Based Methods (FBMs) — Interpolating Functions
SECTION 5: COORDINATE SYSTEMS AND IMAGE PLANES
↑ AXIAL (depth axis, A-plane)
|
|
+———→ LATERAL (azimuthal, left-right)
/
/
ELEVATIONAL (sagittal-equivalent, front-back = C-plane)
| Plane | Definition | Equivalent |
|---|---|---|
| A-plane | Standard 2D B-mode sweep plane | Long-axis equivalent |
| B-plane | Elevation cross-sections perpendicular to A-plane | Short-axis equivalent |
| C-plane (en face) | Parallel to probe face at a given depth | "Bull's eye" or en-face view |
SECTION 6: VISUALISATION MODES — DISPLAY METHODS
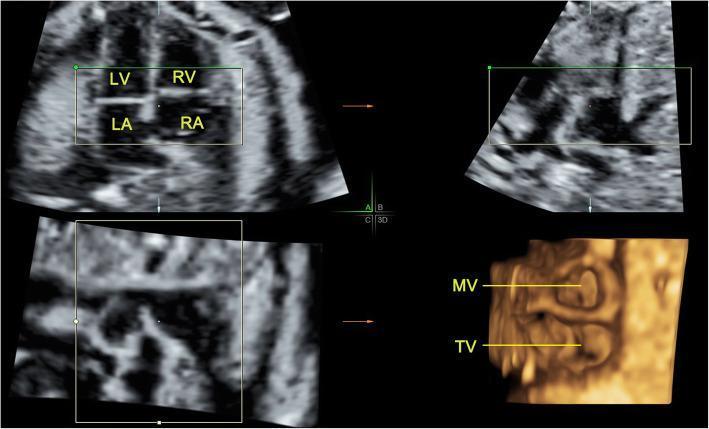
6.1 Multiplanar Reconstruction / Reformatting (MPR)
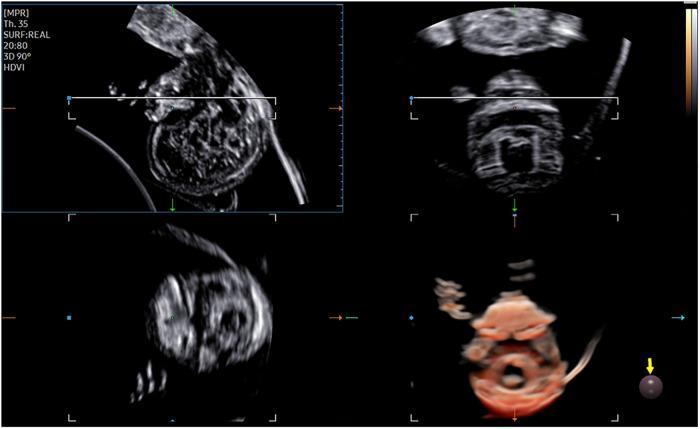
- Top-left: Primary reference plane (e.g., sagittal / long-axis)
- Top-right: Second orthogonal plane (e.g., transverse / short-axis)
- Bottom-left: Third orthogonal plane (e.g., coronal / elevation)
- Bottom-right: 3D rendered or reference volume with colour-coded intersection lines
- Acquire the volumetric dataset
- Select the desired anatomical reference point — the system displays all three orthogonal planes through that point simultaneously
- Rotate or tilt any plane independently — the others update in real time
- Use for planimetry (area measurement), annulus sizing, lesion localization
6.2 Slice Projection (Thick-Slab MIP/MinIP)
- Maximum Intensity Projection (MIP): Each projected pixel = maximum brightness voxel along the ray through the slab. Best for hyperechoic structures (calcified valves, calculi, bony landmarks)
- Minimum Intensity Projection (MinIP): Each pixel = minimum voxel. Best for anechoic fluid-filled structures (cysts, cardiac chambers, vessels)
- Average Projection: Blends all voxels — improves SNR but reduces contrast
6.3 Surface Rendering
- Segmentation: Define the interface between two tissue types (e.g., blood–endocardium, fluid–fetal skin). May be manual (operator traces boundary on multiple 2D planes), semi-automated (active contour/snakes algorithm), or automated (tissue-type classification)
- Mesh generation: The boundary points are connected into a polygonal mesh (triangles), forming a 3D surface
- Shading and rendering: A virtual light source illuminates the surface — near structures appear bright, far structures shadowed — creating depth perception
- Display: The rendered surface is projected onto the 2D monitor as a photorealistic-looking structure
- Fetal face: Photorealistic surface of fetal skin — used in obstetric 3D ultrasound
- LV endocardial surface: The LV inner wall traced over the cardiac cycle → beating 3D model for volume quantification (LV EF without geometric assumptions)
- Mitral valve: 3D leaflet surface shows prolapse segments, flail, restricted motion from LA or LV perspective
- Aortic valve: En-face view from aorta shows cusp number, calcification, orifice area
6.4 Volume Rendering — The Most Clinically Used Method
Voxel Data
↓
Transfer Function (maps grey-value → colour + opacity)
↓
Compositing (integrate along each ray through volume)
↓
Projected 2D Image on Screen
- Low grey values (anechoic blood/fluid) → fully transparent (rendered invisible)
- Mid grey values (myocardium, soft tissue) → semi-transparent, coloured orange/gold
- High grey values (calcium, valve leaflets) → opaque, bright white/yellow
6.5 Wireframe Display
- 3D LV models showing endocardial wireframe contracting over time
- Mitral valve annulus: 3D saddle-shaped annulus outline
- Research quantification where the boundary coordinates are extracted for numerical analysis
6.6 Parametric Colour Maps (Bull's-Eye Plots)
- Displayed on a flat "bull's-eye" map (apical view looking from apex)
- Provides a comprehensive at-a-glance overview of regional LV function
- Ischaemic territories show synchrony defects as colour differences
- Used for dyssynchrony assessment and regional wall-motion analysis
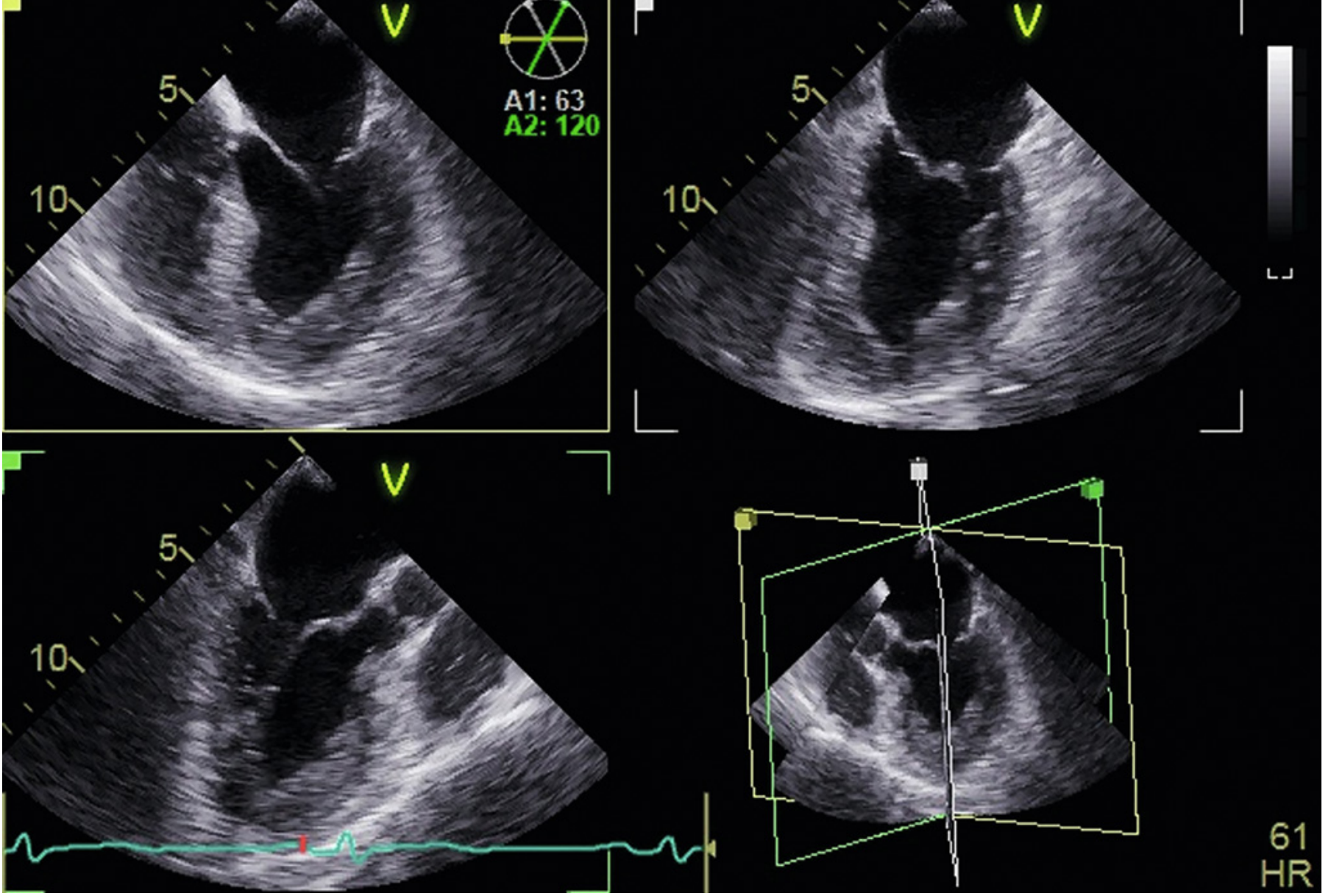
6.7 Simultaneous Multiplane (Biplane / Triplane) Display
- Primary reference plane + one or two secondary planes at adjustable angles
- Each plane is independently rotatable in real time
- The 3D orientation of all planes shown in a fourth "locator" panel
- Advantage: Highest temporal and spatial resolution of all 3D modes (because each plane still uses full array aperture) — Miller's Anesthesia 10e
6.8 4D Ultrasound (Real-Time 3D Cine)
- Single-beat 4D: volume rate ~5–15 volumes/second (limited by pyramid size and depth)
- Multi-beat 4D (gated): retrospective reconstruction → higher effective temporal resolution but requires stable rhythm
SECTION 7: ACQUISITION MODES — CLINICAL 3D IMAGING MODES IN DETAIL
7.1 Real-Time Narrow Sector (3D Live / Narrow Volume)
| Feature | Value |
|---|---|
| Pyramid size | ~30° × 60° |
| Volume rate | ~20–30 Hz |
| Spatial resolution | Highest of live modes |
| Data source | Single beat, real-time |
| Best for | Quick orientation, guiding catheter/needle, complex anatomy assessment |
| Limitation | Narrow FOV — entire structure often excluded |
7.2 Real-Time Zoom / Wide Sector Mode
| Feature | Value |
|---|---|
| Pyramid size | User-selected enlarged ROI |
| Volume rate | ~10–20 Hz |
| Spatial resolution | Reduced (wider pyramid = fewer scan lines per area) |
| Data source | Single beat |
| Best for | Real-time manipulation, valve visualization, procedure guidance |
| Limitation | Lower spatial and temporal resolution; cannot save/reanalyse post-hoc |
7.3 Full-Volume Gated (Multi-Beat) Mode — Highest Quality
| Feature | Value |
|---|---|
| Pyramid size | Full cardiac pyramid (~90° × 90°) |
| Number of subvolumes | Typically 4–6 heartbeats |
| Volume rate | High (4-beat = ~4× improvement over single-beat) |
| Data source | Multi-beat ECG-gated stitching |
| Best for | LV volume/EF quantification; post-hoc analysis; valve assessment |
| Limitation | Requires regular rhythm; stitch artifact with arrhythmia/movement |
| Post-processing | Full data set saved → can re-crop, re-render, quantify offline |
7.4 Single-Beat Full Volume (Live Full-Volume)
- Same pyramidal coverage as multi-beat but acquired from a single heartbeat
- Eliminates stitch artifact (suitable for AF, arrythmia, non-compliant patients)
- Lower spatial and temporal resolution than gated acquisition
- Frame rate: ~3–8 Hz — adequate for general assessment but not precise quantification
7.5 3D Colour Flow Doppler
- Volume-rendered pyramidal dataset with colour Doppler overlaid on grey-scale
- Acquired in real-time (single beat) or multi-beat gated mode
- Very low volume rate (colour acquisition requires multiple pulses per line → fewer volumes/second)
- Optimised using R-wave gated multi-beat acquisition
- Clinically used to visualize 3D distribution of paravalvular leaks, intracardiac shunts, mitral regurgitation jets — Textbook of Clinical Echocardiography; Miller's Anesthesia 10e
SECTION 8: THE FUNDAMENTAL TRIAD TRADEOFF
TEMPORAL RESOLUTION
(Volume rate, Hz)
/\
/ \
/ \
/______\
SPATIAL FIELD OF VIEW
RESOLUTION (Pyramid size)
- Smaller pyramid → higher volume rate (better temporal resolution) OR more scan lines (better spatial resolution)
- Greater depth → lower PRF per line → lower volume rate
- More scan lines → better lateral resolution → lower volume rate
- Multi-beat gating → overcomes the tradeoff by spreading the scan line load across multiple beats
- Narrow sector: best temporal + spatial resolution, small FOV
- Zoom: larger FOV, worse both
- Full-volume single beat: largest FOV, worst both
- Full-volume multi-beat gated: largest FOV, best of all — at the cost of stitching requirements
SECTION 9: IMAGE OPTIMISATION FOR 3D ACQUISITION
Gain and Compression
- Start with slight over-gain (~50 units) to avoid echo dropout appearing as holes in structures
- Excess gain → obscures fine detail (e.g., aortic valve cusp edges appear fused)
- 3D images are more sensitive to gain than 2D because dropout is amplified in volume rendering
- Effect: Low gain → dropout (holes); optimal → clean anatomy; high gain → obscured detail — Textbook of Clinical Echocardiography, Fig. 4.4
Time-Gain Compensation (TGC)
- Adjust so that the near field and far field are equally bright before acquiring 3D
- Uneven TGC is magnified in volume-rendered images
Focus Depth
- Set the focal zone at the centre of the structure of interest
- Single focal zone recommended to maximise frame rate
Sector Size and Depth
- Reduce depth to minimum that still includes the entire structure → increases PRF → increases volume rate
- Reduce pyramid width to minimum necessary → same effect
Post-Processing
- Threshold: Adjusts opacity mapping — varies which grey values become transparent. Critical for separating blood pool from myocardium
- Depth: Adjusts virtual illumination angle
- Rotation/Cropping: After full-volume acquisition, crop interactively to reveal internal anatomy from any perspective
SECTION 10: ARTEFACTS SPECIFIC TO 3D ULTRASOUND
| Artifact | Appearance | Mechanism | Solution |
|---|---|---|---|
| Stitch artifact | Vertical bright/dark line across volume | Misregistration of subvolumes due to irregular rhythm/motion | Ensure regular rhythm + breath-hold; use single-beat mode |
| Echo dropout | Holes in solid-appearing structures | Insufficient gain; structure parallel to beam | Increase gain; optimise transducer angle |
| Stitching ghosting | Double or ghost image of moving structures | Beat-to-beat variation in cardiac position | Use single-beat acquisition in arrhythmia |
| Foreshortening | Underestimation of LV length | Beam not parallel to LV long axis | Optimise transducer position |
| Resolution anisotropy | Axial resolution >> lateral resolution in elevation | Beam wider in elevation than lateral | Accept as inherent limitation; optimise focus |
| Reduced frame rate | Blurry or jerky 3D motion | Pyramid too large / excessive depth | Reduce depth, reduce sector angle, use multi-beat |
| Range ambiguity | Signal from outside stated pyramid | High-PRF equivalent in 3D mode | Limit pyramid depth |
SECTION 11: QUANTITATIVE ANALYSIS FROM 3D DATA
11.1 LV Volume and Ejection Fraction
- 3D LV EF is the most accurate non-invasive method — no geometric assumptions (unlike Simpson's biplane which assumes an ellipsoid)
- Method: Semi-automated endocardial border tracing in MPR, then software calculates enclosed volume at each time point
- LV EF = (EDV − ESV) / EDV × 100%
- Reference standard comparison: excellent correlation with cardiac MRI — Fuster & Hurst's The Heart 15e
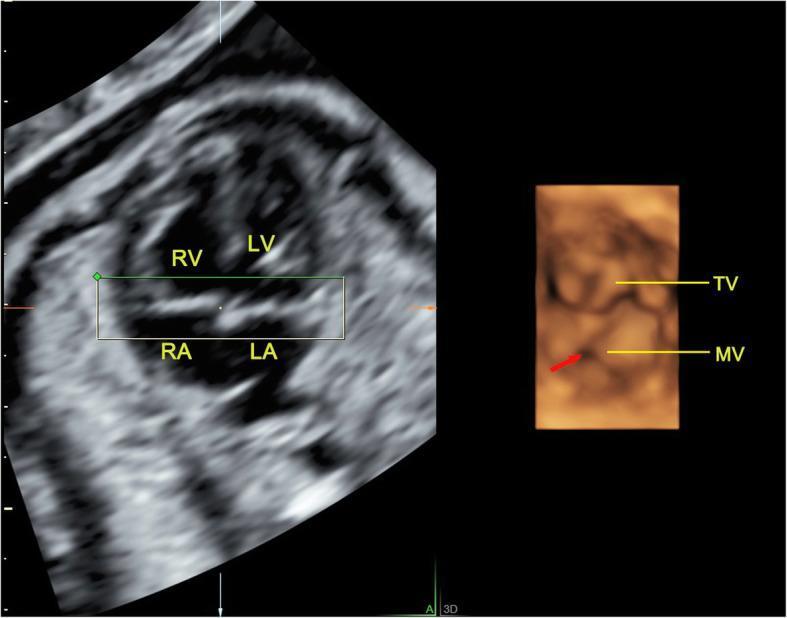
11.2 Mitral Valve Analysis
- 3D TEE allows en-face "surgeon's view" of the mitral valve from LA perspective
- MPR determines precise annulus dimensions: major/minor axis, 3D annular area, annular perimeter — used for MitraClip sizing, surgical ring sizing
- Dynamic annular tracking over cardiac cycle reveals saddle-shape deformation
11.3 Multiplanar Reformatting (MPR) for Measurements
- Linear dimensions and areas (e.g., aortic annulus for TAVI)
- Planimetry of stenotic orifices (precise short-axis cross-section through stenotic jet)
- Left atrial appendage dimensions for occlusion device sizing
- The simultaneous multi-axis visualization guides transcatheter procedures — Miller's Anesthesia 10e
SECTION 12: CLINICAL APPLICATIONS BY SPECIALTY
| Specialty | Application |
|---|---|
| Cardiac — Structural | LV EF; RV volume; CHD anatomy; TAVI planning; mitral valve prolapse mapping; aortic valve en-face |
| Cardiac — Interventional | Real-time 3D TEE guidance of TAVI, MitraClip, WATCHMAN LAA closure, ASD/VSD closure, transseptal puncture |
| Cardiac — Electrophysiology | Pulmonary vein 3D anatomy; LAA morphology assessment |
| Obstetrics | Fetal face (cleft lip/palate); fetal cardiac STIC; placenta volume; fetal biometry |
| Gynecology | Uterine anomalies (arcuate, bicornuate, septate); IUD position; ovarian follicle counting |
| Vascular | 3D CEUS endoleak detection; carotid plaque volume; 3D vascular mapping |
| Urology | Prostate volume; renal mass characterization |
| Musculoskeletal | Volumetric joint imaging; neonatal hip dysplasia |
SECTION 13: SUMMARY COMPARISON TABLE
| Feature | 2D Ultrasound | 3D Single-Beat | 3D Multi-Beat Gated | 4D / RT-3D |
|---|---|---|---|---|
| Frame rate | 50–100 Hz | 3–15 Hz | High (beat number dependent) | 5–20 Hz |
| FOV | One plane | Narrow pyramid | Full pyramid | Adjustable pyramid |
| Spatial resolution | High (one plane) | Reduced | Highest | Variable |
| Requires ECG gating | No | No | Yes | No |
| Affected by arrhythmia | No | No | Yes (stitch artifact) | No |
| Post-hoc rotation | No | Limited | Full | Limited |
| Quantification (LV EF) | Geometric assumptions | Moderate | Best (no geometric assumptions) | Moderate |
| Real-time procedural guidance | Yes | Yes | No (offline stitching) | Yes |
SECTION 14: HIGH-YIELD EXAM SUMMARY POINTS
- 3D ultrasound stages: Acquisition → Reconstruction → Visualisation
- Matrix array key feature: Thousands of elements in 2D rectangular grid; electronic steering in both lateral and elevation planes; ASIC micro-beamforming reduces cable count
- Pyramidal output: All 3D cardiac datasets are pyramid-shaped with apex at transducer face
- Tradeoff triad: Volume rate ↔ Spatial resolution ↔ Field of view — cannot optimise all three simultaneously
- Multi-beat gating: Overcomes the tradeoff by spreading scan lines over N beats; requires regular rhythm + breath-hold; produces stitch artifact if either fails
- Volume reconstruction algorithms: VBM (nearest-neighbour, distance-weighted), PBM (forward projection), FBM (function-based/spline) — VBM NN is fastest; FBM most accurate
- Three visualisation planes: A-plane (standard B-mode), B-plane (elevation cross-section), C-plane (en-face/depth)
- MPR: Any arbitrary 2D plane extracted from 3D dataset; 4-quadrant display; angle-independent measurement
- Volume rendering: Opacity + colour transfer function applied to raw voxel data; no segmentation required; most clinically used 3D display
- Surface rendering: Requires boundary segmentation first; photorealistic; used for fetal face, LV EF model
- Gain critical: Over-gain → obscures detail; under-gain → dropout holes in solid structures
- 3D EF: Most accurate; no geometric assumption; correlates with MRI; method of choice for LV volume quantification
- STIC: Fetal cardiac 4D — retrospective gating using intrinsic cardiac pulsation; no ECG needed
- Stitch artifact: Vertical line; cause = irregular rhythm/movement during multi-beat acquisition; solution = single-beat mode or ensure regular rhythm
References
- Textbook of Clinical Echocardiography — Three-Dimensional Echocardiography (Ch. 4): acquisition modes, image display, gain optimisation, stitch artifact
- Miller's Anesthesia 10e — 3D Image Acquisition, Multiplane Imaging, Gated Acquisition, MPR, Quantitative Analysis
- Fuster & Hurst's The Heart 15e — 3D Echocardiography: matrix array, surface rendering, LV/RV volumes, MRI correlation
- Barash's Clinical Anesthesia 9e — 3D TEE: pyramidal dataset, volume rendering, procedural guidance
- PALNI Ultrasound Physics — Equipment design, STIC, 4D display, rendering methods
- Steen E, Olstad B. Volume rendering of 3D medical ultrasound data using direct feature mapping. IEEE Trans Med Imaging 1994 [PMID: 18218527]
3d ultrasound imaging , acquisition, visualisation, display methods in detail and instrumentation
- Conceptual overview (2D → 3D transition)
- Instrumentation — Matrix array transducer design, element count, ASIC micro-beamforming, probe variants
- Acquisition methods — Electronic matrix steering, mechanical scanning (linear/tilt/rotational), freehand with position tracking (EM/optical/acoustic arm/sensorless), ECG-gated multi-beat stitching, STIC (fetal)
- Volume reconstruction — VBM (nearest-neighbour, distance-weighted, Gaussian), PBM (pixel-based), FBM (function-based/spline)
- Visualisation & Display methods — MPR/multiplanar reformatting, slice projection (MIP/MinIP), surface rendering, volume rendering (with transfer function pipeline), wireframe, parametric bull's-eye maps, simultaneous multiplane, 4D real-time
- Acquisition modes — Narrow sector, zoom/wide sector, full-volume single-beat, full-volume multi-beat gated, 3D colour Doppler
- The fundamental triad tradeoff — Volume rate ↔ Spatial resolution ↔ Field of view (with equation)
- Image optimisation — Gain, TGC, focus, sector size
- 3D-specific artifacts — Stitch, dropout, ghosting, resolution anisotropy
- Quantitative analysis — LV EF, MVA, MPR-guided measurements
- Clinical applications by specialty
- High-yield exam summary (14 key points)
4D ultrasound imaging , acquisition, visualisation, display methods in detail and instrumentation
4D ultrasound imaging acquisition visualization display instrumentation real-time volume rate
4D ultrasound instrumentation acquisition volume rate display modes real-time STIC fetal cardiac
4D ultrasound cardiac STIC fetal acquisition volume rate GPU rendering instrumentation 2024
4D ultrasound acquisition modes volume rate GPU rendering STIC fetal cardiac instrumentation display
4D ultrasound real-time fetal cardiac STIC volume rendering display
4D Ultrasound Imaging — Acquisition, Visualisation, Display Methods, and Instrumentation
SECTION 1: DEFINITION AND CONCEPTUAL BASIS
1.1 What is 4D Ultrasound?
- 3D ultrasound: Acquires a single static volumetric dataset (x, y, z spatial dimensions)
- 4D ultrasound: Acquires a continuous, rapidly updating sequence of 3D volumes displayed in real time, so the anatomy is seen moving within the 3D volume
"Four-dimensional ultrasonography: an imaging method that adds the dimension of time via the fast and continuous acquisition and display of 3D volumes, especially useful for imaging moving targets (fetal heart, moving limbs)." — Volume Sonography Core Concepts
1.2 Terminology Clarification
| Term | Meaning | Context |
|---|---|---|
| RT-3D (Real-Time 3D) | Live 3D volumes displayed continuously | Cardiac echo (some authors call this 4D) |
| 4D ultrasound | Live 3D cine loop, typically at lower volume rates | Obstetric (fetal face, body movements) |
| 4D-STIC | Retrospectively gated 4D cine of fetal heart | Fetal echocardiography |
| Live 3D | Single-beat real-time 3D | Cardiac (e.g., Philips, GE nomenclature) |
| 4D echo | Real-time 3D cardiac with colour Doppler | Cardiology |
"RT-3D imaging acquires data over a single heartbeat; some authors and vendors refer to this as 4D imaging." — Miller's Anesthesia 10e
SECTION 2: INSTRUMENTATION FOR 4D IMAGING
2.1 The Matrix Array Transducer — Core Instrument
| Parameter | Value |
|---|---|
| Element count | 2,500–9,000+ elements |
| Grid configuration | Square: e.g., 50×50, 60×60, 72×72 |
| Frequency range | 1–8 MHz (cardiac 2–7 MHz; obstetric 3–7 MHz) |
| Volume rate (real-time) | 5–30 volumes/second |
| Volume rate (zoom, reduced aperture) | Up to 24–60 volumes/second |
| Pyramid angle | 30°×60° (narrow) to 90°×90° (full volume) |
- A 1D phased array steers in the azimuthal plane only → 2D fan image
- To get the elevation plane, the array would need to be mechanically tilted → too slow for real-time 3D
- The 2D matrix array steers electronically in BOTH planes → can sweep through the full pyramid within milliseconds → true real-time volume acquisition
2.2 ASIC Technology in 4D Probes
- Transmit beamforming: Time-delay chips apply precise sub-nanosecond delays to each element for focused transmit beam steering in both x and y directions
- Micro-receive beamforming: Elements are grouped into patches (~4×4 = 16 elements); partial beamforming summed within each patch → reduces cable count from ~3,000 to ~128 channels
- Low-noise amplification: Each element's receive signal amplified before digitisation, minimising noise
- High-voltage multiplexing: Transmit/receive (T/R) switches protect the sensitive receive electronics from high transmit voltages
- Power supply management: On-chip voltage regulation, thermal management
2.3 Mechanical 4D Probes
- A conventional 1D phased or curved array is mounted on a motor-driven pivot within the probe housing
- The motor continuously rocks (tilts) the array back and forth through the elevation plane
- Each complete sweep (one direction + return) generates one 3D volume
- The sweep repeats continuously → produces a 4D cine loop
- Sweep angle: 40°–85° elevation range
- Volume rate: 1–24 volumes/second (depends on sweep angle and depth)
- Frequency: 3–9 MHz (transvaginal), 2–8 MHz (transabdominal)
- Frame count per volume: 100–400 2D slices per sweep
2.4 GPU-Based Real-Time Rendering Engines
- Scan conversion: Transform pyramidal coordinates → Cartesian voxel grid
- Volume rendering: Ray-casting or texture-based projection with opacity mapping
- Real-time display: Repeat at 10–30 volumes/second
- Store the pyramidal volume directly as a 3D projective texture in GPU memory (no explicit Cartesian conversion needed)
- Use 3D projective texture mapping to perform ray-casting directly in pyramidal coordinates
- GPU fragment and vertex processors execute the opacity transfer function and compositing in parallel for every screen pixel simultaneously
- Result: Volume rendering at the rates required for cardiac 4D imaging — NVIDIA GPU Gems Ch. 40
2.5 4D Transducer Variants
| Probe Type | Technology | Application | Volume Rate |
|---|---|---|---|
| xMATRIX (Philips) | Full 2D matrix, 3000 elements | Cardiac TTE | 5–30 Hz |
| 4D TEE (miniaturised matrix) | Matrix in endoscope tip | Intraoperative cardiac | 5–20 Hz |
| Voluson E10 probe (GE) | Mechanical motor + curved array | OB/GYN 4D | 1–24 Hz |
| RM7C (mechanical) | Tilting curved array | Fetal 4D face/body | Up to 35 Hz |
| V6C (electronic matrix) | Reduced aperture matrix | Fast fetal 4D | Up to 60 Hz |
| High-density matrix (research) | 9000+ element full matrix | All applications | Variable |
SECTION 3: THE 4D ACQUISITION PIPELINE
START IN 2D B-MODE
↓
Select region of interest (ROI) and optimise 2D image
↓
Choose 4D acquisition mode (sector size, volume rate)
↓
ACQUIRE VOLUMETRIC DATA
├─ Single-beat real-time (cardiac)
├─ Multi-beat ECG-gated (cardiac)
├─ Mechanical sweep (OB/GYN)
└─ STIC (fetal cardiac)
↓
SCAN CONVERSION (pyramidal → Cartesian voxels)
↓
VOLUME RENDERING (GPU)
↓
DISPLAY (scrolling 4D cine loop)
↓
POST-PROCESSING + QUANTITATIVE ANALYSIS
SECTION 4: ACQUISITION METHODS IN DETAIL
4.1 Single-Beat Real-Time 4D (Cardiac)
- $c$ = speed of sound ≈ 1540 m/s
- $d$ = imaging depth (m)
- $N_{lines/volume}$ = number of scan lines per volume (proportional to pyramid width × line density)
| Mode | Pyramid Size | Volume Rate | Spatial Resolution | Best Use |
|---|---|---|---|---|
| Narrow sector | 30°×60° | Highest (~20–30 Hz) | Highest | Procedure guidance, real-time manipulation |
| Wide sector (Zoom) | User-defined ROI | Medium (~10–20 Hz) | Reduced | Valve visualisation, entire valve in one volume |
| Live Full-Volume | 90°×90° | Lowest (~3–8 Hz) | Reduced | Gross anatomy, arrhythmia patients |
4.2 Multi-Beat ECG-Gated 4D (Cardiac — Highest Quality)
- Regular sinus rhythm (RR interval variability <10 ms ideally)
- Breath-hold during acquisition
- No patient movement between beats
4.3 Mechanical Sweep 4D (Obstetric/Abdominal)
4.4 STIC (Spatiotemporal Image Correlation) — 4D Fetal Cardiac Imaging
4.4.1 STIC Acquisition Protocol
- The mechanical probe performs a slow, steady sweep through the fetal chest in the elevation direction over 7.5–15 seconds (user-selectable)
- During this sweep, ~200–400 2D B-mode frames are acquired with timestamps but no spatial position tracking
- Auto-detection of cardiac rate: The software analyses the periodic motion patterns (wall/valve motion) in the acquired frames to automatically detect the fetal heart rate — no ECG needed
- Retrospective temporal sorting: All frames are sorted according to their estimated phase within the cardiac cycle (systole or diastole) based on the detected rate
- Volume construction: Frames belonging to the same cardiac phase are assembled into a 3D volume; frames at the next phase into another volume; and so on until a full cardiac cycle is reconstructed
- Result: A 4D cine loop of 10–40 volumetric frames spanning one complete fetal cardiac cycle — can be played back repeatedly as a loop
4.4.2 STIC Technical Parameters
| Parameter | Value | Effect |
|---|---|---|
| Sweep time | 7.5–15 seconds | Longer → more frames, better temporal resolution |
| Sweep angle | 15°–40° elevation | Wider → larger chest volume covered |
| Frame rate during sweep | 50–120 Hz | Higher → more frames, better temporal resolution |
| Resulting 4D frames | 10–40 volumes/cardiac cycle | More = smoother motion playback |
| Fetal HR detection method | Autocorrelation of motion signal | Automatic, no ECG |
4.4.3 STIC Limitations and Failure Modes
- Fetal movement during sweep: Causes blurring and misregistration of cardiac phases
- High/irregular fetal HR: Difficult auto-detection of rate; unreliable sorting
- Poor acoustic window: Insufficient signal for cardiac motion detection
- Operator sweep speed: Must be slow, uniform, and straight in one direction
- Artefact: If HR is incorrectly estimated, cardiac structures appear at wrong phase → misdiagnosis risk
4.4.4 STIC Combined Modalities
| STIC Combination | What it shows |
|---|---|
| STIC + B-mode | Standard grey-scale 4D cardiac anatomy |
| STIC + Colour Doppler | 4D colour flow through cardiac structures |
| STIC + Power Doppler | 4D mapping of vascular flow, placental vascularity |
| STIC + VOCAL | Automated fetal cardiac chamber volume calculation |
| STIC + M-mode | Virtual M-mode through any plane in stored volume |
| STIC + Glass-body | Angiographic-style 4D rendering of cardiac vessels |
SECTION 5: SCAN CONVERSION (DATA TRANSFORMATION)
5.1 Coordinate Transformation
5.2 Interpolation Methods
| Method | Algorithm | Speed | Quality |
|---|---|---|---|
| Nearest-Neighbour | Assign each voxel the value of its closest acquired sample | Fastest | Blocky; adequate for real-time |
| Trilinear | Weighted average of 8 surrounding samples | Fast | Smooth; standard for clinical 4D |
| Gaussian kernel | Weighted sum using Gaussian function of distance | Moderate | Better SNR; smooth |
| Spline / RBF | Fitted smooth function | Slow | Best quality; offline only |
5.3 Direct Pyramidal Rendering (No Explicit Scan Conversion)
- The pyramidal volume is stored directly in GPU memory as a 3D projective texture
- Ray-casting is performed in the original pyramidal coordinate system
- The GPU's projective texture sampling hardware handles the geometric transformation implicitly
- Advantage: eliminates the scan conversion step, saving time and memory — NVIDIA GPU Gems Ch. 40
SECTION 6: VISUALISATION AND DISPLAY MODES
6.1 Real-Time 4D Cine Loop Display
- Volume rate (Hz): Adjusted by sector size and depth
- Playback speed: Can replay stored 4D loops at slower speed for detailed review
- Rotation: Volume can be rotated in any direction during real-time display
- Cropping: A virtual cut-plane reveals internal anatomy (e.g., remove anterior wall → view mitral valve)
6.2 Volume Rendering (The Primary 4D Rendering Method)
- Anechoic blood → transparent (rendered invisible) → cavity appears empty (black)
- Myocardium/tissue → semi-transparent, orange/amber → structures appear solid
- Highly echogenic structures (calcium, valve leaflets, sutures) → opaque, bright → rendered prominently
- Perspective projection: Structures closer to the virtual camera appear larger
- Phong shading: A virtual light source illuminates the scene — near surfaces are bright, shadowed areas create depth
- Transparency compositing: Semi-transparent tissues show underlying anatomy
6.3 Surface Rendering in 4D
- At each time frame, the endocardial (or epicardial) border is detected (semi-automatically or automated)
- The surface is rendered as a solid, lit mesh
- As the 4D loop plays, the surface appears to contract and expand — showing myocardial motion
- Used for: LV endocardial motion, fetal face movement, fetal limb motion, valve leaflet morphology
6.4 Multiplanar Reconstruction (MPR) in 4D
- Navigate to end-diastole or end-systole and measure dimensions at precisely those phases
- Extract virtual planes that were never available physically (e.g., true coronal plane of fetal chest)
- Play the MPR cine to watch one plane's anatomy changing through the cardiac cycle
- Simultaneous triplane MPR: Three orthogonal planes shown simultaneously, all animating through the cardiac cycle
6.5 Volume Contrast Imaging (VCI)
- Rather than projecting through the entire volume, a thin slab of voxels (typically 3–8 mm thick) is projected
- The maximum, minimum, or average of the slab is displayed as a 2D image
- VCI-A (coronal plane): Renders a thick coronal slice, equivalent to viewing a "slice" of the volume from above — produces images with dramatically improved contrast resolution vs. standard 2D
- VCI-A in real time: The ultra-fast volume rate of modern probes (e.g., Voluson E10) allows VCI-A to be used live as a standard real-time mode, improving imaging of fetal brain, extremities, or heart in difficult patients
6.6 Glass Body / Inversion Mode
- Colour/power Doppler is acquired within the 4D volume
- The grey-scale anatomy is made transparent; only the Doppler signal is displayed
- Result: an "angiographic" 4D rendering showing only moving blood — a pulsating vascular tree
- Clinical uses: Placental vascularity mapping, intrahepatic flow, tumour vascularity, fetal cardiac outflows
- Inverts the signal intensity: anechoic (fluid) becomes bright; echogenic tissue becomes dark
- Fluid-filled structures (cysts, cardiac chambers, bladder, renal pelvis) appear as bright solid masses
- Allows volume calculation of fluid-filled organs without manual tracing
- Clinical: fetal stomach volume, amniotic fluid pockets, LV volume, renal pelvis volume
6.7 4D LV Quantification Display (Cardiac)
- Acquire full-volume gated 4D dataset (4–6 beats)
- Place landmark points (apex, mitral annulus) in one or two frames
- Software propagates endocardial surface detection across all time frames using active appearance models or deformable mesh tracking
- LV volume is calculated at each time point without geometric assumptions
- Volume-time curve displayed: LV volume (y-axis) vs. cardiac cycle phase (x-axis) — shows full volume excursion
- Output: EDV, ESV, EF, SV, CO, dV/dt (rate of volume change)
6.8 Parametric 4D Display — Regional Function Maps
- LV divided into 17-segment AHA model
- Each segment's parameter colour-coded on a flat disc (apex at centre, base at periphery)
- Parameters: time-to-minimum volume, regional EF, wall thickening, radial displacement
- Synchrony map: Colour shows timing of peak contraction per segment — used to identify dyssynchrony for CRT (cardiac resynchronization therapy) selection
- Software tracks speckle patterns frame-to-frame through the 4D dataset
- Derives regional myocardial deformation: longitudinal strain, circumferential strain, radial strain, area strain
- Displayed as colour-coded maps on the 3D LV surface, animating through the cardiac cycle
- More comprehensive than 2D strain (covers all segments without foreshortening)
SECTION 7: THE FUNDAMENTAL 4D TRADEOFF — TEMPORAL vs. SPATIAL vs. VOLUME
| To improve volume rate | Consequence |
|---|---|
| Reduce depth | May lose far-field anatomy |
| Reduce pyramid angle | Narrower FOV |
| Reduce line density | Worse lateral resolution |
| Use multi-beat gating | Requires regular rhythm; stitch artifacts |
| Use reduced aperture | Worse spatial resolution |
| Use parallel receive beamforming | Increased hardware complexity |
| Application | Minimum Volume Rate Needed | Reason |
|---|---|---|
| Fetal face 4D | 5–10 Hz | Slow facial movements |
| Fetal limb 4D | 10–15 Hz | Moderate speed movement |
| Fetal cardiac 4D (STIC) | N/A (retrospective gating) | Inherently high HR (~150 bpm) |
| Adult cardiac 4D | 15–25 Hz | HR ~70 bpm; need ≥5 frames/cycle |
| LV EF quantification | 25–30 Hz minimum | Need to capture end-systole accurately |
| Valve dynamics (transcatheter guidance) | ≥20 Hz | Rapid leaflet motion |
| 3D Colour Doppler | 5–10 Hz | Reduced PRF for colour acquisition |
"The number of volumes per second required for imaging a fetal face is far less than the number required for imaging the human heart — the heart moves rapidly and we need several 3D volumes per cardiac cycle to adequately visualise heart motion." — NVIDIA GPU Gems, Sumanaweera
SECTION 8: ARTIFACTS SPECIFIC TO 4D IMAGING
| Artifact | Appearance in 4D | Mechanism | Solution |
|---|---|---|---|
| Stitch artifact | Vertical discontinuity across cine loop | Sub-volume misregistration from arrhythmia/movement | Regular rhythm, breath-hold; use single-beat mode |
| Temporal smearing | Blurred valve or wall at fast events | Volume rate too low to capture rapid motion | Reduce sector size, increase volume rate |
| STIC misregistration | Structural phantom/ghost in wrong phase | Incorrect fetal HR detection during STIC | Repeat acquisition; avoid fetal movement |
| Dropout | Holes in solid surfaces (valve, myocardium) | Beam parallel to structure; insufficient gain | Optimise gain; different acquisition angle |
| Side-lobe clutter | False structures adjacent to bright reflectors | Grating lobes from large element spacing | Intrinsic to array design; reduce gain |
| Ghost volumes | Duplicated moving structures | Beat-to-beat cardiac position variation during gating | Ensure stable transducer position |
| Temporal aliasing | Jerky, discontinuous motion in cine loop | Too few volumes per cardiac cycle | Increase volume rate, reduce sector size |
| Reduced frame rate with colour | Slow, jerky 4D colour flow loop | Colour acquisition requires multiple pulses per line | Use gated acquisition for colour 4D |
SECTION 9: POST-PROCESSING AND OFFLINE ANALYSIS
9.1 Virtual Planes Navigation
- Scroll through any 2D plane (A/B/C) at any cardiac phase
- Equivalent to having acquired any 2D scan plane during the examination — "virtual rescan"
- Critical for: fetal anomaly re-review, missed views, operator re-learning
9.2 VOCAL (Virtual Organ Computer-aided AnaLysis)
- Operator places a reference point within the fetal heart at a defined phase
- Software automatically segments the cardiac chamber at multiple rotational planes
- Calculates chamber volume, myocardial volume, cardiac output
- Used for: Fetal cardiac function assessment, hydrops evaluation
9.3 4D Auto LVQ / HeartModel (Cardiac)
- Automated software (Philips HeartModel, GE 4D AutoLVQ) fully automated endocardial detection across all 4D frames without manual interaction
- Produces: EDV, ESV, EF, wall motion score, synchrony analysis
- Research-grade accuracy correlating with MRI
9.4 M-Mode from 4D Dataset
- A virtual M-mode can be reconstructed from any stored 4D dataset by extracting a single scan-line's time-amplitude trace across the cardiac cycle
- Provides temporal resolution equivalent to real M-mode from planes never physically acquired
SECTION 10: 4D DOPPLER IMAGING
10.1 4D Colour Flow Doppler
- The matrix array acquires colour Doppler data simultaneously across the full pyramidal volume
- Each scan line requires 8–16 transmit pulses (burst length) for autocorrelation → volume rate drops significantly (typically 2–8 Hz for 4D colour)
- Best acquired with multi-beat ECG gating to overcome low volume rate
- Display: Colour-coded flow animated within the 3D volume
- Clinical: Paravalvular leak localisation (360° spatial view), ASD/VSD shunt direction, intracardiac catheter guidance
10.2 4D Power Doppler (Glass-Body Mode)
- Power Doppler (amplitude-only, no velocity direction) is acquired within the volume
- All grey-scale rendered transparent → only flow signal shown as coloured vascular tree
- No aliasing (power Doppler is angle-independent and has no Nyquist limit for display)
- Applications: Placental blood flow assessment, hepatic vasculature, tumour angiogenesis mapping
SECTION 11: CLINICAL APPLICATIONS OF 4D ULTRASOUND
11.1 Obstetrics and Fetal Medicine
| Application | Method | Clinical Value |
|---|---|---|
| Fetal face | RT-4D mechanical sweep | Cleft lip/palate, parent bonding |
| Fetal body movements | RT-4D | Biophysical profile scoring |
| Fetal cardiac anatomy | STIC 4D | CHD screening, surgical planning |
| Fetal cardiac function | STIC + VOCAL | Cardiomyopathy, hydrops, arrhythmia |
| Fetal limbs and spine | RT-4D | Skeletal dysplasia, neural tube defects |
| Placental vascularity | 4D Power Doppler (glass-body) | Placenta accreta spectrum, molar pregnancy |
| Fetal CNS | STIC-derived neurosonogram | Corpus callosum, cerebellar vermis |
11.2 Cardiac (Adult Echocardiography)
| Application | Method | Clinical Value |
|---|---|---|
| LV EF + volumes | Full-volume gated 4D | Most accurate; MRI-equivalent |
| RV volume/function | Full-volume 4D | RV is non-geometric; 4D is only accurate method |
| Mitral valve prolapse | RT-4D zoom; surface rendering | Map exact prolapsing scallop |
| Mitral valve TAVI planning | Full-volume + MPR | Annulus area, perimeter, commissure anatomy |
| Paravalvular leak | 4D colour Doppler | 3D localisation for transcatheter closure |
| ASD/VSD guidance | RT-4D TEE | Real-time device positioning |
| Dyssynchrony | 4D LV parametric maps | CRT patient selection |
| Cardiac thrombus | RT-4D | 3D confirmation, extent mapping |
11.3 Other Applications
| Specialty | Application |
|---|---|
| Gynaecology | Uterine anomalies; IUD position; endometrium |
| Vascular | 4D CEUS of endoleak; 4D carotid imaging |
| Breast | Lesion vascularity; biopsy guidance |
| Musculoskeletal | Dynamic joint assessment; neonatal hip 4D |
| Interventional | Real-time 4D TEE guidance of structural heart procedures |
SECTION 12: COMPARISON — 2D vs 3D vs 4D
| Feature | 2D | 3D (Static) | 4D (RT-3D) |
|---|---|---|---|
| Spatial dimensions | x, y | x, y, z | x, y, z |
| Temporal dimension | Yes (video) | No (single frame) | Yes (cine loop of volumes) |
| Frame rate | 50–100 Hz | — | 5–30 Hz (volume rate) |
| Anatomy captured | One plane at a time | Full volume (one instant) | Full volume through time |
| LV EF accuracy | Moderate (geometric assumption) | Good | Best (no assumptions) |
| Procedural guidance | Yes | Limited | Yes (RT-4D TEE) |
| Requires gating | No | Only for high-res | For high-res (or single-beat) |
| Operator skill needed | Standard | High | High |
| Acoustic window req. | Standard | Stricter | Stricter |
| Post-acquisition re-analysis | No (re-scan needed) | Yes (any plane) | Yes (any plane + any time point) |
SECTION 13: HIGH-YIELD EXAM SUMMARY
- 4D = 3D + time: A continuously updated sequence of 3D volumes; each voxel has position (x,y,z) + time
- Instrumentation: Matrix array (2D grid of elements); ASIC micro-beamforming (reduces 3000 cables → 128 channels); dedicated GPU for real-time volume rendering
- Mechanical 4D probes (OB/GYN): Motor-driven tilt of 1D array; 1–35 Hz; not fast enough for adult cardiac
- Electronic matrix 4D (cardiac): Full electronic beam-steering; 5–30 Hz; can reduce aperture for 60 Hz
- Three single-beat RT-4D modes: Narrow (best temporal/spatial; small FOV) → Zoom (larger FOV; reduced) → Full-volume (largest FOV; worst temporal/spatial)
- Multi-beat gated 4D: Overcomes the tradeoff; N beats = N× better volume rate; requires regular rhythm; vulnerable to stitch artifact
- STIC: Slow mechanical sweep (7.5–15 s); retrospective cardiac phase sorting from motion detection (no ECG); produces 4D cardiac cine loop; can combine with colour/power Doppler/VOCAL
- GPU rendering: 3D projective texture mapping for real-time volume rendering of pyramidal data — avoids explicit scan conversion
- Volume rendering transfer function: Maps grey-value → opacity + colour; anechoic = transparent; tissue = semi-opaque amber; calcified = opaque white
- 4D LV EF: Automated endocardial detection through all cardiac phases; EDV, ESV, EF without geometric assumptions; volume-time curve; correlates with MRI
- 4D colour Doppler (Glass Body): Power Doppler rendered in 3D; all grey-scale transparent; angiographic vascular tree display; used for placenta, cardiac shunts
- Inversion mode: Anechoic fluid made bright; used for volume calculation of fluid-containing organs
- STIC failure causes: Fetal movement, irregular fetal HR, poor acoustic window, non-uniform sweep
- Volume rate minimum: Fetal face 5 Hz; fetal cardiac via STIC (retrospective); adult cardiac 15–25 Hz minimum for diagnostic quality
- VCI-A: Thick-slab coronal projection from 4D volume; improved contrast resolution; used in real-time mode on modern machines
References
- Miller's Anesthesia 10e — Real-Time Three-Dimensional Imaging, Gated Acquisition, 3D Colour Flow
- Textbook of Clinical Echocardiography — THREE-DIMENSIONAL ECHOCARDIOGRAPHY (acquisition modes, display types, stitch artifact)
- Barash's Clinical Anesthesia 9e — 3D TEE volume rendering, procedural guidance
- Fuster & Hurst's The Heart 15e — 3D/4D echocardiography, LV volume/EF, MRI correlation
- Creasy & Resnik's Maternal-Fetal Medicine — STIC fetal echocardiography for CHD
- Sumanaweera T. Chapter 40: Applying Real-Time Shading to 3D Ultrasound Visualization. NVIDIA GPU Gems — pyramidal grid volume rendering, GPU projective texture mapping
- Volume Sonography Core Concepts for Clinical Practice — 4D definitions, mechanical probe types, VCI, glass-body mode, VOCAL (ObgynKey)
- MIT CSAIL Real-Time 4D Ultrasound Reconstruction Thesis — prospective/retrospective gating, RT3D systems