Blood and mucus in stools loose multiple episodes per day with blood sometimes bright and sometimes dark
Reading File
Finding Sources
Finding Sources
Searching PubMed
bloody diarrhea mucus stool differential diagnosis management
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a thorough, well-sourced answer. Here it is:
Blood and Mucus in Stools - Multiple Loose Episodes Per Day
This presentation - bloody, mucus-containing loose stools with multiple episodes per day and blood that varies between bright red and dark - is a classic picture of inflammatory diarrhea (colitis). The combination of blood + mucus + frequency points strongly to mucosal disease of the colon or rectum. Here is a structured clinical approach.
Understanding the Blood Color
The color of blood in stool reflects the site of bleeding:
- Bright red blood = lower colorectum, rectum, or anus (distal source; rapid transit)
- Dark red/maroon blood = more proximal colon or right colon (slower transit, partial degradation of hemoglobin)
- Both colors in same patient = either disease spanning multiple colonic segments, or variable transit speed during an active flare
Key Differential Diagnosis
The presence of blood AND mucus together narrows the differential significantly toward causes of colitis (mucosal inflammation). The major categories are:
1. Inflammatory Bowel Disease (IBD)
Ulcerative Colitis (UC) is the most important diagnosis to consider.
"The major symptoms of UC are diarrhea, rectal bleeding, tenesmus, passage of mucus, and crampy abdominal pain."
- Harrison's Principles of Internal Medicine 22E, p. 2599
- Patients with proctitis pass fresh blood or blood-stained mucus, either mixed with stool or streaked on the surface of a normal stool, along with tenesmus (urgent, incomplete defecation).
- When disease extends beyond the rectum, blood is usually mixed with stool or there is grossly bloody diarrhea.
- With severe disease, the patient passes liquid stool containing blood, pus, and fecal matter. Diarrhea is often nocturnal and/or postprandial.
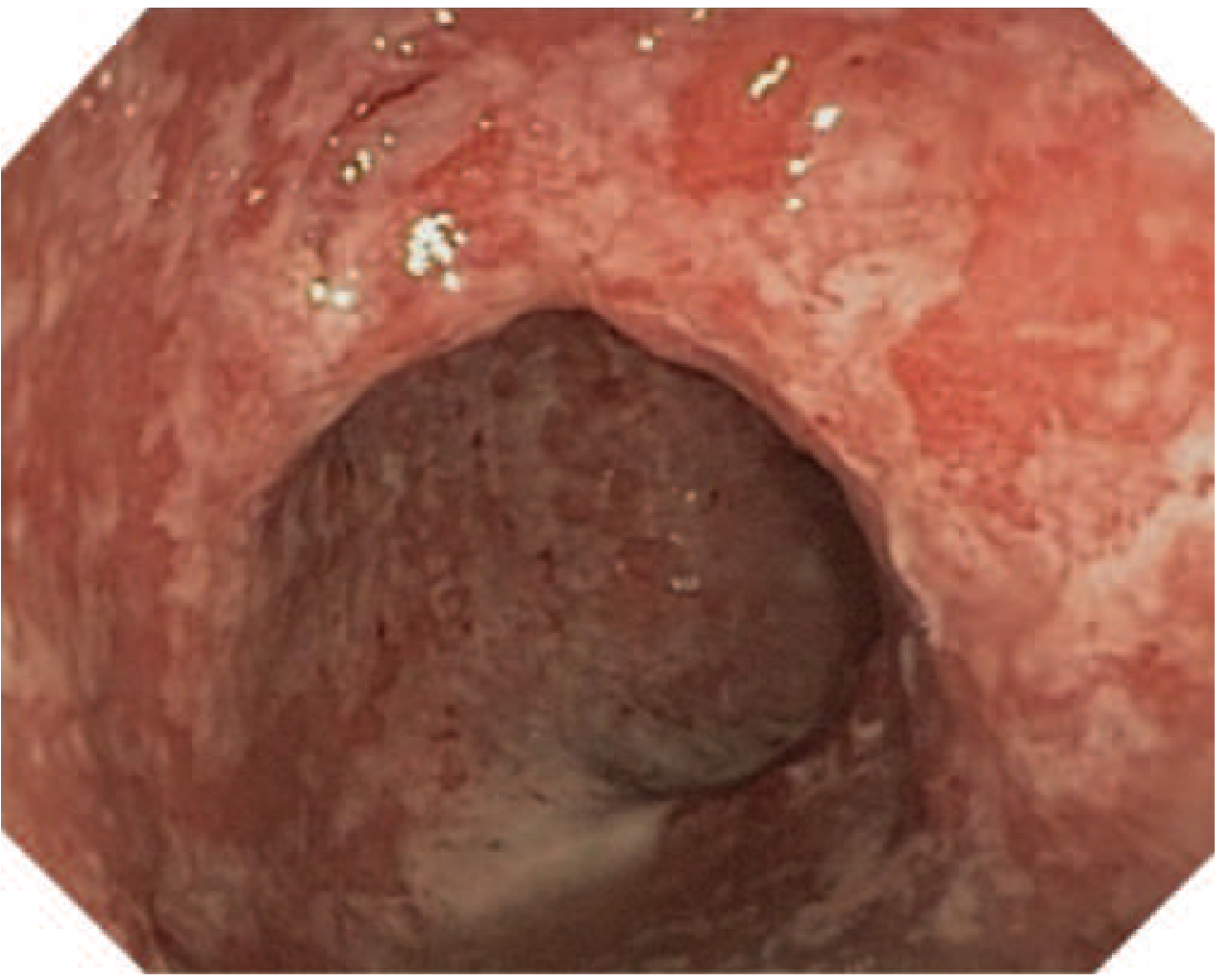
Colonoscopy in acute UC shows erythema, friability, loss of vascular pattern, erosions, and ulcerations:
Severity classification (Montreal):
| Severity | Definition |
|---|---|
| S1 - Mild | ≤4 stools/day (with or without blood), no systemic illness, normal ESR |
| S2 - Moderate | ≥4 stools/day, minimal systemic toxicity |
| S3 - Severe | ≥6 bloody stools/day, pulse ≥90/min, temp ≥37.5°C, Hb <10.5 g/dL, ESR ≥30 mm/h |
Crohn's Disease (CD) of the colon can also cause bloody diarrhea with mucus, though gross rectal bleeding is less common than in UC. CD may have skip lesions, perianal disease, and fistulas as additional features.
2. Infectious Colitis (must be ruled out first)
This is the most important initial differential, especially in acute presentations.
"Infections with organisms such as Salmonella, Shigella, Amoeba, Giardia, E. coli O157:H7, and Campylobacter can be accompanied by bloody diarrhea, abdominal cramps, and an endoscopic mucosal appearance identical to that of ulcerative colitis."
- Goldman-Cecil Medicine, p. 1493
Key infectious causes of bloody mucoid diarrhea:
| Pathogen | Notes |
|---|---|
| Shigella | Classic dysentery; endoscopy can look identical to UC |
| Entamoeba histolytica (amoebiasis) | Prolonged course; flask-shaped ulcers in cecum/ascending colon covered with yellow exudate; can mimic IBD |
| Campylobacter jejuni | Common bacterial cause; endoscopy resembles UC |
| E. coli O157:H7 | Enterohemorrhagic; can cause hemolytic uremic syndrome |
| Clostridioides difficile | Especially post-antibiotic; pseudomembranous colitis |
| Salmonella | Bloody diarrhea, fever |
| Yersinia | Can mimic Crohn's (terminal ileum involvement) |
The key distinction between infection and IBD: infectious diarrhea is typically limited to days-to-weeks; IBD symptoms are of longer duration (weeks to months). However, stool cultures and PCR panels must be done before starting IBD-specific treatment.
3. Ischemic Colitis
- Typically in elderly patients with cardiovascular risk factors (or young patients on vasoconstrictive drugs)
- Blood in stool, but usually less profuse
- Classically affects the "watershed" areas (splenic flexure, sigmoid), and the rectum is typically spared (distinguishing it from UC, which always involves the rectum)
- Yamada's Textbook of Gastroenterology, 7th Edition
4. Colorectal Cancer / Polyps
- Passage of blood clots is unusual in UC; if present, suggests other diagnoses such as tumor
- Chronic dark blood mixed with stool, weight loss, and change in bowel habits - particularly in older adults
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease
5. Other Causes
- Radiation colitis - history of pelvic/abdominal radiotherapy
- Microscopic colitis (collagenous/lymphocytic) - watery diarrhea, usually no visible blood, normal endoscopy
- Diverticular bleeding - usually brisk bright red bleeding without significant mucus or inflammation
Immediate Workup
History:
- Duration of symptoms (acute vs. chronic)
- Travel history, antibiotic use, sexual history
- Prior episodes, family history of IBD or colorectal cancer
- Fever, weight loss, night sweats
Stool Studies (first step):
- Stool culture (bacterial pathogens: Shigella, Salmonella, Campylobacter, E. coli O157:H7)
- Stool PCR/GI panel (nucleic acid amplification test)
- C. difficile toxin PCR
- Ova and parasites (for Entamoeba histolytica, Giardia)
- Fecal white blood cells or fecal lactoferrin/calprotectin (marker of mucosal inflammation)
Blood Tests:
- CBC (anaemia, leukocytosis)
- CRP and ESR (inflammatory markers)
- Serum albumin (low in severe IBD)
- U&E/renal function (electrolyte derangement from diarrhea)
Imaging:
- Abdominal X-ray (exclude toxic megacolon: transverse colon diameter >6 cm)
- CT abdomen/pelvis if severe or uncertain
Endoscopy:
- Colonoscopy is the definitive investigation for IBD and to exclude malignancy
- Should be done after infectious causes are ruled out unless urgently needed
- Biopsies are essential for histopathological diagnosis
- Goldman-Cecil Medicine, p. 1499-1500
Management Overview
If Infectious - treat the cause:
- Shigella, Campylobacter: fluoroquinolone (ciprofloxacin) or azithromycin
- Amoebic dysentery: metronidazole followed by luminal agent (diloxanide furoate)
- C. difficile: oral vancomycin or fidaxomicin
If UC - based on severity:
- Mild-Moderate disease:
- 5-ASA (mesalamine) oral ± topical (enemas for distal disease)
- Sulfasalazine 3-6 g/day or mesalamine 2.4-4.8 g/day
- Topical mesalamine enemas more effective for distal colitis
- Moderate-Severe disease:
- Oral prednisone 40-60 mg/day
- IV hydrocortisone 300 mg/day or methylprednisolone 40-60 mg/day for hospitalised patients
- Budesonide MMX (Uceris) 9 mg/day is an option with fewer systemic effects
- Steroid-refractory/dependent disease:
- Biologics: anti-TNF agents (infliximab, adalimumab), integrin inhibitors (vedolizumab), IL-12/23 inhibitors (ustekinumab)
- Thiopurines (azathioprine, 6-MP) for maintenance
- Surgical (colectomy) for refractory disease, toxic megacolon, perforation, or dysplasia/cancer
Harrison's Principles of Internal Medicine 22E, pp. 2603-2610; Sleisenger and Fordtran's GI and Liver Disease
Red Flag Features Requiring Urgent/Emergency Assessment
- ≥6 bloody stools per day
- Fever >37.5°C
- Tachycardia (pulse >90/min)
- Haemoglobin <10.5 g/dL
- Marked abdominal tenderness or distension (risk of toxic megacolon)
- Signs of peritonitis
- Passage of blood clots (raises concern for tumour or severe haemorrhage)
Bottom line: Blood and mucus in multiple loose stools per day is colitis until proven otherwise. Infectious causes must be excluded with stool studies first. If negative, the most likely diagnosis is ulcerative colitis, and colonoscopy with biopsy is needed to confirm extent, severity, and guide treatment. Urgent assessment is warranted if any of the red flag features above are present.
Disclaimer: This information is for educational purposes. Any patient with these symptoms should be evaluated promptly by a clinician for proper diagnosis and individualised management.
It's is chronic from nearly 2 months
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
I have everything I need. Here is the focused update given the 2-month chronic course:
Chronic Course (2 Months) - Revised Clinical Assessment
Two months of continuous bloody, mucus-laden loose stools with multiple episodes per day is well beyond the typical self-limiting window of infectious gastroenteritis. This duration fundamentally reshapes the differential.
What 2 Months of Symptoms Tells You
"An important distinction between acute bacterial infections and ulcerative colitis is that the diarrhea in infectious diseases tends to be limited to a period of days to a few weeks, whereas the diarrhea of ulcerative colitis is typically of longer duration."
- Yamada's Textbook of Gastroenterology, 7th Edition
- Most bacterial causes (Shigella, Campylobacter, Salmonella) resolve within 1-3 weeks
- 2 months of persistent symptoms essentially rules out common acute bacterial infections
- Protozoal infections (especially amoeba) and IBD are now the front-runners
Revised Priority Differential
1. Ulcerative Colitis (UC) - Most Likely
This presentation is the textbook picture of active UC:
- Chronic diarrhea with blood and mucus
- Multiple episodes per day
- Duration >4 weeks with no infectious cause
Based on stool frequency alone, this patient likely falls in the moderate-to-severe range (≥4-6 bloody stools/day).
By the Montreal Classification:
| Severity | Stool Frequency | Systemic Features |
|---|---|---|
| Mild (S1) | ≤4/day ± blood | No systemic illness, normal inflammatory markers |
| Moderate (S2) | ≥4/day | Minimal systemic toxicity |
| Severe (S3) | ≥6 bloody/day | Pulse ≥90, Temp ≥37.5°C, Hb <10.5 g/dL, ESR ≥30 mm/h |
Harrison's Principles of Internal Medicine 22E
2. Chronic Intestinal Amoebiasis (Entamoeba histolytica)
- Can cause prolonged illness lasting weeks-to-months
- Bloody diarrhea with mucus, colicky abdominal pain
- Ulcers characteristically in the cecum and ascending colon (covered with yellow exudate), but can be anywhere
- Endoscopy may look similar to IBD
- Critical point: If missed and patient is given steroids for presumed UC, amoebiasis can rapidly disseminate and become life-threatening
- Must be excluded before starting immunosuppression
3. Intestinal Tuberculosis
- Particularly relevant in TB-endemic regions (South Asia, Sub-Saharan Africa)
- Can present with chronic diarrhea, blood in stool, weight loss, night sweats, low-grade fever
- Primarily involves ileocecal region; can closely mimic Crohn's disease
- Must be excluded before starting biologics/immunosuppressants
4. Crohn's Disease (Colonic)
- Less commonly presents with gross rectal bleeding than UC
- Consider if there are: perianal disease (fistulas, skin tags), upper GI symptoms, skip lesions, or weight loss out of proportion
5. Colorectal Cancer
- 2 months of rectal bleeding in adults (especially >40 years) warrants exclusion
- Particularly if there is significant weight loss, family history, or change in stool calibre
Priority Investigation Plan
Given 2 months duration, this patient needs urgent investigation, not just empirical treatment.
Step 1 - Bloods (same day)
- CBC - check haemoglobin (anaemia from chronic blood loss), WBC, platelets
- CRP and ESR - elevated in active IBD and infection
- Serum albumin - low in severe/prolonged IBD; nutritional marker
- LFTs, U&E, renal function
- Blood cultures if febrile
Step 2 - Stool Studies (send immediately)
- Stool microscopy for trophozoites of Entamoeba histolytica (3 fresh samples on different days for maximum sensitivity)
- Stool culture - bacterial pathogens
- Stool PCR/GI multiplex panel - covers bacteria, parasites, viruses in one test
- C. difficile toxin PCR
- Fecal calprotectin - highly sensitive marker of mucosal inflammation; elevated in IBD and infectious colitis, helps distinguish from IBS
- Ova and parasites - Giardia antigen
Step 3 - Imaging
- Plain abdominal X-ray - look for toxic megacolon (transverse colon >6 cm), free gas under diaphragm, or faecal loading
- CT abdomen/pelvis with contrast - if severe, to assess extent of colitis, complications, and exclude perforation or abscess
Step 4 - Endoscopy (once infection excluded or as urgent)
- Colonoscopy with biopsy is the definitive investigation
- Biopsies distinguish UC from Crohn's from amoebic colitis from TB from CMV colitis histologically
- Goldman-Cecil Medicine: "Colonoscopy is the initial endoscopic test for patients who present with lower GI symptoms such as diarrhea and hematochezia"
Step 5 - TB Workup (if in endemic region or high suspicion)
- Chest X-ray
- Mantoux/TST or IGRA (QuantiFERON-TB Gold)
- Tissue biopsy PCR for TB from colonoscopy specimens
Management - Once Infectious Causes Excluded
If Amoeba Confirmed:
- Metronidazole 400-800 mg three times daily for 5-10 days (tissue amoebicide)
- Followed by luminal agent: diloxanide furoate 500 mg three times daily for 10 days (to clear intestinal cysts)
If UC Confirmed - Treatment Based on Severity:
Mild-Moderate UC:
- 5-ASA (mesalamine) is first-line
- Oral mesalamine 2.4-4.8 g/day
- If distal colitis: add mesalamine enemas (rectal) - combination oral + topical is more effective than either alone
- Sulfasalazine 3-6 g/day is an alternative (cheaper, but more side effects)
Moderate-Severe UC:
- Oral prednisolone 40-60 mg/day - most require this to induce remission
- Once remission achieved, taper slowly and transition to maintenance with 5-ASA or azathioprine
- Harrison's 22E: "The majority of patients with moderate to severe UC benefit from oral or parenteral glucocorticoids"
Severe/Hospitalised UC:
- IV methylprednisolone 40-60 mg/day or IV hydrocortisone 300 mg/day
- IV fluids, correct anaemia (blood transfusion if Hb <8 g/dL)
- DVT prophylaxis (IBD patients have elevated thrombotic risk)
- Nutritional support
- If no response in 3-5 days: rescue therapy with infliximab (anti-TNF) or ciclosporin
- If medical therapy fails: urgent colectomy
Maintenance (after remission):
- Mesalamine long-term for UC
- If steroid-dependent: azathioprine or 6-mercaptopurine
- If moderate-severe with biologic need: infliximab, adalimumab, vedolizumab, or ustekinumab
- Goodman & Gilman's: Mesalamine for induction and maintenance of remission in mild-to-moderate UC; combination with glucocorticoids for severe UC
Warning Signs Requiring Same-Day Hospital Admission
At 2 months of symptoms, complications are a real concern. Go to hospital urgently if:
- Fever above 38°C
- Pulse >90 beats/minute
- Abdominal distension or severe tenderness
- Passing >6 bloody stools in one day
- Haemoglobin dropping (pallor, breathlessness, dizziness)
- Significant weight loss (>5-10% body weight)
- Signs of dehydration (dry mouth, reduced urine output)
The most feared complication is toxic megacolon - a life-threatening dilation of the colon requiring emergency surgery.
Practical Next Step
The single most important action right now is:
- See a gastroenterologist urgently - do not start corticosteroids empirically without excluding amoeba and TB first
- Send stool samples (culture, microscopy for amoeba, C. diff PCR, calprotectin)
- Blood tests today - CBC, CRP, albumin, ESR
- Colonoscopy with biopsy to be arranged as soon as possible (or urgently if severe)
Disclaimer: This is clinical educational information only. A patient with 2 months of bloody diarrhea needs prompt evaluation by a physician - please seek medical care urgently.
No signs of dehydration There is dizziness while standing history of fever and chills with severe colicky pain in left side of abdomen
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
I now have all the key information. Here is the focused clinical update:
Updated Assessment - Significant Escalation in Severity
The new features change this from a "needs urgent outpatient workup" to a "needs hospital assessment today" situation.
Clinical Interpretation of New Symptoms
Dizziness on Standing = Orthostatic Hypotension
This is a critical finding. In the context of 2 months of chronic rectal bleeding, it most likely signals significant anaemia from chronic blood loss, not dehydration.
- Two months of daily bloody stools = slow but continuous haemorrhage
- The body compensates for gradual blood loss, masking obvious signs of dehydration (mucous membranes may still look normal)
- But when the patient stands, the cardiovascular system cannot maintain perfusion against gravity - hence dizziness
- This is a red flag for haemoglobin likely <8-9 g/dL (moderate-severe anaemia)
"Tachycardia and hypotension may be present secondary to dehydration or anaemia from chronic blood loss."
- Tintinalli's Emergency Medicine
Fever and Chills = Systemic Inflammation / Possible Infection
Fever in the context of active colitis means one of three things:
- Severe active IBD itself (systemic inflammatory response) - fever is one of the Montreal S3 severity criteria for UC
- Superimposed infection on top of IBD (e.g. C. difficile flare, CMV colitis)
- Complication - colonic perforation, abscess formation, or bacteraemia from translocation through a damaged colonic wall
Chills alongside fever suggest a bacteraemic or septic process - the inflamed, ulcerated colon mucosa allows gut bacteria to leak into the bloodstream.
Severe Left-Sided Colicky Pain
- Left-sided abdominal pain in bloody diarrhea = sigmoid colon and descending colon involvement
- This is the classic distribution of ulcerative colitis (starts at rectum, extends proximally - left-sided disease is the most common pattern)
- "Colicky" pain that precedes and is partially relieved by defecation is typical of colonic inflammation
- Severe colicky pain with fever raises concern for:
- Severe/fulminant colitis
- Early toxic megacolon (transverse colon dilation >6 cm with fever, abdominal pain, systemic inflammation)
- Colonic perforation (sudden severe pain, peritoneal signs)
"Toxic megacolon is a complication of severe ulcerative colitis in which large bowel dilation is present on abdominal radiograph or CT in the setting of fever, abdominal pain, and laboratory markers of systemic inflammation. Treatment requires hospital admission."
- Tintinalli's Emergency Medicine
Revised Severity Assessment
Mapping this patient against the Montreal S3 (Severe UC) criteria:
| Criterion | Status |
|---|---|
| ≥6 bloody stools/day | Likely (multiple per day) |
| Pulse ≥90/min | Unknown - but dizziness on standing suggests it |
| Temperature ≥37.5°C | YES - fever and chills reported |
| Hb <10.5 g/dL | Probable - dizziness on standing from anaemia |
| ESR ≥30 mm/h | Probable given systemic symptoms |
This patient meets probable criteria for SEVERE disease (S3).
Immediate Actions Required
This patient needs hospital admission today. Do not delay.
What Will Happen in Hospital
On Arrival - Emergency Assessment:
- Vital signs - lying and standing blood pressure (confirm orthostatic drop), pulse rate, temperature, oxygen saturation
- IV access established immediately
- Urgent bloods:
- Full blood count - haemoglobin level (expect low), WBC, platelets
- CRP and ESR
- Serum electrolytes (Na, K, Cl, bicarbonate)
- Renal function (urea, creatinine)
- Serum albumin
- Blood cultures (×2 sets, given fever and chills)
- Coagulation screen
- Group and screen (for possible transfusion)
- Stool samples:
- C. difficile toxin PCR (urgent - superimposed C. diff on IBD is common and worsens outcome)
- Stool culture
- Microscopy for Entamoeba histolytica
- Abdominal X-ray - rule out toxic megacolon (transverse colon >6 cm), free air under diaphragm (perforation)
- CT abdomen/pelvis with contrast - assess extent of colitis, bowel wall thickening, free fluid, abscess
Inpatient Treatment:
If Haemoglobin <7-8 g/dL:
- Blood transfusion
If Severe Active Colitis (UC most likely):
- IV methylprednisolone 40-60 mg/day OR IV hydrocortisone 100 mg four times daily
- IV fluids and electrolyte correction
- Nutritional support (high-protein diet or nasogastric feeding if not tolerating food)
- DVT prophylaxis (IBD carries increased clotting risk)
- Nil by mouth if toxic megacolon is suspected
If no response to IV steroids in 3-5 days - Rescue therapy:
- Infliximab (anti-TNF biologic) - 5 mg/kg IV
- OR Cyclosporin 2-4 mg/kg IV - effective in 82% of steroid-refractory UC cases
- Harrison's Principles of Internal Medicine 22E
If Toxic Megacolon or Perforation:
- Emergency surgical consultation
- Urgent colectomy
Critical Rule Before Starting Steroids:
- Exclude C. difficile (stool PCR result needed)
- Exclude amoeba (stool microscopy)
- Exclude CMV colitis if immunocompromised or steroid-refractory (tissue biopsy)
- Giving steroids to someone with active amoebiasis can be fatal
The Overall Picture
| Feature | Significance |
|---|---|
| 2 months bloody mucoid diarrhea | Chronic colitis - IBD most likely |
| Fever + chills | Systemic inflammation or bacteraemia |
| Dizziness on standing | Orthostatic hypotension - significant anaemia from chronic blood loss |
| Severe left colicky pain | Sigmoid/descending colon disease - consistent with UC |
| No clinical dehydration | Anaemia, not fluid loss, is the main problem |
Bottom Line
This person has probable severe ulcerative colitis (or less likely, another chronic colitis) with:
- Symptomatic anaemia (dizziness on standing)
- Systemic infection/inflammation (fever + chills)
- Active colonic disease (severe left-sided colicky pain)
This is a medical emergency. The patient needs to go to a hospital emergency department right now for IV fluids, bloods including haemoglobin, blood cultures, abdominal X-ray, and probable admission for IV steroids.
Do not attempt to manage this at home or wait for an outpatient appointment.
Disclaimer: This is clinical educational information. The symptoms described require immediate in-person medical evaluation and should not be managed based on this information alone.
Diet for ibs
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
"irritable bowel syndrome"[MeSH Terms] AND "diet"[MeSH Terms] AND "FODMAP"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive textbook content. Here is the full, well-sourced answer:
Diet for IBS (Irritable Bowel Syndrome)
Important note first: Before reading this, the symptoms we discussed earlier - 2 months of bloody mucoid diarrhea, fever, chills, left-sided pain, and dizziness on standing - are NOT consistent with IBS. IBS does not cause blood in stool, fever, or anaemia. Those symptoms require urgent medical investigation. This diet guide applies to confirmed IBS only.
IBS is a functional bowel disorder characterised by chronic or recurrent abdominal pain linked to changes in stool form or frequency, in the absence of structural or biochemical disease. Diet is a first-line treatment.
Why Diet Matters in IBS
"Meal-related symptoms are reported by about two thirds of patients and include abdominal pain, bloating, and flatulence, often triggered by larger meals, foods rich in carbohydrates or fats, coffee, alcohol, and spicy foods."
- Goldman-Cecil Medicine
Food interacts with gut motility, visceral sensitivity, gut microbiota, and mucosal permeability - all of which are dysregulated in IBS. Identifying and avoiding dietary triggers is central to management.
Step 1 - Food and Symptom Diary
Before changing anything, keep a 1-2 week diary recording:
- Everything eaten and drunk
- Timing and nature of symptoms
- Stool frequency and consistency (use the Bristol Stool Scale)
- Stress levels
This identifies personal triggers before any formal dietary intervention.
Step 2 - General Dietary Principles (All IBS Subtypes)
These apply regardless of whether your IBS is predominantly constipation, diarrhea, or mixed:
| Principle | Detail |
|---|---|
| Regular meal timing | Eat at consistent times; avoid skipping meals |
| Smaller portions | Large meals trigger the gastrocolic reflex and worsen symptoms |
| Eat slowly | Reduces air swallowing (bloating) |
| Adequate hydration | 6-8 glasses of water/day; avoid fizzy drinks |
| Limit caffeine | Coffee, tea, energy drinks - stimulate colonic motility |
| Limit alcohol | Worsens diarrhea and bloating |
| Limit fatty/fried food | Fat strongly stimulates gut contractions |
| Limit spicy food | Can exacerbate pain and urgency |
Step 3 - The Low-FODMAP Diet (Most Evidence-Based)
FODMAP stands for Fermentable Oligosaccharides, Disaccharides, Monosaccharides, And Polyols - short-chain carbohydrates that are poorly absorbed in the small intestine, then rapidly fermented by colonic bacteria, producing gas, bloating, pain, and altered stool.
"A diet that is low in FODMAPs can improve global IBS symptoms, especially in patients with predominant diarrhea, and also can reduce abdominal pain, abdominal bloating, and abnormal bowel habits. This diet is best explained and supervised by a trained dietitian."
- Goldman-Cecil Medicine
A 2025 network meta-analysis in the Lancet Gastroenterology & Hepatology confirmed the low-FODMAP diet as among the most effective dietary interventions for IBS symptom reduction.
The Low-FODMAP Protocol Has 3 Phases:
Phase 1 - Strict Elimination (4-6 weeks)
Remove all high-FODMAP foods completely.
Phase 2 - Reintroduction (6-8 weeks)
Systematically reintroduce one FODMAP group at a time to identify personal triggers. Not everyone reacts to all FODMAPs.
Phase 3 - Personalisation
Long-term diet based only on avoiding confirmed personal triggers - not permanent restriction of everything.
High-FODMAP Foods to AVOID (Phase 1):
| Category | FODMAP Type | Avoid |
|---|---|---|
| Fruits | Fructose/Polyols | Apples, pears, mangoes, watermelon, cherries, dried fruits |
| Vegetables | Fructans/Polyols | Onion, garlic, leek, cauliflower, mushrooms, asparagus |
| Legumes | Oligosaccharides | Chickpeas, lentils, kidney beans, baked beans |
| Dairy | Lactose | Cow's milk, soft cheeses, yogurt, ice cream |
| Wheat/Rye | Fructans | Bread, pasta, cereals, crackers (wheat-based) |
| Sweeteners | Polyols | Sorbitol, mannitol, xylitol (in "sugar-free" products) |
| Drinks | Multiple | Apple juice, pear juice, high-fructose corn syrup drinks |
Low-FODMAP Foods that are SAFE to eat:
| Food Group | Safe Choices |
|---|---|
| Fruits | Banana (ripe), blueberries, strawberries, grapes, oranges, kiwi, pineapple |
| Vegetables | Carrots, cucumber, bell peppers, tomatoes, spinach, potatoes, courgette (zucchini), green beans |
| Protein | Chicken, turkey, fish, eggs, tofu, firm tempeh |
| Grains | Rice, oats (rolled), quinoa, gluten-free bread/pasta, corn/polenta |
| Dairy alternatives | Lactose-free milk, almond milk, rice milk, hard cheeses (cheddar, parmesan), lactose-free yogurt |
| Nuts/seeds | Walnuts, peanuts, pecans, pumpkin seeds (small portions) |
| Fats/oils | Olive oil, butter (small amounts), coconut oil |
Step 4 - Fibre Considerations
Soluble fibre is beneficial - can normalise stool consistency in both diarrhea and constipation subtypes:
- Psyllium husk (Ispaghula) - 5-10 g/day, build up gradually
- Oats
- Bananas, carrots
Insoluble fibre (wheat bran) should be avoided or minimised - it can worsen bloating, gas, and abdominal pain in IBS.
"Guidelines specifically recommend soluble (e.g., psyllium) but not insoluble fiber (e.g., wheat bran). Fiber may cause abdominal discomfort and gas, so lower doses should be used initially."
- Goldman-Cecil Medicine
Step 5 - Subtype-Specific Adjustments
IBS-D (Diarrhea-Predominant):
- Strict low-FODMAP adherence most important
- Limit caffeine and alcohol strictly
- Avoid raw bran, high-fat meals
- Cooked, low-residue foods are better tolerated
- Probiotics (Lactobacillus, Bifidobacterium strains) may help
IBS-C (Constipation-Predominant):
- Increase soluble fibre gradually
- Ensure adequate fluid intake (dehydration worsens constipation)
- Prune juice (small amounts) or kiwi fruit can help
- Regular physical activity stimulates gut motility
IBS-M (Mixed):
- Start with general principles + low-FODMAP
- Identify specific triggers through food diary
- Adjust fibre based on predominant symptom at any given time
Other Dietary Considerations
| Approach | Evidence | Notes |
|---|---|---|
| Gluten-free diet | Modest benefit in some | May help if gluten consistently triggers symptoms; less evidence than low-FODMAP |
| Lactose-free | Helps if lactose intolerant | Worth trying if dairy consistently triggers symptoms |
| Probiotics | Moderate evidence | Bifidobacterium infantis 35624 and certain Lactobacillus strains reduce bloating and pain |
| Peppermint oil | Good evidence | Antispasmodic; reduces abdominal pain; take enteric-coated capsules |
What to Avoid Regardless of Subtype
- Chewing gum (contains polyols like sorbitol/xylitol)
- Carbonated drinks (gas and bloating)
- Skipping meals (disrupts gut motility rhythm)
- Eating very late at night
- Ultra-processed foods (additives, emulsifiers can worsen gut barrier function)
Practical Sample Day (Low-FODMAP, IBS-D)
| Meal | Example |
|---|---|
| Breakfast | Oat porridge with lactose-free milk + banana + a few blueberries |
| Snack | Rice cakes with peanut butter |
| Lunch | Grilled chicken with rice + steamed carrots and green beans + olive oil dressing |
| Snack | Hard-boiled egg + handful of walnuts |
| Dinner | Baked salmon with quinoa + roasted bell peppers + courgette |
| Drinks | Water, peppermint tea, lactose-free milk; avoid coffee, fizzy drinks, alcohol |
Key Takeaways
- Low-FODMAP diet is the most evidence-based dietary approach for IBS - works best under dietitian supervision
- Keep a food diary first to identify personal triggers
- Soluble fibre helps; insoluble bran worsens symptoms
- Low-FODMAP is a temporary elimination then reintroduction process - not a lifelong restrictive diet
- General habits (regular meals, smaller portions, slow eating, adequate water) matter alongside specific food choices
- Blood in stool, fever, weight loss, or anaemia are never IBS - always investigate these
Sources: Goldman-Cecil Medicine; Textbook of Family Medicine 9e; Lancet Gastroenterol Hepatol 2025 [PMID: 40258374]
Food diet for ulcerative colitis
Finding Sources
Finding Sources
Searching PubMed
"ulcerative colitis"[MeSH Terms] AND "diet"[MeSH Terms]
Finding Sources
Searching PubMed
"inflammatory bowel disease" AND diet AND nutrition
Reading Article
PMID: 38276922
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Searching PubMed
"ulcerative colitis" AND "dietary patterns" AND remission
Excellent - I have the 2024 AGA Clinical Practice Update (the most authoritative current guideline), an RCT on Mediterranean diet in UC, and Harrison's textbook content. Here is the comprehensive answer:
Diet for Ulcerative Colitis
Diet in UC is context-dependent - what you eat during an active flare is very different from what you eat during remission. No single diet cures UC, but the right nutrition plan reduces symptom burden, supports healing, prevents nutritional deficiencies, and may help reduce the frequency of flares.
The Central Principle
"A healthy Mediterranean diet will benefit patients with IBD. No diet has consistently been found to decrease the rate of flares in adults with IBD. A diet low in red and processed meat may reduce ulcerative colitis flares."
- AGA Clinical Practice Update on Diet in IBD, Gastroenterology 2024 (Hashash et al., PMID 38276922)
Phase 1 - During an Active Flare
When the bowel is actively inflamed and bleeding, the goal is to rest the gut, maintain nutrition, and avoid irritants without starving yourself.
General Principles During a Flare:
| Principle | Why |
|---|---|
| Low-residue / low-fibre diet | Reduces stool bulk and frequency; less mechanical irritation to inflamed mucosa |
| Small, frequent meals (5-6/day) | Easier on the inflamed colon than large meals |
| Soft, well-cooked foods | Easier to digest; less colonic stimulation |
| Adequate hydration | Replace fluid and electrolytes lost in diarrhea |
| High protein intake | Supports mucosal healing and counters protein loss from inflamed, leaking bowel |
| Avoid raw fruits and vegetables | High fibre and residue worsens diarrhea during flares |
Foods to EAT During a Flare:
Carbohydrates:
- White rice, white bread, plain crackers, rice cakes
- Plain pasta or noodles (white, not wholegrain)
- Boiled or mashed white potato (no skin)
- Oatmeal (plain, well-cooked)
- Cornflakes or rice-based cereals
Protein:
- Chicken (boiled, baked, without skin)
- Fish (steamed or baked - salmon, white fish)
- Eggs (boiled, poached, scrambled - not fried)
- Tofu
- Well-cooked lentils (small amounts if tolerated)
Vegetables (cooked only, no skin, no seeds):
- Well-boiled carrots, courgette (zucchini), butternut squash
- Peeled cucumber
- Mashed sweet potato (peeled)
- Avoid: broccoli, cauliflower, cabbage, onion, peppers (raw), corn
Fruits (peeled, cooked, or tinned in juice):
- Banana (ripe)
- Tinned peaches, pears (in juice, not syrup)
- Cooked apple (peeled, no skin)
- Avoid: high-fibre fruits (apples with skin, pears, berries, dried fruit)
Dairy:
- If lactose-tolerant: natural yogurt (small amounts), hard cheese
- If lactose causes symptoms: use lactose-free milk, lactose-free yogurt, or plant-based alternatives
- Note: lactose intolerance is common during flares even if normally tolerated - temporarily limit dairy
Fluids:
- Water (sip regularly throughout the day)
- Oral rehydration solutions (ORS) if significant diarrhea
- Diluted fruit juice (not apple or pear - high fructose)
- Weak tea (no milk if lactose avoiding)
- Avoid: fizzy drinks, alcohol, caffeine, full-strength fruit juices
Foods to AVOID During a Flare:
| Category | Specific Foods |
|---|---|
| High fibre | Brown rice, wholegrain bread, bran cereals, raw vegetables, legumes |
| Spicy foods | Chilli, hot sauce, curry (high spice) |
| Fatty/fried foods | Fast food, deep-fried anything, fatty meats |
| Dairy (if intolerant) | Full-fat milk, soft cheeses, ice cream |
| Alcohol | Beer, wine, spirits |
| Caffeine | Coffee, strong tea, energy drinks |
| Red/processed meat | Beef, pork sausages, bacon, deli meats |
| Ultra-processed foods | Ready meals, packaged snacks, artificial additives |
| Seeds and nuts | Can mechanically irritate inflamed mucosa |
| Fizzy drinks | Bloating and gas |
Phase 2 - During Remission (When Symptoms Are Controlled)
When UC is in remission, the goals shift to maintaining remission, eating for overall health, correcting nutritional deficiencies, and supporting the gut microbiome.
The Mediterranean Diet - First-Line Recommendation
The 2024 AGA Clinical Practice Update recommends the Mediterranean diet as the primary dietary pattern for all IBD patients in remission. A 2023 RCT published in the Journal of Crohn's and Colitis showed that a Mediterranean diet pattern improved intestinal inflammation and beneficially reshaped the gut microbiome in UC patients.
The Mediterranean Diet Includes:
| Food Group | Frequency | Examples |
|---|---|---|
| Vegetables | Every meal | Tomatoes, leafy greens, peppers, aubergine, courgette |
| Fruits | 2-3 portions/day | Berries, citrus, apples, grapes, figs |
| Whole grains | Daily | Wholegrains, brown rice, oats (if tolerated) |
| Legumes | 3-4x/week | Lentils, chickpeas, beans (introduce slowly) |
| Fish/seafood | 2-3x/week | Salmon, sardines, mackerel (rich in omega-3) |
| Olive oil | Primary fat | Extra virgin; anti-inflammatory properties |
| Nuts and seeds | Daily (small amounts) | Walnuts, almonds, flaxseed (well-chewed) |
| Lean poultry | Moderate | Chicken, turkey |
| Dairy | Moderate | Yogurt (probiotic), hard cheese |
| Red meat | Rare (≤1-2x/week) | Small portions; avoid processed meats |
| Alcohol | Minimal/none | Red wine only in moderation if at all |
Foods with Evidence of Reducing UC Flares:
- Omega-3 fatty acids (oily fish: salmon, mackerel, sardines, herring) - anti-inflammatory effect on colonic mucosa
- Fermented foods (natural yogurt, kefir, miso) - support gut microbiome
- Soluble fibre (oats, psyllium, cooked vegetables) - feeds beneficial gut bacteria, produces butyrate which nourishes colonocytes
- Curcumin (turmeric) - some evidence as adjunct to maintain remission in mild-moderate UC; anti-inflammatory
Foods Linked to Increasing UC Flares - LIMIT OR AVOID:
- Red meat and processed meats (bacon, sausages, hot dogs) - AGA advises a diet low in red and processed meat to reduce UC flares
- Ultra-processed foods - emulsifiers (carrageenan, polysorbate-80) disrupt mucosal barrier and alter microbiome
- Refined sugars and sweetened beverages
- High-fat Western diet foods
- Alcohol - directly irritates mucosa and can trigger flares
- NSAIDs (ibuprofen, naproxen) - not food, but a common trigger for UC flares; always tell your doctor before taking
Nutritional Deficiencies Common in UC - Monitor and Supplement
Active UC depletes several key nutrients through bleeding, diarrhea, malabsorption, and medication effects:
| Nutrient | Reason Deficient | Signs | Source/Supplement |
|---|---|---|---|
| Iron | Chronic rectal bleeding | Fatigue, pallor, dizziness | Red meat (remission), leafy greens, IV iron if severe |
| Folate | Sulfasalazine blocks absorption | Anaemia, neural tube risk | Green vegetables, folate supplement (1 mg/day) |
| Vitamin D | Reduced absorption, steroid use | Bone pain, low immunity | Sunlight, oily fish, supplement (800-2000 IU/day) |
| Calcium | Steroid use, low dairy intake | Bone loss (osteoporosis risk) | Dairy, fortified foods, calcium supplements if on steroids |
| Vitamin B12 | If terminal ileum affected | Fatigue, neurological symptoms | Meat, eggs, dairy; supplement if low |
| Zinc | Lost in diarrhea | Poor wound healing, low immunity | Meat, nuts, seeds, supplement if deficient |
| Magnesium | Lost in diarrhea | Muscle cramps, fatigue | Nuts, seeds, leafy greens |
All UC patients on steroids should take Vitamin D + Calcium supplementation to prevent steroid-induced osteoporosis.
Practical Sample Day (UC in Remission - Mediterranean Style)
| Meal | Example |
|---|---|
| Breakfast | Porridge (oats) with lactose-free milk, sliced banana, a drizzle of honey; herbal tea |
| Mid-morning | Natural yogurt with blueberries |
| Lunch | Grilled salmon with brown rice, steamed courgette and carrots; olive oil dressing |
| Afternoon snack | Small handful of walnuts + an orange |
| Dinner | Chicken or lentil soup with soft-cooked vegetables; gluten-free or white bread if grains are an issue |
| Evening | Kefir (probiotic) or warm lactose-free milk |
| Throughout day | 1.5-2 litres of water; peppermint or chamomile tea |
Practical Sample Day (UC During Active Flare)
| Meal | Example |
|---|---|
| Breakfast | Plain white rice porridge with a mashed banana; weak tea |
| Mid-morning | Oral rehydration drink; plain rice cake |
| Lunch | Boiled chicken with white rice and well-cooked mashed carrot |
| Afternoon | Ripe banana + lactose-free yogurt (small portion) |
| Dinner | Steamed white fish with mashed potato (peeled) and boiled courgette |
| Evening | Warm water or diluted juice (not apple/pear) |
Key Rules to Remember
- Diet does not replace medication - mesalamine, steroids, and biologics treat the disease; diet supports recovery and overall health
- Flare phase = low residue, soft, easy-to-digest foods - rest the colon
- Remission phase = Mediterranean diet - variety of plant foods, oily fish, olive oil, limit processed and red meat
- Always correct nutritional deficiencies - especially iron (from chronic bleeding), folate (if on sulfasalazine), and vitamin D/calcium (if on steroids)
- Keep a food and symptom diary - UC triggers are personal; identify your own
- Work with a registered dietitian - especially for ongoing management; the AGA specifically recommends this
- Avoid alcohol, NSAIDs, and ultra-processed foods consistently - these are known flare triggers
Sources: AGA Clinical Practice Update on Diet and Nutritional Therapies in IBD, Gastroenterology 2024 (PMID 38276922); Mediterranean diet RCT in UC (PMID 37095601); Harrison's Principles of Internal Medicine 22E
Disclaimer: This dietary guide is for educational purposes. Nutritional management of UC should be individualised with the help of a gastroenterologist and registered dietitian.
This is a shared conversation. Sign in to Orris to start your own chat.