analyse_media
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
CT Brain Analysis - Polaris Neuroscience Hospital, Agra
This is a non-contrast CT (NCCT) of the brain taken at Polaris Neuroscience Hospital, Agra. The scan includes axial slices from the posterior fossa through the vertex.
Key Findings
1. Acute Left Basal Ganglia / Putaminal Hemorrhage
The dominant finding is a large, hyperdense (bright white) intraparenchymal hematoma in the region of the left putamen and adjacent internal capsule. This is the most common location for hypertensive intracerebral hemorrhage. The clot is irregular, and a surrounding hypodense rim indicates acute vasogenic edema.
2. Intraventricular Extension (IVH)
Hyperdense blood is seen tracking into the posterior horn of the left lateral ventricle and the third ventricle, indicating intraventricular extension - a marker of severity and poor prognosis.
3. Mass Effect and Midline Shift
- Rightward midline shift of the septum pellucidum and adjacent structures
- Compression and effacement of the left lateral ventricle
- Sulcal effacement over the left hemisphere
- The right lateral ventricle is mildly dilated due to outflow obstruction at the foramen of Monro
4. Early Obstructive Hydrocephalus
Asymmetric ventricular enlargement (right > left) consistent with early non-communicating hydrocephalus from blood in the ventricular system.
5. No other lesions
No independent mass lesion, abscess, or large territorial infarction identified.
Diagnosis
Acute left putaminal / basal ganglia intracerebral hemorrhage (ICH) with intraventricular extension, significant mass effect, rightward midline shift, and early obstructive hydrocephalus.
The pattern - deep location in basal ganglia/putamen, no signs of underlying tumor or vascular malformation - is classic for hypertensive hemorrhage, the most common cause of spontaneous ICH, accounting for 72-81% of cases.
Clinical Correlation
As described in Adams and Victor's Principles of Neurology, 12th Ed.:
"The most common hypertensive hemorrhage syndrome is the one caused by putaminal hemorrhage with extension to the adjacent internal capsule. Hemiplegia from transection of the internal capsule is a consistent feature of medium-sized and large clots... With large hemorrhages, patients lapse almost immediately into a stupor with hemiplegia and their condition visibly deteriorates as the hours pass."
Expected clinical findings with a hemorrhage of this size and location:
- Contralateral hemiplegia/hemiparesis (right-sided weakness, right facial droop)
- Dysarthria or aphasia (left hemisphere dominant in most patients)
- Headache, vomiting
- Depressed consciousness / coma (large clot + IVH)
- Gaze deviation to the LEFT (away from paretic limbs)
- Possible Babinski signs bilaterally
Management Priorities (from Bradley and Daroff's Neurology in Clinical Practice)
| Priority | Action |
|---|---|
| Airway | Intubation if GCS ≤8 (use fentanyl 2-3 mcg/kg to blunt ICP rise) |
| Blood pressure | IV antihypertensive if BP >180/105 mmHg; target SBP ~140-160 mmHg |
| ICP management | Head elevation 30°, osmotherapy (mannitol or hypertonic saline) |
| Coagulopathy reversal | Check INR, platelets, DOAC use; reverse if abnormal |
| Surgical consult | Neurosurgery for possible hematoma evacuation or EVD for hydrocephalus |
| Glucose | Control hyperglycemia (associated with hematoma expansion) |
| Seizure prophylaxis | Monitor; treat clinically evident seizures |
Surgical considerations: IVH with early hydrocephalus may warrant external ventricular drain (EVD) insertion. Surgical evacuation for a deep basal ganglia hemorrhage remains controversial but should be discussed with neurosurgery.
Reference Comparison (Textbook)
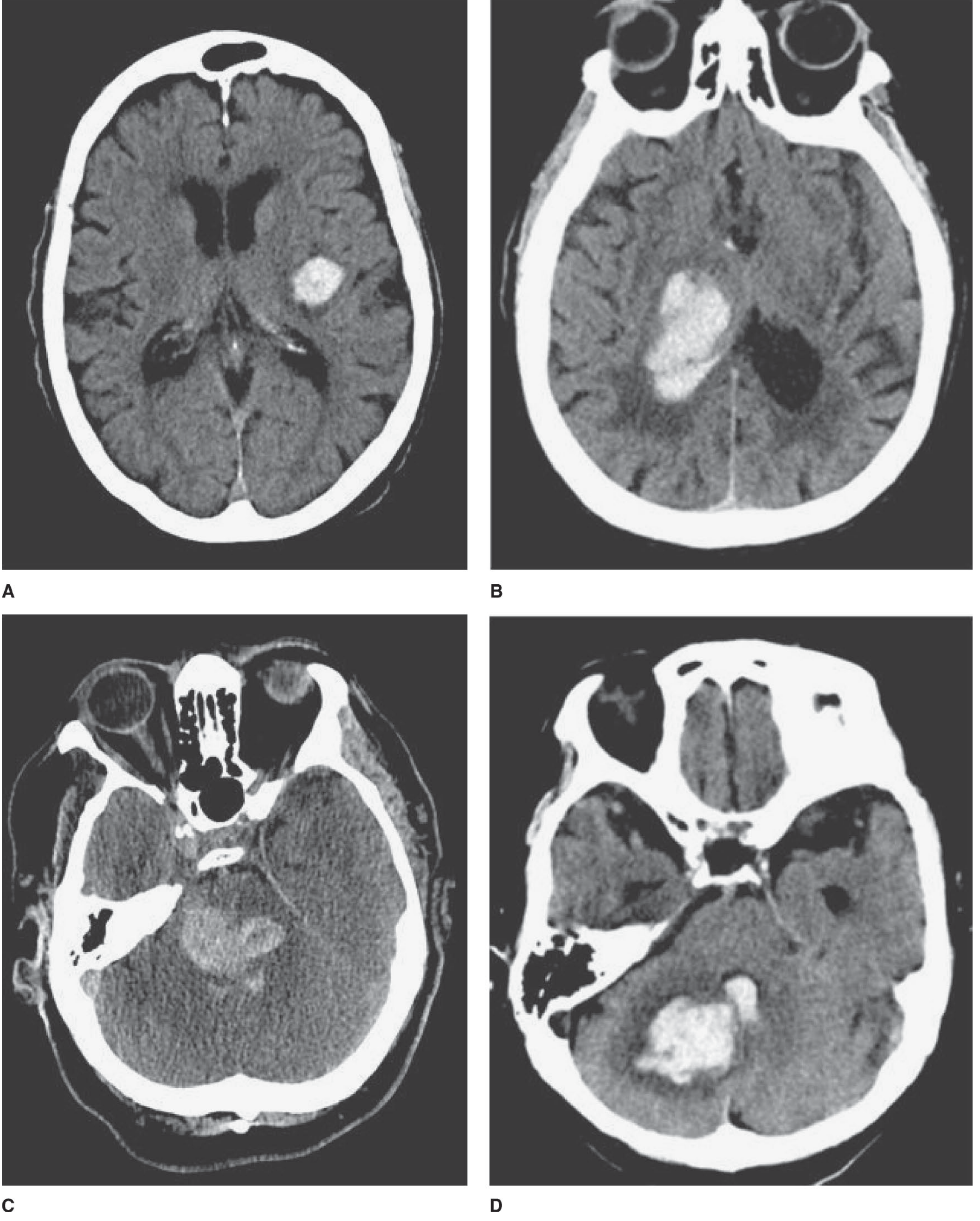
The image below from Adams and Victor's Principles of Neurology shows classic hypertensive hemorrhages at the same locations - note the left putaminal hematoma (panel A) as the closest comparator to this patient's scan:
Clinical Disclaimer: This analysis is for educational/informational purposes. Clinical decisions must be made by qualified physicians with full access to the patient's history, examination, and complete imaging data.
This is a shared conversation. Sign in to Orris to start your own chat.