Detailed note on mammary gland with diagram
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compose the detailed note.
Mammary Gland - Detailed Notes
1. Introduction
The mammary gland is a modified sweat gland (apocrine type) that lies within the subcutaneous tissue (superficial fascia) of the anterior chest wall. It is a branched tubuloalveolar exocrine gland that develops from the epidermis and serves as the organ of milk production. Although present in both sexes, it reaches full functional development only in females after pregnancy.
2. Position and Surface Anatomy
- Situated between the skin and the superficial pectoral fascia, overlying the pectoralis major muscle
- Extends vertically from rib II to rib VI
- Lies between the lateral border of the sternum and the midaxillary line
- The superolateral region extends along the inferior border of pectoralis major toward the axilla as the axillary tail (axillary process of Spence) - this may penetrate the deep fascia to enter the axilla proper
- The nipple and surrounding areola occupy a variable position depending on breast size
3. Gross Structure and Layers
From superficial to deep:
| Layer | Content |
|---|---|
| Skin (epidermis + dermis) | Contains lymphatics |
| Subcutaneous fat | Subcutaneous adipose tissue |
| Glandular parenchyma | Lobes, ducts, TDLUs |
| Retromammary fat | Separates breast from pectoral fascia |
| Deep fascia | Overlies pectoralis major |
| Pectoralis major muscle | Posterior support |
Diagram: Cutaway of a Mature Resting Breast
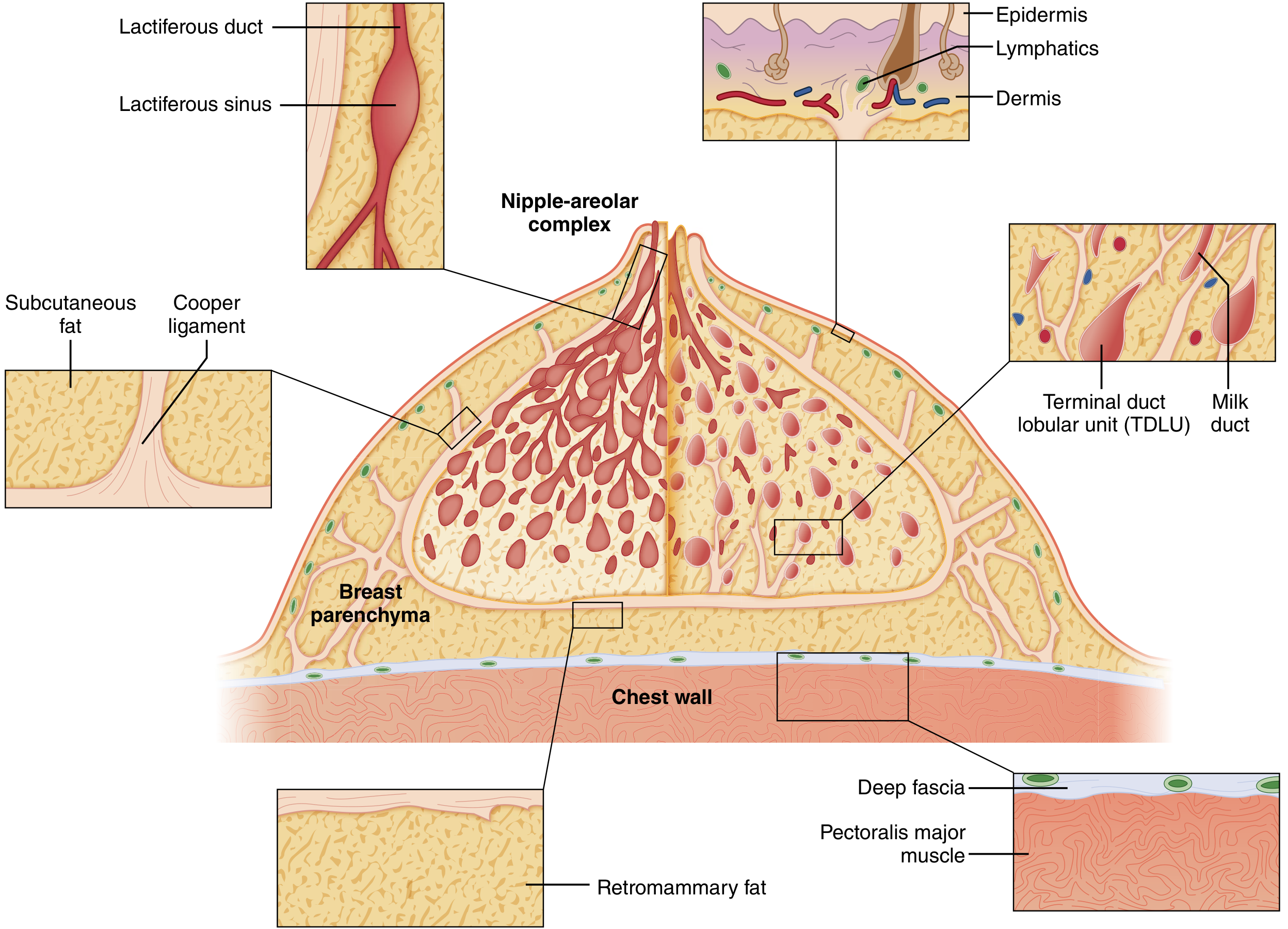
Cutaway diagram showing the major structural components of the breast. The duct system is arranged like an inverted tree, converging at the nipple. TDLUs are the functional milk-forming units at the periphery. Cooper ligaments run from the chest wall to the dermis giving the breast its shape. (Sabiston Textbook of Surgery, Fig. 68.1)
4. Structural Components (Parenchyma)
The mature breast is composed of three principal tissue types:
- Glandular epithelium - the ductal and lobular system
- Fibrous stroma - Cooper's ligaments and intralobular/interlobular connective tissue
- Adipose tissue - predominates after menopause
4a. Lobes and Ducts
- The glandular apparatus consists of 15 to 20 lobes, arranged radially around the nipple-areolar complex (NAC)
- Each lobe drains via a single lactiferous duct that opens at the nipple
- Just below the NAC, each lactiferous duct has a dilated segment = lactiferous sinus (ampulla)
- From the sinus, ducts branch progressively into smaller ducts and ultimately end at the terminal ductules or acini
4b. Terminal Duct Lobular Unit (TDLU)
The TDLU is the functional unit of the breast:
- Consists of the terminal intralobular duct + its surrounding cluster of acini (alveoli)
- Invested in specialized loose intralobular stroma containing capillaries, lymphocytes, and plasma cells
- Distinguished from the denser, less cellular interlobular stroma and surrounding adipose tissue
- Most breast diseases (both benign and malignant) originate in TDLUs
Diagram: TDLU Histology
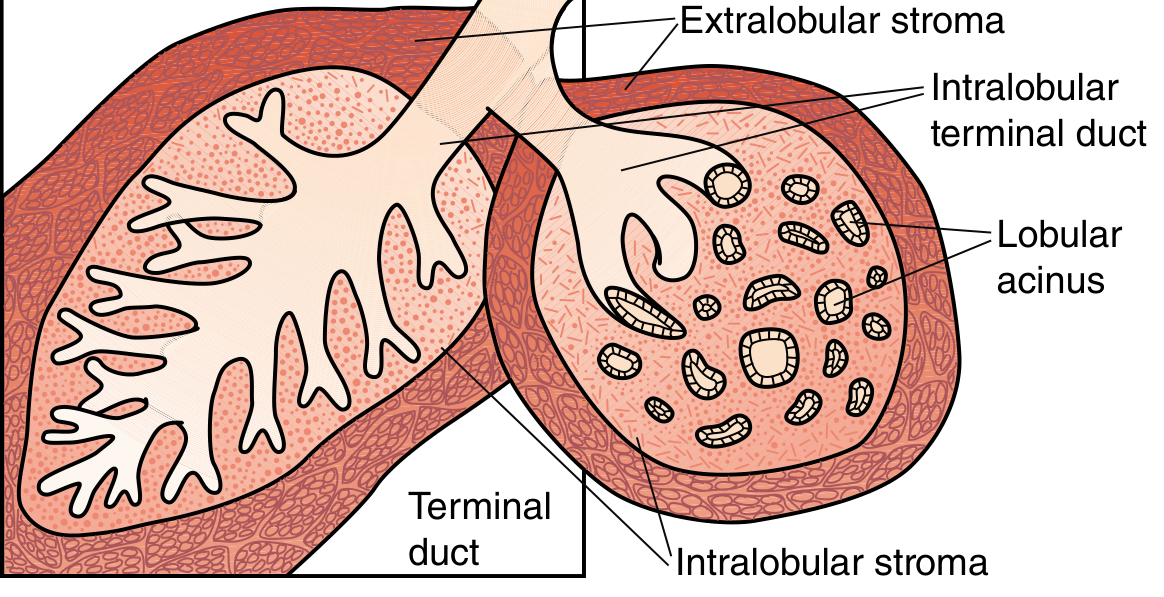
Schematic of two TDLUs. Left: inactive lobule with ductal components. Right: active lobule showing intralobular terminal duct, lobular acini, and the contrasting intralobular (loose) vs extralobular (dense) stroma. (Sabiston Textbook of Surgery, Fig. 68.2)
4c. Cooper's Ligaments (Suspensory Ligaments)
- Multiple fibrous bands that run from the chest wall to the dermis
- Provide structural support and shape to the breast
- When infiltrated by carcinoma or when edema is present, they shorten and pucker the overlying skin - producing peau d'orange (skin of orange) or skin dimpling
5. Histology
Inactive (Resting) Stage
- Parenchyma is sparse, consisting mainly of duct elements
- Ducts are surrounded by loose intralobular connective tissue containing lymphocytes, plasma cells, and fibroblasts
- Dense interlobular connective tissue contains adipocytes
- Ductal epithelium is cuboidal; myoepithelial cells are present at the base of epithelial cells
H&E section of inactive human mammary gland (x200). Ducts (D) are surrounded by loose connective tissue (CT/L) within lobules. Dense connective tissue (CT/D) with adipocytes (A) forms the interlobular framework. Lymphocytes (L) and plasma cells (P) populate the loose stroma. (Histology: A Text and Atlas, Plate 23.11)
Lactating Stage
- Ducts branch extensively; alveoli develop prominently from ductal ends
- Alveolar epithelium and intralobular ductal epithelium are single-layered cuboidal secretory cells
- Myoepithelial cells proliferate and lie between the base of epithelial cells and the basal lamina - they are most prominent in larger ducts
- Lobules are separated by narrow dense connective tissue septa
- Two secretory mechanisms operate simultaneously:
- Merocrine (exocytosis) - for protein component (lactalbumin, casein synthesized in ER, sorted through Golgi)
- Apocrine - for lipid component (fat droplets coalesce, bulge apically, are enveloped in plasma membrane as they are released)
6. Blood Supply
Arterial supply:
- Internal thoracic (mammary) artery - perforating branches through 2nd, 3rd, and 4th intercostal spaces supply the medial and central breast (largest contributor, ~60%)
- Lateral thoracic artery (branch of axillary artery) - supplies the lateral and upper breast
- Thoracoacromial artery (pectoral branch) - supplies upper breast
- Posterior intercostal arteries - smaller contribution to the lateral breast
Venous drainage:
- Correspond to the arteries: internal thoracic veins, axillary veins, and intercostal veins
- Communicates with vertebral venous plexus of Batson - a route for haematogenous spread of breast cancer to the spine
7. Lymphatic Drainage
Lymphatic drainage is clinically critical for breast cancer staging.
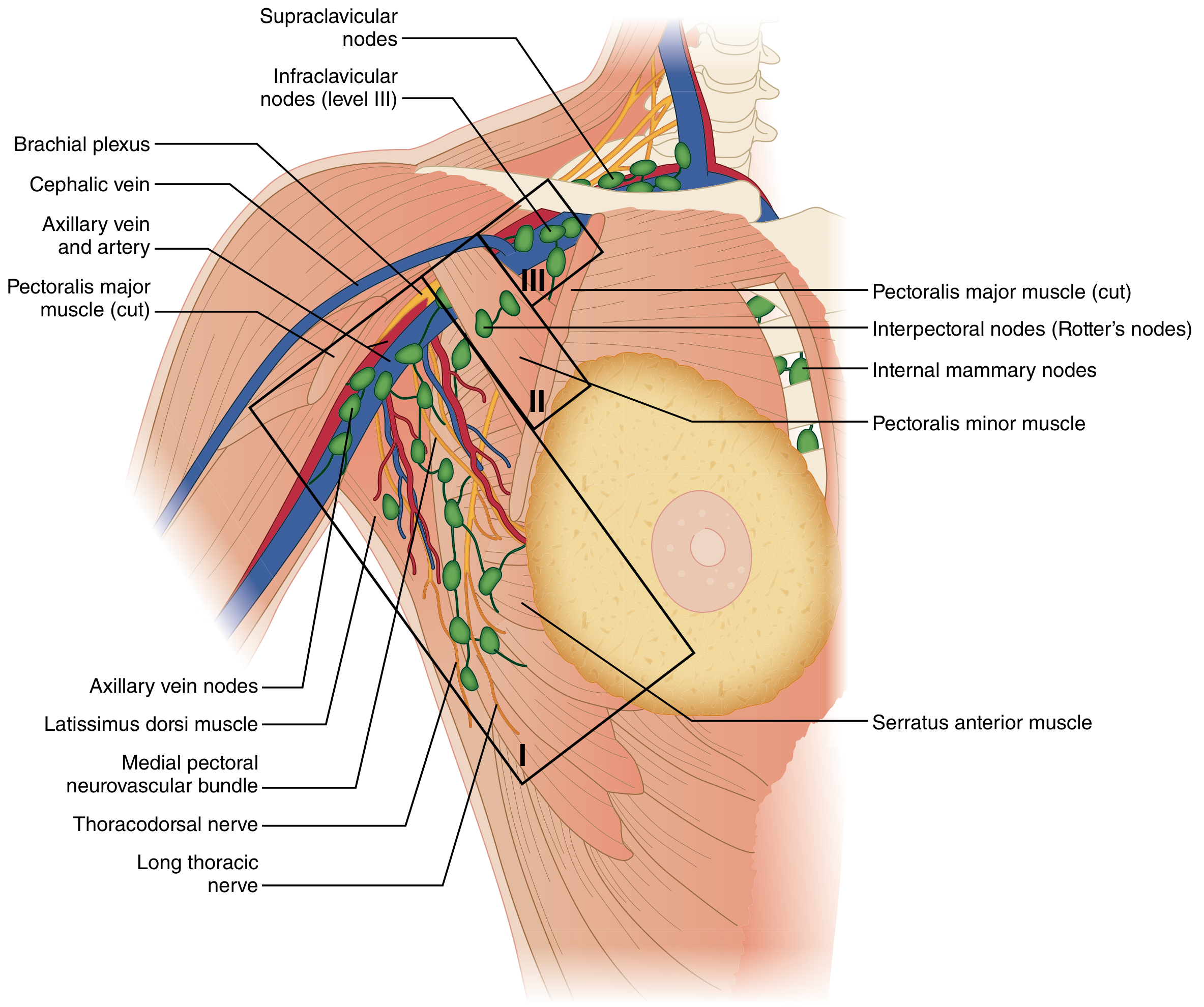
Lymphatic drainage of the breast. Axillary nodes are classified by their relationship to pectoralis minor: Level I (lateral), Level II (posterior), Level III (medial/infraclavicular). Internal mammary nodes drain the medial breast. The sentinel node is usually found in the external mammary (Level I) group. (Sabiston Textbook of Surgery, Fig. 68.4)
Axillary Nodes (principal drainage, ~75% of lymph)
Classified by relationship to pectoralis minor muscle:
| Level | Location | Nodes |
|---|---|---|
| Level I | Lateral to pectoralis minor | Anterior (pectoral), posterior (subscapular), lateral (axillary vein) nodes |
| Level II | Posterior to pectoralis minor | Central nodes + Interpectoral (Rotter's) nodes between pectoralis major and minor |
| Level III | Medial to pectoralis minor | Infraclavicular (apical) nodes |
The sentinel lymph node is functionally the first node in the drainage chain, anatomically usually found in the external mammary/Level I group.
Internal Mammary Nodes (parasternal)
- Drain the medial breast (particularly inner quadrants)
- Lie along the internal thoracic artery, inside the chest wall
- Important second pathway for metastasis
Supraclavicular Nodes
- Level III nodes are continuous with supraclavicular nodes above the clavicle
- Involvement classifies as N3 disease (Stage IIIC)
8. Nerve Supply
- Lateral cutaneous branches of the 2nd to 6th intercostal nerves - supply the lateral breast
- Anterior cutaneous branches of the 2nd to 6th intercostal nerves - supply the medial breast
- The nipple is predominantly supplied by the 4th intercostal nerve (T4 dermatome)
- Sympathetic fibers supply the smooth muscle of the nipple and blood vessels
9. Development
Embryological Development
- Breast develops from the ectoderm as a thickening called the milk bud in the pectoral region
- A bilateral mammary ridge (milk streak/milk line) extends from axilla to inguinal area at ~5 weeks
- By 9 weeks of gestation, the milk streak atrophies except at the pectoral region, forming a single pair of glands
- Failure of normal atrophy leads to polymastia (accessory breast tissue) or polythelia (accessory nipples), located along the milk line from axilla to pubis
- Accessory breast tissue most commonly appears in the axilla and may enlarge during pregnancy
Developmental Anomalies
| Anomaly | Description |
|---|---|
| Polymastia | Accessory breast glands along milk line |
| Polythelia | Accessory nipples along milk line |
| Amastia | Congenital absence of breast tissue |
| Athelia | Absence of nipple |
| Poland Syndrome | Unilateral absence of breast + pectoralis major/minor + serratus anterior + ribs |
Pubertal Development (Tanner Stages)
- Breast development begins at age 9-12 years in females (thelarche), typically the first sign of puberty
- Menarche follows at approximately 11-14 years
- Driven by rising estrogen from maturing ovaries: stimulates ductal growth
- Progesterone stimulates lobuloalveolar development
- Also requires: GH (via IGF-1), cortisol, prolactin
10. Hormonal Regulation and Physiology
Menstrual Cycle Effects
| Phase | Hormone | Effect on Breast |
|---|---|---|
| Follicular phase | Estrogen | Proliferation of lactiferous duct components |
| Luteal phase | Progesterone | Growth of alveoli; intralobular stroma becomes edematous; breast tenderness and mass increase |
Pregnancy Changes
- Corpus luteum then placenta produce continuous estrogen and progesterone → massive increase in TDLUs
- Lymphocytes and plasma cells infiltrate loose connective tissue
- Alveoli develop from ductal ends; most prominent in later pregnancy
- Myoepithelial cells proliferate at the alveolar and ductal base
- Prolactin (from anterior pituitary), hCS/hPL (from placenta), cortisol, and insulin all promote growth
Hormones affecting the mammary gland
| Category | Hormones |
|---|---|
| Mammogenic (ductal growth) | Estrogen, GH, cortisol, relaxin |
| Mammogenic (lobuloalveolar growth) | Estrogen, GH, cortisol, prolactin |
| Lactogenic (initiate milk production) | Prolactin, hCS, cortisol, insulin, thyroid hormones; withdrawal of estrogens and progesterone |
| Galactokinetic (milk ejection) | Oxytocin (principal), vasopressin (weak) |
(Medical Physiology, Table 56-6)
Lactation
- Initiation of lactation: During pregnancy, high estrogen and progesterone inhibit the effect of prolactin. After delivery, estrogen and progesterone fall sharply → prolactin acts on alveolar cells to initiate milk synthesis
- Milk ejection reflex: Suckling → sensory impulses → hypothalamus → posterior pituitary releases oxytocin → myoepithelial cells contract → milk is ejected from ducts
- Composition of milk: Fat emulsion in aqueous solution containing lactose, lactalbumin, casein, K+, Ca2+, Na+, Cl-, phosphate
- Colostrum: Secreted in first few days postpartum; alkaline, yellowish, higher in protein, vitamin A, Na+, Cl-; lower in fat and carbohydrates; rich in secretory IgA antibodies (from plasma cells in stroma, transcytosed across glandular cells) - provides passive immunity to the neonate
Involution
- After cessation of lactation, alveoli regress and TDLUs return to resting state
- After menopause, glandular structures involute and are replaced largely by adipose tissue
11. Clinical Correlations
| Finding | Mechanism |
|---|---|
| Peau d'orange (orange peel skin) | Inflammatory breast cancer infiltrates Cooper's ligaments and dermal lymphatics → skin dimpling and thickened skin |
| Skin dimpling | Carcinoma invades and shortens Cooper's ligaments |
| Nipple inversion | Central duct carcinoma or periductal fibrosis tethers the nipple |
| Witches' milk | 90% of newborns secrete breast fluid due to high maternal/placental hormones; resolves in 3-4 weeks |
| Paget's disease of breast | Malignant ductal cells invade epidermis of nipple → eczematous nipple change |
| Sentinel node biopsy | First draining axillary node (usually Level I); negative = no further node dissection needed |
| Batson's plexus | Valveless vertebral venous plexus communicating with mammary veins → hematogenous metastasis to spine/skull without lung involvement |
12. Summary - Key Points
- The mammary gland is a modified apocrine sweat gland, situated in the superficial fascia over pectoralis major (ribs II-VI)
- Structurally composed of 15-20 lobes, each draining via a lactiferous duct at the nipple; functional unit is the TDLU
- Cooper's ligaments connect chest wall to dermis - their infiltration by cancer causes peau d'orange
- Blood supply: mainly internal thoracic artery (medial/central) and lateral thoracic artery (lateral)
- Lymphatic drainage: primarily axillary (Levels I-II-III) with medial drainage to internal mammary nodes; sentinel node is the first in chain
- Hormonal control: estrogen (ductal), progesterone (lobuloalveolar), prolactin (lactogenesis), oxytocin (milk ejection)
- Colostrum contains secretory IgA providing passive neonatal immunity; true milk follows after progesterone/estrogen withdrawal
Sources:
- Sabiston Textbook of Surgery, Chapter 68 (Breast Anatomy, Development & Physiology)
- Gray's Anatomy for Students (Surface anatomy and axillary process)
- Histology: A Text and Atlas with Correlated Cell and Molecular Biology, Chapter 23 (Plates 23.11-23.12)
- Medical Physiology (Boron & Boulpaep), Chapter 56 (Lactation physiology)
This is a shared conversation. Sign in to Orris to start your own chat.