Fever differential diagnosis approach flowchart
Fever: Differential Diagnosis Approach
Definition
Step 1 - Initial Triage: Stable vs. Unstable
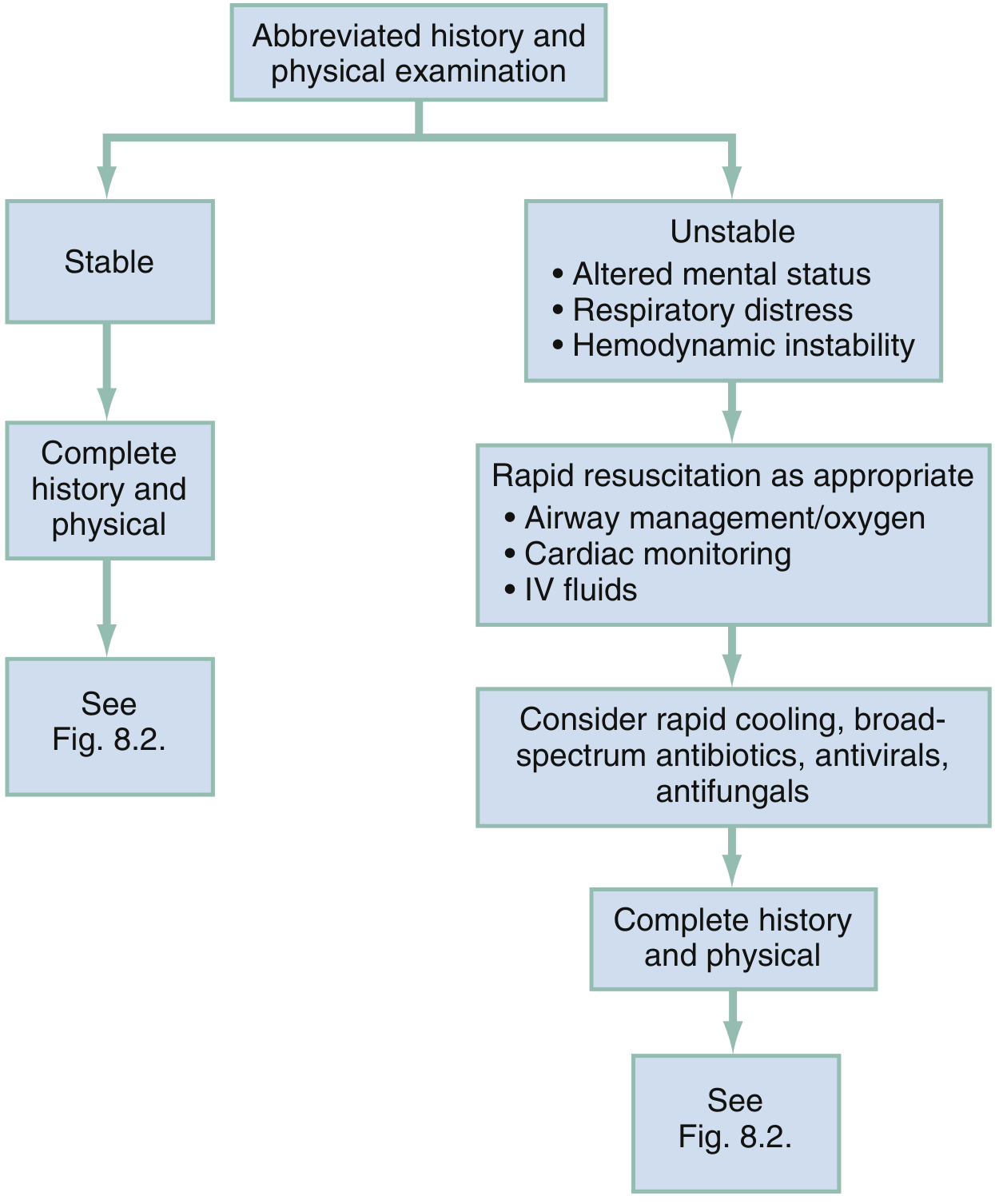
- Altered mental status
- Respiratory distress
- Hemodynamic instability (tachycardia, hypotension)
Step 2 - Approach to the Stable Febrile Patient
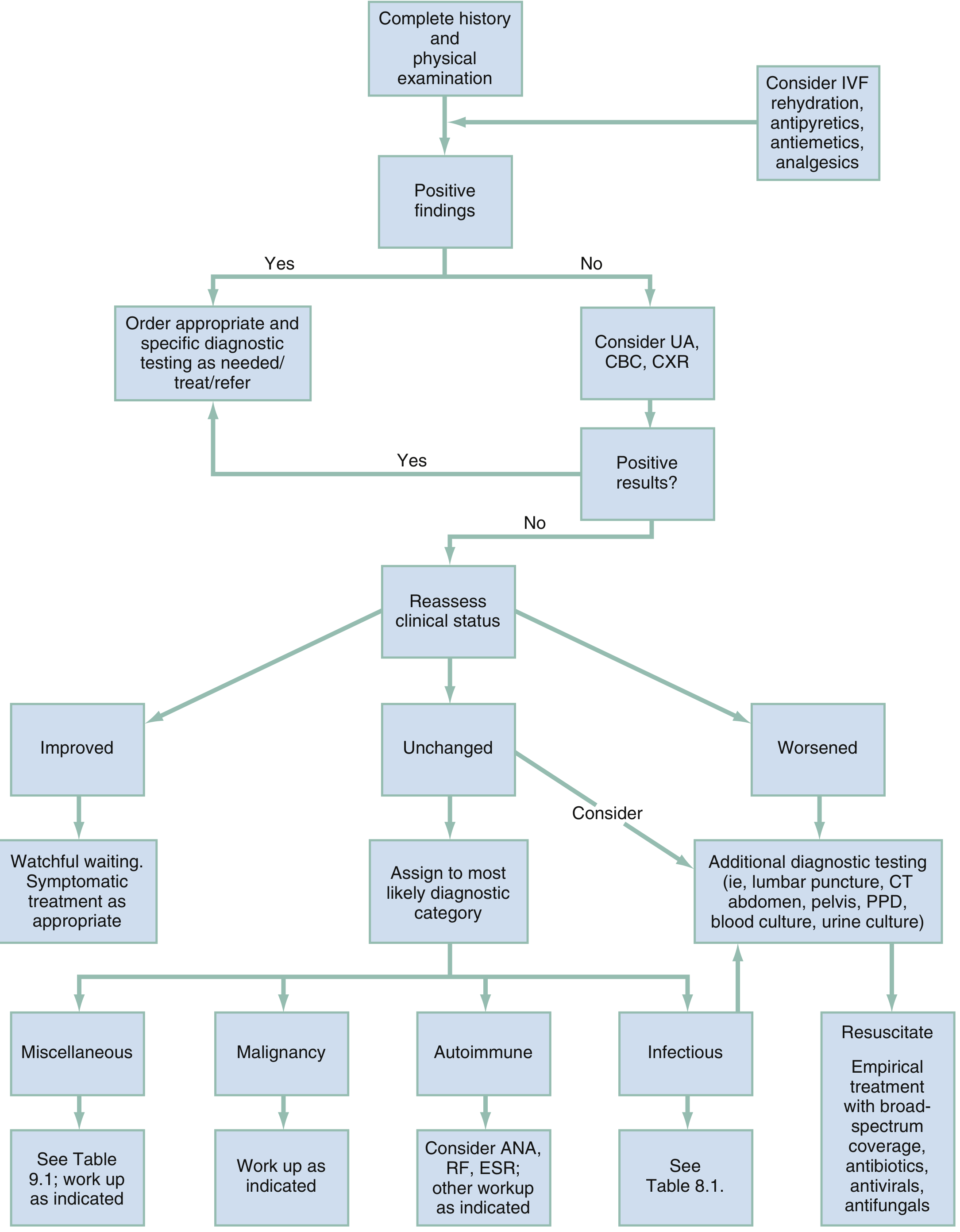
- Positive localizing findings on H&P - Order targeted diagnostic tests; treat/refer accordingly.
- No localizing findings - Screen with UA, CBC, CXR.
- Positive results - targeted workup/treatment.
- Negative results - reassess clinical status:
- Improved - Watchful waiting, symptomatic care.
- Unchanged - Assign to most likely diagnostic category (Infectious / Autoimmune / Malignancy / Miscellaneous). Consider ANA, RF, ESR for autoimmune; blood/urine cultures; CT for occult infection.
- Worsened - Additional diagnostics (LP, CT abdomen/pelvis, blood cultures) + empirical broad-spectrum coverage.
Step 3 - Differential Diagnosis Categories
A. Infectious Causes (most common treatable causes)
| Organ System | Critical | Emergent | Nonemergent |
|---|---|---|---|
| Respiratory | Bacterial pneumonia with respiratory failure | Pneumonia, peritonsillar abscess, epiglottitis | Otitis media, sinusitis, pharyngitis, bronchitis, influenza, TB, COVID-19 |
| Cardiovascular | - | Endocarditis, pericarditis | - |
| GI | Peritonitis | Appendicitis, cholecystitis, diverticulitis, intra-abdominal abscess | Colitis, enteritis |
| GU | - | Pyelonephritis, tubo-ovarian abscess, PID | Cystitis, epididymitis, prostatitis |
| Neurologic | Meningitis, cavernous sinus thrombosis | Encephalitis, brain abscess | - |
| Skin/Soft tissue | - | Cellulitis, infected decubitus ulcer, soft tissue abscess | - |
| Systemic | Sepsis/septic shock, meningococcemia | Influenza, COVID-19 | - |
B. Noninfectious Causes (Box 8.1 - Rosen's EM)
- Acute MI, pulmonary embolism/infarction
- Intracranial hemorrhage, CVA
- Neuroleptic malignant syndrome
- Thyroid storm, acute adrenal insufficiency
- Transfusion reaction, pulmonary edema
- CHF, dehydration, recent seizure
- Sickle cell disease, transplant rejection, pancreatitis, DVT
- Drug fever, malignancy, gout, sarcoidosis, Crohn disease
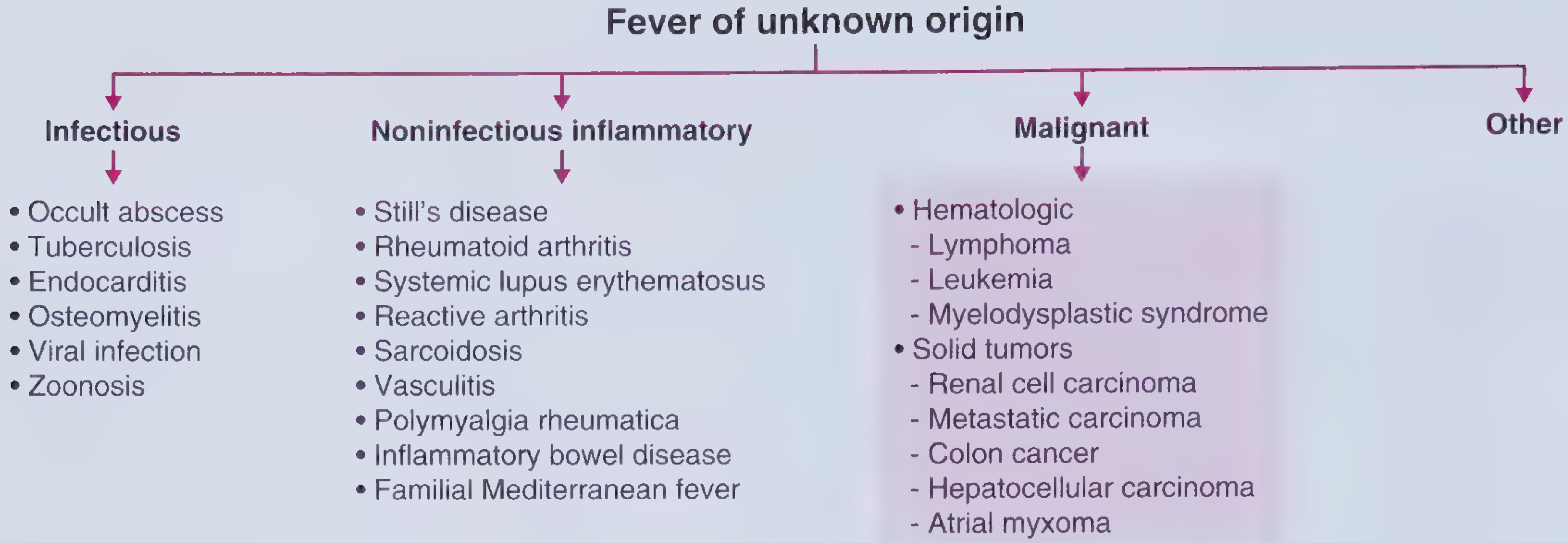
Step 4 - Fever of Unknown Origin (FUO)
| Category | Examples |
|---|---|
| Infectious | Occult abscess, TB (especially miliary), endocarditis (culture-negative), osteomyelitis, viral infections, zoonoses |
| Noninfectious inflammatory | Still's disease, RA, SLE, reactive arthritis, sarcoidosis, vasculitis, polymyalgia rheumatica, IBD, Familial Mediterranean Fever |
| Malignant | Lymphoma, leukemia, myelodysplastic syndrome; renal cell carcinoma, metastatic carcinoma, colon cancer, HCC, atrial myxoma |
| Other | Drug fever, factitious fever, undiagnosed in ~20% of cases |
Key History Clues
| Feature | Consider |
|---|---|
| Travel history | Malaria, typhoid, viral hemorrhagic fevers, leishmaniasis |
| Zoonotic exposure | Brucellosis, Q fever, tularemia, bartonellosis (cat scratch) |
| Medications | Drug fever (often with eosinophilia, rash, ALP elevation) |
| IV drug use / prosthetic valve | Endocarditis |
| Indwelling catheter / surgery | Hospital-acquired: C. diff, wound infection, vascular catheter infection |
| Morning stiffness >1 hour | Rheumatoid arthritis, Still's disease |
| B symptoms (night sweats, weight loss) | Lymphoma, TB, endocarditis |
| Periodic/recyclical pattern | Malaria, Familial Mediterranean Fever, lymphoma (Pel-Ebstein) |
| Immunocompromised (HIV, chemo) | Opportunistic infections, broader organism coverage |
Lab & Imaging Approach
- Respiratory: sputum culture, PCR panel, procalcitonin
- Meningeal signs: LP (cell count, glucose, protein, culture, PCR)
- GI/abdominal: CT abdomen/pelvis
- Cardiac murmur: Echocardiogram, serial blood cultures
- Prolonged FUO: ANA, RF, ESR, CRP, ferritin (markedly elevated in Still's), SPEP, LDH, HIV, hepatitis serologies, PPD/IGRA, CT chest/abdomen/pelvis, PET scan if malignancy suspected
- Rosen's Emergency Medicine: Concepts and Clinical Practice (Table 8.1, Box 8.1, Figs. 8.1-8.2)
- Goldman-Cecil Medicine, Ch. 259 (Diagnosis of fever, inpatient vs. outpatient approach)
- Frameworks for Internal Medicine (FUO categories and clinical reasoning framework)
seizure management with proper pathway with doctors order case sheet
- Phase 0 (0-2 min): Safety, positioning, call for help
- Phase 1 (0-5 min): ABCs, O2, IV access, glucose, labs
- Phase 2 (5-20 min): 1st-line benzodiazepines with doses and route selection
- Phase 3/4 (20-60 min): 2nd-line AEDs (fosphenytoin, levetiracetam, valproate, lacosamide) then refractory SE agents (midazolam infusion, propofol, ketamine, phenobarbital, pentobarbital)
explain with a seizure case
Case-Based Seizure Management Walkthrough
THE CASE
Mr. Arjun R., 34-year-old male Brought to the Emergency Department by his wife at 10:05 AM Chief complaint (per wife): "He collapsed and started shaking while having breakfast. He hasn't woken up properly."
SCENE: ARRIVAL - T = 0 min
- Seizure started approximately 8 minutes ago (so this is already established status epilepticus on arrival)
- No prior history of seizures or epilepsy
- No known drug allergies
- Not on any regular medications
- Had complained of headache for 2 days and appeared feverish last night
- No alcohol or drug use
- No recent travel
- Weight approximately 70 kg
| Parameter | Value |
|---|---|
| BP | 148/92 mmHg |
| HR | 118 bpm |
| RR | 22 breaths/min |
| SpO2 | 89% on room air |
| Temperature | 38.7°C (101.7°F) |
| GCS | E1V1M2 = 4 (unresponsive, posturing) |
STEP 1 - IMMEDIATE TEAM RESPONSE (T = 0-2 min)
- Lateral (recovery) position - right lateral decubitus
- Pad side rails, lower bed
- Suction pooled secretions from oropharynx
- Place on cardiac monitor, pulse oximeter
- Two large-bore IVs inserted (right antecubital + left forearm)
- BP cuff - continuous cycling q5 min
- Seizure started ~8 min ago = already status epilepticus (>5 min threshold crossed)
- Fever + headache for 2 days + new-onset seizure = bacterial meningitis must be on the differential until proven otherwise
- SpO2 89% - immediate O2 required
O2 via non-rebreather mask at 15 L/min - target SpO2 > 94%
STEP 2 - FIRST-LINE: BENZODIAZEPINE (T = 2-5 min)
╔══════════════════════════════════════════════════════════╗
║ ORDER 1 - FIRST-LINE BENZODIAZEPINE ║
║ ║
║ Lorazepam (Ativan) 0.1 mg/kg IV slow push ║
║ = 0.1 × 70 kg = 7 mg → give 4 mg IV (max per dose) ║
║ ║
║ Administer over 2 minutes ║
║ If seizure continues at 5 min → REPEAT x1 ║
║ Repeat dose: Lorazepam 4 mg IV ║
╚══════════════════════════════════════════════════════════╝
STEP 3 - SECOND-LINE AED (T = 10-20 min)
- No cardiac monitoring needed (unlike fosphenytoin/phenytoin)
- Safe in patients with unknown cardiac status
- Can be given rapidly
- No interaction with planned meningitis antibiotics
╔══════════════════════════════════════════════════════════╗
║ ORDER 2 - SECOND-LINE AED ║
║ ║
║ Levetiracetam (Keppra) 60 mg/kg IV ║
║ = 60 × 70 kg = 4200 mg IV ║
║ → Give 4000 mg IV in 100 mL NS over 15 minutes ║
║ ║
║ Rate: 267 mL/h via infusion pump ║
╚══════════════════════════════════════════════════════════╝
╔══════════════════════════════════════════════════════════╗
║ ORDER 3 - EMPIRIC MENINGITIS TREATMENT ║
║ (Fever + Headache 2 days + New seizure = HIGH SUSPICION ║
║ Do NOT wait for LP - treat immediately) ║
║ ║
║ Ceftriaxone 2 g IV q12h - STAT first dose ║
║ Vancomycin 25 mg/kg IV (= 1750 mg) q8-12h - STAT ║
║ Dexamethasone 0.15 mg/kg IV q6h x4 days ║
║ = 10.5 mg → give 10 mg IV (before or with 1st abx) ║
║ Acyclovir 10 mg/kg IV q8h (= 700 mg) - cover HSV ║
╚══════════════════════════════════════════════════════════╝
STEP 4 - REFRACTORY STATUS EPILEPTICUS (T = 22-30 min)
- Seizure has now lasted >22 minutes total
- Two adequate AED agents failed (lorazepam x2 + levetiracetam)
- SpO2 is falling despite O2 - 88% now
- Patient cannot protect airway
- Continuous EEG monitoring needed
RSI Orders:
╔══════════════════════════════════════════════════════════╗
║ ORDER 4 - RSI (RAPID SEQUENCE INTUBATION) ║
║ ║
║ Pre-oxygenation: 100% O2 via BVM x3-5 min ║
║ ║
║ INDUCTION: ║
║ Ketamine 2 mg/kg IV = 140 mg IV push ║
║ (chosen: hemodynamically stable, may reduce seizures) ║
║ ║
║ PARALYTIC (SHORT-ACTING ONLY): ║
║ Succinylcholine 1.5 mg/kg IV = 105 mg IV push ║
║ *** SHORT-ACTING - duration 10 min *** ║
║ *** DO NOT use vecuronium/rocuronium long-acting *** ║
║ *** Paralysis will MASK ongoing seizure activity *** ║
║ ║
║ Post-intubation: Continuous EEG monitoring - STAT ║
║ ETT confirmed by waveform capnography + CXR ║
╚══════════════════════════════════════════════════════════╝
Why short-acting paralytic only? Long-acting paralytics stop the visible shaking but seizure activity continues silently in the brain (non-convulsive SE). EEG is the only way to detect ongoing seizure after paralysis.
Continuous Infusion for Refractory SE:
╔══════════════════════════════════════════════════════════╗
║ ORDER 5 - REFRACTORY SE INFUSION ║
║ ║
║ Midazolam (Versed): ║
║ Loading dose: 0.2 mg/kg IV = 14 mg IV bolus ║
║ Then infusion: start at 0.05 mg/kg/h = 3.5 mg/h ║
║ Titrate by 0.05 mg/kg/h q15 min to seizure cessation ║
║ on EEG (max 2 mg/kg/h) ║
║ ║
║ Vasopressor on standby (hypotension anticipated): ║
║ Norepinephrine 0.05-0.3 mcg/kg/min if MAP < 65 mmHg ║
╚══════════════════════════════════════════════════════════╝
STEP 5 - DIAGNOSTIC WORKUP (now seizure is controlled)
╔══════════════════════════════════════════════════════════╗
║ ORDER 6 - STAT LABS & IMAGING ║
║ ║
║ Blood: ║
║ - CBC with differential ║
║ - CMP: Na, K, Ca, Mg, Cl, CO2, BUN, Creatinine, glucose║
║ - LFTs + ammonia ║
║ - Serum lactate ║
║ - Blood cultures x2 (BEFORE antibiotics if possible, ║
║ but DO NOT delay antibiotics for cultures) ║
║ - HIV screen ║
║ - CRP, ESR, procalcitonin ║
║ - ABG (patient intubated) ║
║ ║
║ Imaging: ║
║ - CT brain non-contrast STAT ║
║ - CT brain with contrast (after non-contrast) ║
║ ║
║ Lumbar Puncture: ║
║ - AFTER CT brain clears herniation risk ║
║ - CSF: cell count, glucose, protein, Gram stain, ║
║ culture, HSV PCR, cryptococcal antigen, VDRL ║
╚══════════════════════════════════════════════════════════╝
STEP 6 - RESULTS & DIAGNOSIS
| Test | Result | Interpretation |
|---|---|---|
| WBC | 18,400/μL (84% neutrophils, bands 12%) | Marked neutrophilia - bacterial infection |
| Na | 128 mEq/L | Hyponatremia (SIADH from meningitis) |
| Ca | 9.1 mg/dL | Normal |
| Mg | 1.9 mg/dL | Normal |
| Glucose | 79 mg/dL | Normal |
| CRP | 142 mg/L | Markedly elevated |
| Procalcitonin | 8.4 ng/mL | Strongly suggests bacterial infection |
| Blood cultures | Pending | - |
| CSF Parameter | Result | Normal |
|---|---|---|
| Opening pressure | 28 cm H2O | <20 |
| Appearance | Cloudy, turbid | Clear |
| WBC | 2,800/μL (95% PMNs) | <5 |
| Glucose | 22 mg/dL | >60% serum glucose |
| Protein | 385 mg/dL | 15-45 |
| Gram stain | Gram-positive diplococci | - |
STEP 7 - ONGOING MANAGEMENT & ICU ORDERS
╔══════════════════════════════════════════════════════════╗
║ FINAL STANDING ORDERS - NEURO ICU ║
║ ║
║ ANTIBIOTIC REGIMEN (continue): ║
║ Ceftriaxone 2 g IV q12h x14 days ║
║ Vancomycin - dose by pharmacy per levels ║
║ (target AUC/MIC 400-600) ║
║ Dexamethasone 0.15 mg/kg IV q6h x4 days (COMPLETE) ║
║ (reduces neurologic complications in pneumococcal) ║
║ Acyclovir - STOP once HSV PCR returns negative ║
║ ║
║ SEIZURE PROPHYLAXIS / MAINTENANCE: ║
║ Levetiracetam 500 mg IV q12h (maintenance dose) ║
║ Continue until seizure-free x48h then reassess ║
║ ║
║ MIDAZOLAM WEAN: ║
║ When EEG seizure-free x24h: decrease by 25% q4-6h ║
║ ║
║ HYPONATREMIA CORRECTION (Na 128): ║
║ Fluid restrict to 1000 mL/24h ║
║ 3% NaCl NOT needed (Na not < 120, no herniation) ║
║ Recheck Na q6h; correct no faster than 8-10 mEq/L/day ║
║ (rapid correction → osmotic demyelination syndrome) ║
║ ║
║ VENTILATOR SETTINGS (post-intubation): ║
║ Mode: Volume AC TV: 6 mL/kg IBW (= 420 mL) ║
║ PEEP: 5 cmH2O FiO2: 0.4 RR: 14 ║
║ Target: SpO2 >94%, PaCO2 35-40 mmHg ║
║ ║
║ MONITORING: ║
║ Continuous EEG x48h minimum ║
║ Neuro checks q1h (pupils, GCS as assessable) ║
║ ICP monitoring if clinical deterioration ║
║ HOB elevation 30° (reduce ICP) ║
╚══════════════════════════════════════════════════════════╝
CASE TIMELINE SUMMARY
T = 0 min → Patient arrives, actively seizing (~8 min into seizure)
→ O2, monitors, IV access, POC glucose
→ STATUS EPILEPTICUS declared
T = 2 min → Lorazepam 4 mg IV (1st dose)
T = 7 min → Lorazepam 4 mg IV (2nd dose)
→ No response → move to 2nd-line
T = 10 min → Levetiracetam 4000 mg IV started (over 15 min)
→ EMPIRIC MENINGITIS antibiotics started (ceftriaxone,
vancomycin, dexamethasone, acyclovir)
T = 22 min → Levetiracetam complete, seizure CONTINUES
→ REFRACTORY SE declared → intubation decision
T = 25 min → RSI: Ketamine 140 mg IV + Succinylcholine 105 mg IV
→ Intubated; continuous EEG attached
T = 28 min → Midazolam 14 mg IV bolus + infusion started 0.05 mg/kg/h
T = 35 min → EEG confirms SEIZURE CESSATION
→ Midazolam titrated to 0.1 mg/kg/h
T = 45 min → CT brain: meningeal enhancement, no herniation
T = 60 min → LP performed: CSF confirms bacterial meningitis
T = 90 min → Patient in Neuro-ICU, sedated but hemodynamically stable
→ Blood cultures growing Gram-positive diplococci
→ Antibiotics narrowed to high-dose ceftriaxone
Day 3 → EEG seizure-free; midazolam weaned and discontinued
→ Extubated; following commands
→ Na corrected to 136 mEq/L
Day 7 → Transfer to step-down; levetiracetam continued orally
→ Neurology follow-up arranged
→ Outpatient EEG in 4 weeks
KEY TEACHING POINTS FROM THIS CASE
| Point | Lesson |
|---|---|
| Fever + new seizure = meningitis until proven otherwise | Do not delay antibiotics waiting for LP or CT |
| Treat empirically before diagnosis is confirmed | Antibiotics + antivirals started at T=10 min, diagnosis confirmed at T=60 min |
| Benzodiazepines: max 2 doses then escalate | More doses = more respiratory depression, not more seizure control |
| Short-acting paralytic only during RSI | Long-acting masks ongoing electrical seizure activity |
| Hyponatremia contributed to seizure | Na 128 from SIADH (meningitis) lowers seizure threshold |
| Never delay treatment to do LP | LP is done AFTER CT clears herniation AND after antibiotics are started |
| Levetiracetam preferred 2nd-line here | No cardiac monitoring needed, rapid administration, safe with unknown cardiac history |
| Continuous EEG is mandatory post-intubation | NCSE (non-convulsive SE) is present in up to 24% of comatose patients |
Pregnancy safe Drugs with Frequency, case wise & tips tricks, clinical pearls
Pregnancy-Safe Drugs: Complete Clinical Reference
Understanding Drug Safety in Pregnancy
| Old FDA Category | Meaning |
|---|---|
| A | Controlled studies show no fetal risk - safest |
| B | Animal studies show no risk; no adequate human studies, OR animal risk not confirmed in humans |
| C | Animal studies show adverse effects; no adequate human data; give only if benefit outweighs risk |
| D | Evidence of human fetal risk; benefit may outweigh risk in serious conditions |
| X | Fetal risk clearly outweighs any benefit - CONTRAINDICATED |
Golden Rule: Untreated maternal disease is often MORE dangerous to the fetus than treating it with a relatively safe drug.
SECTION 1: ANTIBIOTICS IN PREGNANCY
Safe (Preferred):
| Drug | FDA Category | Safe Trimester | Frequency | Use |
|---|---|---|---|---|
| Penicillin G/Amoxicillin | B | All trimesters | Amox: 500 mg TID x7d | UTI, strep throat, dental infections, syphilis |
| Amoxicillin-Clavulanate | B | All (caution T1) | 875/125 mg BID x7d | Skin infections, sinusitis, UTI - avoid in 1st trimester if possible |
| Cephalexin (1st gen) | B | All trimesters | 500 mg QID x7d | UTI, cellulitis, skin infections |
| Ceftriaxone | B | All trimesters | 1-2 g IV/IM once daily | Severe infections, gonorrhea, meningitis |
| Azithromycin | B | All trimesters | 500 mg x1, then 250 mg OD x4d | Atypical pneumonia, chlamydia |
| Erythromycin | B | All trimesters | 500 mg QID x7d | Alternative for penicillin allergy |
| Clindamycin | B | All trimesters | 300 mg TID x7d | BV, anaerobic infections, skin infections |
| Nitrofurantoin | B | T1, T2 only | 100 mg ER BID x5d | Uncomplicated UTI - AVOID at term (>36 wk) |
| Metronidazole | B | T2, T3 (caution T1) | 500 mg BID x7d | BV, trichomoniasis, anaerobic infections |
Use with Caution / Conditional:
| Drug | FDA Category | Concern | Alternative |
|---|---|---|---|
| Trimethoprim-Sulfamethoxazole (TMP-SMX) | C/D | T1: folate antagonist (NTD risk); T3: neonatal jaundice, kernicterus | Use only if no alternative; avoid T1 and T3 |
| Ciprofloxacin/Fluoroquinolones | C | Cartilage damage in animal studies; avoid if possible | Use only for serious infections with no safer option |
| Gentamicin/Aminoglycosides | D | Fetal ototoxicity, nephrotoxicity | Short course acceptable for life-threatening sepsis |
CONTRAINDICATED:
| Drug | Risk |
|---|---|
| Tetracyclines (doxy, minocycline) | Dental discoloration, inhibits fetal bone growth |
| Chloramphenicol (T3) | Gray baby syndrome |
| Linezolid | Insufficient safety data |
📋 CASE 1: UTI in Pregnancy
Patient: Priya, 26-year-old, 18 weeks pregnant. Dysuria, frequency, urgency x2 days. Urine dipstick: nitrites +, leukocyte esterase +, no fever.
Cephalexin (Keflex) 500 mg PO QID x 7 days
(cephalosporins - Category B, safe all trimesters)
OR
Nitrofurantoin (Macrobid) 100 mg ER PO BID x 5 days
(Category B - safe T1 and T2; AVOID if > 36 weeks)
- Ciprofloxacin (fluoroquinolone - avoid)
- TMP-SMX in T1 (folate antagonist, NTD risk) or T3 (neonatal jaundice)
- All pregnant women should be screened for asymptomatic bacteriuria at first prenatal visit - UTI in pregnancy is a serious condition that can ascend to pyelonephritis
- Treat even asymptomatic bacteriuria in pregnancy (unlike non-pregnant adults)
- Repeat urine culture 7 days after treatment to confirm cure
- Consider suppressive prophylaxis (nitrofurantoin 50-100 mg at bedtime) if recurrent UTIs
SECTION 2: ANTIHYPERTENSIVES IN PREGNANCY
Safe (First-Line):
| Drug | FDA Category | Dose | Mechanism | Notes |
|---|---|---|---|---|
| Methyldopa (Aldomet) | B | 250 mg PO q6-8h; max 3 g/day | Central α2 agonist | Oldest, most studied; drug of choice historically; can cause depression/fatigue |
| Labetalol | C | 100-400 mg PO BID; IV: 20 mg bolus | α+β blocker | First-line for chronic HTN in pregnancy; also used IV for acute severe HTN |
| Nifedipine (extended-release) | C | 30-90 mg PO OD | CCB | Add-on to labetalol/methyldopa; also used for preterm labor (tocolysis) |
| Hydralazine | C | 5-10 mg IV/IM q20-40 min (acute); 10-50 mg PO QID (chronic) | Direct vasodilator | Used IV in acute hypertensive emergency; can cause reflex tachycardia |
| Nifedipine (immediate-release, oral) | C | 10-30 mg PO (acute) | CCB | For acute severe HTN in ED - not FDA-approved for this indication but used |
ABSOLUTELY CONTRAINDICATED:
| Drug | Risk |
|---|---|
| ACE inhibitors (lisinopril, enalapril, ramipril) | Fetal renal tubular dysplasia, oligohydramnios, IUGR, neonatal renal failure, skull defects - teratogenic in T2/T3 |
| ARBs (losartan, valsartan, olmesartan) | Same as ACEi - contraindicated |
| Atenolol | IUGR, bradycardia in neonate |
| Sodium nitroprusside | Cyanide toxicity to fetus |
- Chronic HTN: target 140-150/90-100 mmHg (not too tight - avoid uteroplacental insufficiency)
- Severe HTN (≥160/110 mmHg): treat urgently - risk of maternal stroke/eclampsia
📋 CASE 2: Hypertensive Emergency in Pregnancy
Patient: Sunita, 32-year-old, 34 weeks pregnant. BP 178/114 mmHg on 2 readings 15 min apart. Severe headache, epigastric pain. Urine protein +++. Platelet count 88,000. LFTs elevated 2x normal.
1. Labetalol 20 mg IV push over 2 min
If BP still ≥160/110 after 10 min → Labetalol 40 mg IV
If still not controlled → Hydralazine 5-10 mg IV q20 min
OR
Nifedipine 10-20 mg PO, may repeat in 30 min
TARGET: BP 140-150/90-100 mmHg
2. MAGNESIUM SULFATE - seizure prophylaxis:
MgSO4 4-6 g IV over 20 min (loading dose)
Then 1-2 g/h IV continuous infusion
Monitor: respiratory rate, urine output, reflexes, Mg levels
3. Delivery planning: definitive treatment for HELLP is delivery
Dexamethasone 12 mg IM q12h x2 doses (fetal lung maturity if <34 wk)
- Magnesium sulfate is NOT an antihypertensive - it is specifically for seizure prevention in preeclampsia
- Toxicity signs of Mg: loss of DTRs (first sign), respiratory depression, cardiac arrest
- Antidote for Mg toxicity: Calcium gluconate 1 g IV push
- NEVER use ACEi or ARB - even a single dose in T2/T3 can cause fetal renal failure
SECTION 3: ANALGESICS & ANTIPYRETICS
| Drug | FDA Category | Safe Trimester | Notes |
|---|---|---|---|
| Paracetamol/Acetaminophen | B | All trimesters (short-term) | Drug of choice for pain and fever in all trimesters; recent data on prolonged use showing possible ADHD link but short-term use acceptable |
| Opioids (codeine, morphine, oxycodone) | C (T1/T2) / D (T3) | Short-term use only | Risk of NAS (neonatal abstinence syndrome) with prolonged use; avoid at term |
CONTRAINDICATED:
| Drug | Trimester | Risk |
|---|---|---|
| NSAIDs (ibuprofen, diclofenac, naproxen) | T3 - AVOID | Premature closure of ductus arteriosus, oligohydramnios, fetal renal impairment. T1 use: possible increased miscarriage risk |
| Aspirin (full dose >150 mg/day) | T3 | Antiplatelet effects, neonatal bleeding. LOW-DOSE aspirin 75-150 mg OD is actually recommended to prevent preeclampsia |
📋 CASE 3: Acute Pain in Pregnancy (Headache/Back Pain)
Patient: Asha, 28-year-old, 24 weeks pregnant. Severe tension headache and low back pain.
1. Paracetamol 500-1000 mg PO q6-8h PRN (max 4 g/day) - FIRST LINE
2. Warm compress for back pain (not hot - no heating pads directly on abdomen)
3. Non-pharmacologic: physiotherapy, support belt for back pain
- Ibuprofen/diclofenac at 24 weeks - although T2 is technically the grey zone, NSAIDs are generally avoided as a habit-forming risk
- Aspirin >150 mg - antiplatelet risk
SECTION 4: ANTIEMETICS (Nausea/Vomiting in Pregnancy)
| Drug | FDA Category | Dose | Notes |
|---|---|---|---|
| Pyridoxine (Vitamin B6) | A | 10-25 mg TID | First-line; safest; take 30 min before meals |
| Doxylamine + Pyridoxine (Diclegis/Bonjesta) | A | 2 tabs at bedtime (delayed-release) | FDA-approved combination; gold standard for NVP |
| Ginger (non-pharmacologic) | - | 250 mg QID or ginger tea | Shown effective in multiple trials; safe |
| Metoclopramide | B | 10 mg IV/PO TID | Safe; risk of extrapyramidal effects with prolonged use |
| Promethazine | C | 12.5-25 mg PO/IV/IM q4-6h | Effective but sedating; AAP cautions in nursing |
| Prochlorperazine | C | 5-10 mg PO/IV TID-QID | For refractory NVP; sedating |
| Ondansetron (Zofran) | B | 4-8 mg IV/PO q6-8h | Use for severe/refractory cases; some studies suggest possible cardiac septum defect and cleft palate risk - data inconsistent. Avoid in T1 if possible, use if severely symptomatic |
- Dietary changes + ginger
- Pyridoxine alone 25 mg TID
- Add doxylamine (Doxylamine/Pyridoxine combination)
- Add metoclopramide or promethazine
- Ondansetron for refractory cases
- IV fluids + IV antiemetics (admit for hyperemesis gravidarum)
📋 CASE 4: Hyperemesis Gravidarum
Patient: Riya, 10 weeks pregnant, 5 kg weight loss, unable to tolerate any oral intake, ketonuria ++, vomiting 12x/day.
ADMIT - IV Access
1. IV Fluids: Normal saline 0.9% + 40 mEq KCl/L @ 125 mL/h
(correct dehydration + electrolytes)
2. Thiamine 100 mg IV BEFORE glucose infusion
(prevent Wernicke's encephalopathy)
3. Ondansetron 4 mg IV q8h
+ Metoclopramide 10 mg IV TID
4. Pyridoxine 25 mg IV/PO TID (continue throughout)
5. Once tolerating oral fluids:
Step down to oral antiemetics
Doxylamine/Pyridoxine 2 tabs HS
6. Monitor: electrolytes, LFTs (exclude acute fatty liver), TFTs
(HCG stimulates TSH-R → gestational thyrotoxicosis in 60% of HG)
- Always give thiamine BEFORE IV dextrose to prevent Wernicke's encephalopathy
- Check TFTs: TSH is often suppressed in hyperemesis - transient gestational thyrotoxicosis does NOT need antithyroid treatment, it resolves as HCG falls
- Ondansetron: Use cautiously in T1 (some data for cleft palate), but risk of dehydration from untreated HG outweighs this theoretical risk
SECTION 5: ANTIEPILEPTIC DRUGS (AEDs) IN PREGNANCY
| Drug | Malformation Risk | Specific Risk | Verdict |
|---|---|---|---|
| Lamotrigine | Lowest among AEDs (~1%) | Levels fall precipitously in pregnancy - monitor and adjust | Preferred AED in pregnancy |
| Levetiracetam | Low (not associated with increased malformations) | Levels may fall; adjust by monitoring | Preferred; rapidly gaining favor |
| Carbamazepine | 4-5% major malformations | Cleft palate, NTD, fetal anticonvulsant syndrome | Use only if only effective agent |
| Phenytoin | 4-5% | Fetal hydantoin syndrome: midface hypoplasia, finger hypoplasia, NTD | Avoid if possible |
| Phenobarbital | 6-7% | NTDs, cardiac defects, cleft palate; neonatal bleeding | Avoid if possible |
| Valproate | 20% serious adverse outcomes | NTD (spina bifida 1-2%), cardiac defects, autism, IQ reduction (9 points), fetal valproate syndrome | AVOID - absolute contraindication in women of childbearing age without contraception |
| Topiramate | ~4% | Cleft palate, IUGR | Avoid |
- NEVER stop AEDs abruptly (risk of GTCS is more dangerous than AED exposure)
- Use monotherapy at lowest effective dose - polytherapy multiplies risk
- Folic acid 5 mg/day (high-dose) from pre-conception through T1
- Monitor drug levels every trimester (clearance increases in pregnancy)
- Neonates exposed to AEDs - give Vitamin K 1 mg IM at birth (AEDs reduce Vitamin K-dependent clotting factors)
SECTION 6: THYROID DRUGS IN PREGNANCY
| Drug | Safety | Dose | Notes |
|---|---|---|---|
| Levothyroxine (T4) | Safe - Category A | Adjust to maintain TSH 0.1-2.5 mIU/L | Hypothyroidism MUST be treated - untreated leads to fetal neurological damage; requirements increase ~25-30% in pregnancy |
| Propylthiouracil (PTU) | Preferred in T1 | Lowest effective dose; TID dosing | Drug of choice for hyperthyroidism in T1 (hepatotoxicity risk but crosses placenta less than methimazole) |
| Methimazole (MMI/Carbimazole) | Use in T2/T3 | Lowest effective dose; OD or BID dosing | Associated with aplasia cutis and "methimazole embryopathy" in T1 - switch to PTU in T1, back to MMI in T2 |
- T1: Use PTU (less teratogenic in organogenesis period)
- T2 onwards: Switch to Methimazole (PTU has more hepatotoxicity with prolonged use)
- At delivery: Risk of neonatal thyroid disease from maternal antibodies - check neonatal TSH
📋 CASE 5: Hyperthyroidism in Pregnancy
Patient: Nidhi, 8 weeks pregnant. Palpitations, tremor, weight loss despite increased appetite. TSH < 0.01, FT4 elevated 3x normal. Anti-TPO antibodies positive. Thyroid scan shows diffuse uptake.
Propylthiouracil (PTU) 100 mg PO TID
(preferred in T1 - less teratogenic during organogenesis)
Target: FT4 in upper normal range;
do NOT normalize TFTs (risk of fetal hypothyroidism)
At 13 weeks: Switch to Methimazole 10-20 mg PO OD
Monitor: TFTs q4 weeks; adjust dose to maintain FT4 high-normal
Check fetal heart rate at each visit - fetal tachycardia suggests
fetal hyperthyroidism from maternal antibody transfer
NEVER use: Radioiodine (I-131) - destroys fetal thyroid
NEVER use: Atenolol for prolonged rate control (IUGR risk)
Propranolol: short-term use acceptable for symptomatic tachycardia
SECTION 7: ANTICOAGULANTS IN PREGNANCY
| Drug | Safety | Route | Notes |
|---|---|---|---|
| Heparin (unfractionated) | Safe - does NOT cross placenta | IV/SC | Safe in all trimesters; drug of choice for anticoagulation in pregnancy |
| Low-Molecular-Weight Heparin (LMWH) - Enoxaparin, Dalteparin | Safe - does NOT cross placenta | SC | Preferred over UFH (once or twice daily SC; more predictable); dose-adjust by anti-Xa levels |
| Warfarin | Category D/X | Oral | Teratogenic in T1 (warfarin embryopathy: nasal hypoplasia, stippled epiphyses); CNS defects in T2/T3; fetal bleeding |
| Direct oral anticoagulants (DOACs) - apixaban, rivaroxaban | CONTRAINDICATED | Oral | Cross placenta; teratogenic; insufficient safety data |
SECTION 8: ANTIDEPRESSANTS & PSYCHIATRIC DRUGS
| Drug | FDA Category | Verdict |
|---|---|---|
| SSRIs - Sertraline, Fluoxetine | C | Generally preferred if antidepressant needed; sertraline has best safety profile in pregnancy; avoid paroxetine (cardiac septal defects) |
| Sertraline | C | Most commonly used SSRI in pregnancy; minimal placental transfer |
| Paroxetine | D | Increased cardiac defects (VSD); AVOID |
| SNRIs - Venlafaxine | C | Limited data; use if SSRI inadequate |
| TCAs | C/D | Avoid if possible; nortriptyline safer than amitriptyline |
| Lithium | D | Ebstein's anomaly (small but real risk); requires detailed fetal cardiac echo at 20 weeks if used |
| Valproate | D | AVOID in pregnancy for psychiatric indications |
| Benzodiazepines | D | Neonatal withdrawal syndrome; cleft palate risk debated; avoid in T1; use minimum effective dose if needed in acute anxiety |
| Antipsychotics (olanzapine, quetiapine) | C | Risk of neonatal extrapyramidal symptoms; use lowest effective dose; all carry metabolic risks in mother |
- Review necessity of all drugs
- Aim for monotherapy at lowest effective dose
- Restart abruptly-discontinued medication if relapse occurs - relapse is more dangerous
- Continue throughout pregnancy if condition is severe (depression increases obstetric risk)
SECTION 9: ASTHMA DRUGS IN PREGNANCY
| Drug | Safety | Notes |
|---|---|---|
| Salbutamol/Albuterol (SABA inhaler) | B - Safe | Drug of choice for acute bronchospasm; use unrestricted |
| Budesonide (ICS) | B - Preferred | Preferred inhaled corticosteroid; most safety data |
| Fluticasone (ICS) | C - Acceptable | Less data than budesonide but widely used |
| Salmeterol (LABA) | C - Use with ICS only | Add-on to ICS for poorly controlled asthma |
| Montelukast (LTRA) | B - Safe | Can continue if well controlled on it pre-pregnancy |
| Oral prednisolone | C - Use for exacerbations | Risk of cleft palate with T1 use (small); risk of uncontrolled asthma far greater - use when needed |
| Theophylline | C - Use with caution | Narrow therapeutic index; neonatal toxicity; use only if other agents fail |
SECTION 10: ANTIFUNGALS
| Drug | Safety | Notes |
|---|---|---|
| Clotrimazole (topical) | B - Safe | First-line for VVC (vaginal candidiasis) in pregnancy |
| Miconazole (topical) | C - Acceptable | Topical use safe |
| Nystatin (topical/oral) | B - Safe | Oral nystatin for thrush - minimal systemic absorption |
| Fluconazole oral | D - AVOID | Single dose (150 mg) controversial; repeated doses linked to fetal cardiac defects and craniosynostosis. Avoid especially in T1 |
| Amphotericin B | B - Acceptable | For serious systemic fungal infections only |
MASTER QUICK-REFERENCE TABLE
| Condition | First Choice | Avoid |
|---|---|---|
| UTI | Cephalexin, Nitrofurantoin (avoid T3) | TMP-SMX (T1, T3), fluoroquinolones |
| Hypertension | Labetalol, Methyldopa, Nifedipine ER | ACEi, ARBs, atenolol |
| HTN emergency | Labetalol IV, Hydralazine IV, Nifedipine oral | Sodium nitroprusside |
| Eclampsia seizure | Magnesium sulfate IV | Phenytoin (less effective) |
| Nausea/vomiting | Pyridoxine + Doxylamine, Metoclopramide | None first-line |
| Pain/fever | Paracetamol | NSAIDs (T3), full-dose aspirin |
| Diabetes | Insulin (preferred), Metformin (T2D/GDM) | Sulfonylureas (stop 2 wk before delivery) |
| Hypothyroidism | Levothyroxine | - |
| Hyperthyroidism | PTU (T1), Methimazole (T2/T3) | Radioiodine (I-131) |
| Epilepsy | Lamotrigine, Levetiracetam | Valproate, Topiramate |
| DVT/PE | LMWH (Enoxaparin) | Warfarin (T1), DOACs |
| Asthma (acute) | Salbutamol inhaler, Budesonide ICS | - |
| Depression | Sertraline | Paroxetine, Valproate |
| VVC (candida) | Clotrimazole topical | Oral fluconazole (T1) |
| Preeclampsia prophylaxis | Low-dose Aspirin 75-150 mg OD from 12 wk | - |
UNIVERSAL CLINICAL PEARLS FOR PRESCRIBING IN PREGNANCY
-
"The disease treats the fetus too" - untreated hypertension, seizures, asthma, diabetes, and depression all carry significant fetal risk. Never withhold necessary treatment.
-
Folic acid 400 mcg/day for all women planning pregnancy (start 1 month before conception); 5 mg/day for high-risk patients (epilepsy, diabetes, BMI >30, previous NTD).
-
T1 (weeks 1-12) is organogenesis - highest teratogenesis risk. T2/T3 risks are more about fetal growth, function, and neonatal adaptation.
-
Always give the lowest effective dose and for the shortest needed duration.
-
Monotherapy over polypharmacy - drug combinations multiply teratogenic risk non-linearly.
-
Check every drug before prescribing - use TERIS, LactMed, or Drugs@FDA as reference databases.
-
Neonatal effects to watch: Neonatal abstinence syndrome (opioids, benzodiazepines, SSRIs), neonatal hypoglycemia (sulfonylureas, beta-blockers), neonatal bradycardia (labetalol, atenolol), neonatal hypothyroidism (antithyroid drugs).
-
Inform the patient - shared decision-making is essential for all drug prescribing in pregnancy.
-
The 1-month rule: Warfarin embryopathy occurs at weeks 6-12 - risk window overlaps with time before many women know they are pregnant. Women of childbearing age on warfarin MUST use contraception.
-
Supplementation always needed: Iron (from 12 weeks or earlier if anaemic), folic acid, iodine (in iodine-deficient regions), Vitamin D 400-1000 IU/day.
ortho cases with proper drug dose and frequency with clinical case examples opd,ward & icu
What's Covered:
OPD Cases (3)
- Acute Gout - Colchicine, NSAIDs, intra-articular steroid; urate-lowering therapy timing rules
- OA Knee - Step-up analgesic ladder from paracetamol → topical NSAID → oral COX-2 → IA injection → tramadol
- Ankle Sprain - POLICE protocol, Ottawa rules, ibuprofen dosing, grading-based management
Ward Cases (3)
- Post-THR Day 1 - Complete multimodal analgesic regimen, 35-day enoxaparin VTE prophylaxis, hip precautions, bowel care, bone health, physio
- Open Tibial Fracture Grade IIIB - Emergency resuscitation, Gustilo-graded antibiotic selection with timing, tetanus prophylaxis, fasciotomy monitoring
- Septic Arthritis - Gram stain-guided empiric antibiotics (vancomycin + ceftriaxone), mandatory drainage, duration by joint type, de-escalation strategy
ICU Cases (3)
- Acute Compartment Syndrome - Fasciotomy threshold (delta pressure < 30 mmHg), rhabdomyolysis IV fluid protocol, CK monitoring targets
- Fat Embolism Syndrome - Gurd criteria, methylprednisolone 1.5 mg/kg q8h x3 days, ARDS ventilation principles
- Diabetic Foot Osteomyelitis + Septic Shock - Sepsis bundle, polymicrobial broad-spectrum empiric (Vancomycin + Pip-Taz), 6-week duration, oral step-down options, glycaemic control
how to approach to decide insulin dose as oer weight and glucose concentration ,HbA1C value,how to diagnose diabetes,drugs ladder for treatment , treatment plan as per opd,ward and icu in detail manner with conceptual explanation in short becoming master in diabetic management
What You Just Got - Complete Roadmap:
Part 1 - Concept (Mental Model)
Part 2 - Diagnosis
Part 3 - Insulin Mastery
- TDD formula: 0.4-0.5 u/kg (lower for elderly/CKD; higher for obese/ICU)
- 50:50 split: Basal vs Bolus
- Correction dose (ISF) = 1800 ÷ TDD - how much 1 unit drops glucose
- Titration rules: 3-3-3 method for Glargine
- Sliding scale with dose table
- Adjustments for renal failure, fasting, steroids, surgery
Part 4 - Drug Ladder
Parts 5-7 - Cases by Setting
| Setting | Case |
|---|---|
| OPD | New T2DM (metformin initiation); T2DM + post-MI (GLP-1/SGLT-2 switch) |
| Ward | New T1DM severe hyperglycaemia (basal-bolus SC protocol); Inpatient T2DM on antibiotics (hold oral meds, temporary insulin) |
| ICU | DKA (fluid → K+ → insulin sequence; transition protocol); HHS (fluids-first concept; osmolality correction rate); Post-cardiac surgery stress hyperglycaemia (IV insulin infusion titration; NICE-SUGAR target 140-180) |
Generate a PDF quick-reference card with insulin dosing formulas and sliding scales
ls -la /home/daytona/workspace/ 2>/dev/null || echo "workspace empty or not found"
mkdir -p /home/daytona/workspace/insulin-ref && python3 -c "import reportlab; print('reportlab ok')" && python3 -c "from reportlab.lib.pagesizes import A4; print('A4 ok')"
~/insulin-ref/build_pdf.py
from reportlab.lib.pagesizes import A4
from reportlab.lib import colors
from reportlab.lib.units import mm
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle,
HRFlowable, KeepTogether
)
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.enums import TA_CENTER, TA_LEFT, TA_RIGHT
from reportlab.platypus import PageTemplate, Frame
from reportlab.pdfgen import canvas as pdfcanvas
OUTPUT = "/home/daytona/workspace/insulin-ref/Insulin_Quick_Reference.pdf"
# ── colour palette ──────────────────────────────────────────────────────────
C_NAVY = colors.HexColor("#1a3a5c")
C_TEAL = colors.HexColor("#0d7377")
C_LTBL = colors.HexColor("#e8f4f8")
C_AMBER = colors.HexColor("#f5a623")
C_AMBER2 = colors.HexColor("#fff3cd")
C_RED = colors.HexColor("#c0392b")
C_LRED = colors.HexColor("#fde8e8")
C_GREEN = colors.HexColor("#1a7a4a")
C_LGRN = colors.HexColor("#e8f8ee")
C_GREY = colors.HexColor("#f2f4f7")
C_DKGRY = colors.HexColor("#4a4a4a")
C_WHITE = colors.white
W, H = A4 # 595 x 842 pt
# ── styles ──────────────────────────────────────────────────────────────────
styles = getSampleStyleSheet()
def S(name, **kw):
return ParagraphStyle(name, **kw)
sTitle = S("sTitle", fontName="Helvetica-Bold", fontSize=20,
textColor=C_WHITE, alignment=TA_CENTER, spaceAfter=2)
sSub = S("sSub", fontName="Helvetica", fontSize=10,
textColor=C_WHITE, alignment=TA_CENTER, spaceAfter=0)
sH1 = S("sH1", fontName="Helvetica-Bold", fontSize=11,
textColor=C_WHITE, alignment=TA_LEFT, spaceBefore=0, spaceAfter=0)
sH2 = S("sH2", fontName="Helvetica-Bold", fontSize=9,
textColor=C_NAVY, alignment=TA_LEFT, spaceBefore=4, spaceAfter=2)
sBody = S("sBody", fontName="Helvetica", fontSize=8,
textColor=C_DKGRY, leading=11, spaceBefore=1, spaceAfter=1)
sBold = S("sBold", fontName="Helvetica-Bold", fontSize=8,
textColor=C_DKGRY, leading=11)
sSmall = S("sSmall", fontName="Helvetica", fontSize=7,
textColor=C_DKGRY, leading=10)
sNote = S("sNote", fontName="Helvetica-Oblique", fontSize=7,
textColor=colors.HexColor("#666666"), leading=10)
sCtr = S("sCtr", fontName="Helvetica-Bold", fontSize=8,
textColor=C_DKGRY, alignment=TA_CENTER)
sWht = S("sWht", fontName="Helvetica-Bold", fontSize=8,
textColor=C_WHITE, alignment=TA_CENTER)
sFormula = S("sFormula", fontName="Helvetica-Bold", fontSize=9,
textColor=C_TEAL, alignment=TA_CENTER, spaceBefore=3, spaceAfter=3)
sAlert = S("sAlert", fontName="Helvetica-Bold", fontSize=8,
textColor=C_RED, alignment=TA_LEFT)
sGreen = S("sGreen", fontName="Helvetica-Bold", fontSize=8,
textColor=C_GREEN, alignment=TA_LEFT)
# ── helpers ──────────────────────────────────────────────────────────────────
def section_header(title):
"""Teal band with white text."""
t = Table([[Paragraph(title, sH1)]], colWidths=[W - 30*mm])
t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), C_TEAL),
("TOPPADDING", (0,0), (-1,-1), 4),
("BOTTOMPADDING", (0,0), (-1,-1), 4),
("LEFTPADDING", (0,0), (-1,-1), 8),
("RIGHTPADDING", (0,0), (-1,-1), 8),
("ROUNDEDCORNERS", [3, 3, 3, 3]),
]))
return t
def navy_header(title):
"""Navy band."""
t = Table([[Paragraph(title, sH1)]], colWidths=[W - 30*mm])
t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), C_NAVY),
("TOPPADDING", (0,0), (-1,-1), 4),
("BOTTOMPADDING", (0,0), (-1,-1), 4),
("LEFTPADDING", (0,0), (-1,-1), 8),
("RIGHTPADDING", (0,0), (-1,-1), 8),
]))
return t
def amber_box(text):
t = Table([[Paragraph(text, sBold)]], colWidths=[W - 30*mm])
t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), C_AMBER2),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING", (0,0), (-1,-1), 5),
("LEFTPADDING", (0,0), (-1,-1), 8),
("RIGHTPADDING", (0,0), (-1,-1), 8),
("BOX", (0,0), (-1,-1), 1, C_AMBER),
]))
return t
def red_box(text):
t = Table([[Paragraph(text, sAlert)]], colWidths=[W - 30*mm])
t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), C_LRED),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING", (0,0), (-1,-1), 5),
("LEFTPADDING", (0,0), (-1,-1), 8),
("RIGHTPADDING", (0,0), (-1,-1), 8),
("BOX", (0,0), (-1,-1), 1, C_RED),
]))
return t
def green_box(text):
t = Table([[Paragraph(text, sGreen)]], colWidths=[W - 30*mm])
t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), C_LGRN),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING", (0,0), (-1,-1), 5),
("LEFTPADDING", (0,0), (-1,-1), 8),
("RIGHTPADDING", (0,0), (-1,-1), 8),
("BOX", (0,0), (-1,-1), 1, C_GREEN),
]))
return t
def formula_box(text):
t = Table([[Paragraph(text, sFormula)]], colWidths=[W - 30*mm])
t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), C_LTBL),
("TOPPADDING", (0,0), (-1,-1), 6),
("BOTTOMPADDING", (0,0), (-1,-1), 6),
("LEFTPADDING", (0,0), (-1,-1), 8),
("RIGHTPADDING", (0,0), (-1,-1), 8),
("BOX", (0,0), (-1,-1), 1.5, C_TEAL),
]))
return t
def std_table(data, col_widths, header_rows=1, zebra=True):
t = Table(data, colWidths=col_widths, repeatRows=header_rows)
style = [
("BACKGROUND", (0,0), (-1, header_rows-1), C_NAVY),
("TEXTCOLOR", (0,0), (-1, header_rows-1), C_WHITE),
("FONTNAME", (0,0), (-1, header_rows-1), "Helvetica-Bold"),
("FONTSIZE", (0,0), (-1,-1), 7.5),
("TOPPADDING", (0,0), (-1,-1), 3),
("BOTTOMPADDING", (0,0), (-1,-1), 3),
("LEFTPADDING", (0,0), (-1,-1), 5),
("RIGHTPADDING", (0,0), (-1,-1), 5),
("GRID", (0,0), (-1,-1), 0.4, colors.HexColor("#cccccc")),
("VALIGN", (0,0), (-1,-1), "MIDDLE"),
]
if zebra:
for i in range(header_rows, len(data)):
if i % 2 == 0:
style.append(("BACKGROUND", (0,i), (-1,i), C_GREY))
t.setStyle(TableStyle(style))
return t
# ── page background callback ─────────────────────────────────────────────────
def page_bg(canvas, doc):
canvas.saveState()
# header band
canvas.setFillColor(C_NAVY)
canvas.rect(0, H - 28*mm, W, 28*mm, fill=1, stroke=0)
# footer
canvas.setFillColor(colors.HexColor("#e8edf2"))
canvas.rect(0, 0, W, 10*mm, fill=1, stroke=0)
canvas.setFillColor(C_NAVY)
canvas.setFont("Helvetica", 7)
canvas.drawCentredString(W/2, 3.5*mm,
"Insulin Quick-Reference Card | For clinical use by trained healthcare professionals | "
"Always verify doses before administering | Page %d" % doc.page)
canvas.restoreState()
# ── document ─────────────────────────────────────────────────────────────────
doc = SimpleDocTemplate(
OUTPUT,
pagesize=A4,
topMargin=32*mm,
bottomMargin=14*mm,
leftMargin=15*mm,
rightMargin=15*mm,
title="Insulin Quick-Reference Card",
author="Orris Medical AI",
)
story = []
sp = lambda n=3: Spacer(1, n)
# ═══════════════════════════════════════════════════════════════════
# PAGE-HEADER OVERLAY (drawn via page_bg; add title content here)
# We place the title as first "story" elements that sit visually
# inside the nav band via top-margin alignment.
# ═══════════════════════════════════════════════════════════════════
# Title block (drawn on top of navy band via negative space trick)
# ReportLab doesn't do overlays easily, so we embed title in the
# first table styled with a navy background that bleeds to margin.
title_data = [[
Paragraph("INSULIN QUICK-REFERENCE CARD", sTitle),
Paragraph("Dosing Formulas · Types · Sliding Scale · DKA Protocol", sSub),
]]
# Two-row header block
header_block = Table([
[Paragraph("INSULIN QUICK-REFERENCE CARD", sTitle)],
[Paragraph("Dosing Formulas · Insulin Types · Sliding Scales · DKA/HHS Protocol · Glucose Targets", sSub)],
], colWidths=[W - 30*mm])
header_block.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), C_NAVY),
("TOPPADDING", (0,0), (-1,-1), 6),
("BOTTOMPADDING", (0,0), (-1,-1), 6),
("LEFTPADDING", (0,0), (-1,-1), 4),
("RIGHTPADDING", (0,0), (-1,-1), 4),
]))
story.append(header_block)
story.append(sp(6))
# ═══════════════════════════════════════════════════════════════════
# SECTION 1 — DIAGNOSIS & HbA1c
# ═══════════════════════════════════════════════════════════════════
story.append(section_header("1. DIAGNOSIS OF DIABETES (ADA 2024)"))
story.append(sp(4))
diag_data = [
[Paragraph("<b>Test</b>", sWht),
Paragraph("<b>Normal</b>", sWht),
Paragraph("<b>Prediabetes</b>", sWht),
Paragraph("<b>DIABETES</b>", sWht)],
["Fasting Plasma Glucose (8 h fast)",
"< 100 mg/dL", "100–125 mg/dL",
Paragraph("<b>≥ 126 mg/dL</b>", sBold)],
["2-h OGTT (75 g glucose)",
"< 140 mg/dL", "140–199 mg/dL",
Paragraph("<b>≥ 200 mg/dL</b>", sBold)],
["HbA1c",
"< 5.7%", "5.7–6.4%",
Paragraph("<b>≥ 6.5%</b>", sBold)],
["Random Glucose + symptoms",
"—", "—",
Paragraph("<b>≥ 200 mg/dL</b>", sBold)],
]
story.append(std_table(diag_data, [70*mm, 35*mm, 38*mm, 35*mm]))
story.append(sp(4))
story.append(Paragraph(
"Confirm on a <b>separate day</b> (except symptomatic hyperglycaemic crisis). "
"HbA1c unreliable in haemolytic anaemia, haemoglobinopathies, or recent transfusion.",
sNote))
story.append(sp(4))
# HbA1c ↔ Average Glucose
story.append(Paragraph("HbA1c → Estimated Average Glucose (eAG)", sH2))
hba1c_data = [
[Paragraph("<b>HbA1c %</b>", sWht),
Paragraph("<b>eAG mg/dL</b>", sWht),
Paragraph("<b>Interpretation</b>", sWht),
Paragraph("<b>HbA1c %</b>", sWht),
Paragraph("<b>eAG mg/dL</b>", sWht),
Paragraph("<b>Interpretation</b>", sWht)],
["5.7", "117", "Prediabetes threshold",
"8.0", "183", "Suboptimal"],
["6.0", "126", "Upper prediabetes",
"9.0", "212", "Poor control"],
["6.5", "140", "Diagnosis threshold",
"10.0", "240", "Very poor"],
[Paragraph("<b>7.0</b>", sBold), Paragraph("<b>154</b>", sBold),
Paragraph("<b>Treatment TARGET</b>", sBold),
"12.0+", "298+", "DKA / HHS risk"],
]
story.append(std_table(hba1c_data,
[18*mm, 22*mm, 37*mm, 18*mm, 22*mm, 37*mm]))
story.append(sp(6))
# ═══════════════════════════════════════════════════════════════════
# SECTION 2 — INSULIN TYPES
# ═══════════════════════════════════════════════════════════════════
story.append(section_header("2. INSULIN TYPES AT A GLANCE"))
story.append(sp(4))
ins_data = [
[Paragraph("<b>Type</b>", sWht),
Paragraph("<b>Examples</b>", sWht),
Paragraph("<b>Onset</b>", sWht),
Paragraph("<b>Peak</b>", sWht),
Paragraph("<b>Duration</b>", sWht),
Paragraph("<b>Clinical Use</b>", sWht)],
[Paragraph("<b>Rapid-acting</b>", sBold),
"Lispro, Aspart, Glulisine",
"5–15 min", "30–90 min", "3–5 h",
"Meal bolus; give with/just before meal"],
[Paragraph("<b>Short-acting</b>", sBold),
"Regular (Actrapid)",
"30–60 min", "2–4 h", "6–8 h",
"Sliding scale SC; IV infusion DKA/ICU"],
[Paragraph("<b>Intermediate</b>", sBold),
"NPH (Insulatard)",
"1–2 h", "4–8 h", "12–16 h",
"BD regimen; steroid-induced hyperglycaemia"],
[Paragraph("<b>Long-acting (Basal)</b>", sBold),
"Glargine (Lantus), Detemir",
"2–4 h", "No peak", "20–24 h",
"Once-daily basal; Glargine → same time daily"],
[Paragraph("<b>Ultra-long</b>", sBold),
"Degludec (Tresiba)",
"2 h", "No peak", "> 42 h",
"Flexible timing; lowest hypoglycaemia risk"],
[Paragraph("<b>Pre-mixed</b>", sBold),
"30/70, Novomix 30",
"Variable", "Dual", "12–16 h",
"BD convenience; less flexible; avoid T1DM"],
]
story.append(std_table(ins_data,
[28*mm, 35*mm, 16*mm, 16*mm, 16*mm, 49*mm]))
story.append(sp(4))
story.append(amber_box(
"⚠ NEVER mix Glargine with other insulins. "
"Rapid-acting analogue is PREFERRED over Regular for meal-time bolus (faster, safer)."))
story.append(sp(8))
# ═══════════════════════════════════════════════════════════════════
# SECTION 3 — DOSING FORMULAS
# ═══════════════════════════════════════════════════════════════════
story.append(section_header("3. INSULIN DOSING FORMULAS"))
story.append(sp(5))
story.append(Paragraph("Step 1 — Total Daily Dose (TDD)", sH2))
story.append(formula_box(
"TDD = 0.4–0.5 units/kg/day "
"│ Obese/Stress: 0.6–0.8 u/kg "
"│ Elderly/CKD/Thin: 0.2–0.3 u/kg"))
story.append(sp(3))
tdd_data = [
[Paragraph("<b>Weight (kg)</b>", sWht),
Paragraph("<b>Conservative TDD (0.4)</b>", sWht),
Paragraph("<b>Standard TDD (0.5)</b>", sWht),
Paragraph("<b>Aggressive TDD (0.6)</b>", sWht),
Paragraph("<b>Use case</b>", sWht)],
["50 kg", "20 units", "25 units", "30 units", "Elderly / low risk"],
["60 kg", "24 units", "30 units", "36 units", "Thin / CKD"],
["70 kg", "28 units", "35 units", "42 units", Paragraph("<b>Standard adult</b>", sBold)],
["80 kg", "32 units", "40 units", "48 units", "Typical adult"],
["90 kg", "36 units", "45 units", "54 units", "Overweight"],
["100 kg","40 units", "50 units", "60 units", "Obese / steroids"],
]
story.append(std_table(tdd_data, [28*mm, 38*mm, 38*mm, 38*mm, 33*mm]))
story.append(sp(6))
story.append(Paragraph("Step 2 — Split TDD into Basal + Bolus", sH2))
story.append(formula_box(
"BASAL = 50% of TDD → Glargine SC once daily (bedtime) │ "
"BOLUS = 50% of TDD ÷ 3 → Rapid-acting SC with each meal"))
story.append(sp(3))
example_data = [
[Paragraph("<b>Example: 70 kg patient, TDD = 35 units</b>", sWht), "", ""],
[Paragraph("<b>Component</b>", sWht),
Paragraph("<b>Dose</b>", sWht),
Paragraph("<b>Timing</b>", sWht)],
["Glargine (Basal)", "17–18 units SC", "10 PM daily (fixed time)"],
["Aspart / Lispro (Breakfast)", "5–6 units SC", "Within 15 min before meal"],
["Aspart / Lispro (Lunch)", "5–6 units SC", "Within 15 min before meal"],
["Aspart / Lispro (Dinner)", "5–6 units SC", "Within 15 min before meal"],
]
example_t = Table(example_data, colWidths=[55*mm, 40*mm, 65*mm])
example_t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), C_TEAL),
("SPAN", (0,0), (-1,0)),
("BACKGROUND", (0,1), (-1,1), C_NAVY),
("TEXTCOLOR", (0,0), (-1,1), C_WHITE),
("FONTNAME", (0,0), (-1,1), "Helvetica-Bold"),
("FONTSIZE", (0,0), (-1,-1), 7.5),
("BACKGROUND", (0,3), (-1,3), C_GREY),
("BACKGROUND", (0,5), (-1,5), C_GREY),
("GRID", (0,0), (-1,-1), 0.4, colors.HexColor("#cccccc")),
("TOPPADDING", (0,0), (-1,-1), 3),
("BOTTOMPADDING", (0,0), (-1,-1), 3),
("LEFTPADDING", (0,0), (-1,-1), 5),
("RIGHTPADDING", (0,0), (-1,-1), 5),
("VALIGN", (0,0), (-1,-1), "MIDDLE"),
]))
story.append(example_t)
story.append(sp(6))
story.append(Paragraph("Step 3 — Insulin Sensitivity Factor (ISF) & Correction Dose", sH2))
story.append(formula_box(
"ISF = 1800 ÷ TDD (Regular insulin) │ 1700 ÷ TDD (Rapid-acting)"))
story.append(sp(3))
story.append(formula_box(
"CORRECTION DOSE = (Actual Glucose − Target Glucose) ÷ ISF"))
story.append(sp(3))
isf_data = [
[Paragraph("<b>TDD (units)</b>", sWht),
Paragraph("<b>ISF (mg/dL per unit)</b>", sWht),
Paragraph("<b>Example: Glucose 280, Target 120</b>", sWht),
Paragraph("<b>Correction Dose</b>", sWht)],
["20", "90", "(280-120) ÷ 90 = 1.8", "→ 2 units"],
["28", "64", "(280-120) ÷ 64 = 2.5", "→ 2–3 units"],
["35", "51", "(280-120) ÷ 51 = 3.1", "→ 3 units"],
["50", "36", "(280-120) ÷ 36 = 4.4", "→ 4 units"],
["70", "26", "(280-120) ÷ 26 = 6.2", "→ 6 units"],
]
story.append(std_table(isf_data, [28*mm, 40*mm, 70*mm, 30*mm]))
story.append(sp(4))
story.append(Paragraph("Step 4 — Insulin-to-Carbohydrate Ratio (ICR)", sH2))
story.append(formula_box(
"ICR = 500 ÷ TDD → 1 unit covers X grams of carbohydrate"))
story.append(sp(3))
story.append(Paragraph(
"Example: TDD = 35 → ICR = 500 ÷ 35 = 14 g/unit. "
"If patient eats 56 g carbs: 56 ÷ 14 = <b>4 units pre-meal bolus.</b>", sBody))
story.append(sp(4))
story.append(Paragraph("Glargine Titration — '3-3-3' Rule", sH2))
story.append(green_box(
"✓ Check fasting glucose for 3 days. "
"If fasting > 130 mg/dL on 3 consecutive mornings → INCREASE Glargine by 2 units. "
"If fasting < 70 mg/dL → DECREASE Glargine by 10–20%. "
"Target fasting: 80–130 mg/dL."))
story.append(sp(8))
# ═══════════════════════════════════════════════════════════════════
# SECTION 4 — SLIDING SCALE
# ═══════════════════════════════════════════════════════════════════
story.append(section_header("4. INPATIENT SLIDING SCALE (Supplemental / Correction Insulin)"))
story.append(sp(4))
story.append(Paragraph(
"Use RAPID-ACTING (Aspart / Lispro) or REGULAR (Actrapid) SC. "
"Sliding scale alone is inadequate — always combine with scheduled BASAL insulin.", sNote))
story.append(sp(3))
# Two-column layout: Low scale | High scale
low_scale = [
[Paragraph("<b>LOW SCALE</b> (Elderly / CKD / Thin / Hypoglycaemia-prone)", sWht), ""],
[Paragraph("<b>Glucose (mg/dL)</b>", sWht),
Paragraph("<b>Dose (SC)</b>", sWht)],
[Paragraph("< 70", sAlert),
Paragraph("HOLD all insulin → Treat hypoglycaemia", sAlert)],
["70–150", "0 units"],
["151–200", "1 unit"],
["201–250", "2 units"],
["251–300", "3 units"],
["301–350", "4 units"],
["351–400", "5 units"],
[Paragraph("> 400", sAlert), Paragraph("6 units + CALL DOCTOR", sAlert)],
]
high_scale = [
[Paragraph("<b>HIGH SCALE</b> (Obese / Steroids / ICU / High insulin resistance)", sWht), ""],
[Paragraph("<b>Glucose (mg/dL)</b>", sWht),
Paragraph("<b>Dose (SC)</b>", sWht)],
[Paragraph("< 70", sAlert),
Paragraph("HOLD all insulin → Treat hypoglycaemia", sAlert)],
["70–150", "0 units"],
["151–200", "4 units"],
["201–250", "6 units"],
["251–300", "8 units"],
["301–350", "10 units"],
["351–400", "12 units"],
[Paragraph("> 400", sAlert), Paragraph("14 units + CALL DOCTOR", sAlert)],
]
def scale_table(data):
t = Table(data, colWidths=[38*mm, 42*mm])
style = [
("BACKGROUND", (0,0), (-1,0), C_TEAL),
("SPAN", (0,0), (-1,0)),
("BACKGROUND", (0,1), (-1,1), C_NAVY),
("TEXTCOLOR", (0,0), (-1,1), C_WHITE),
("FONTNAME", (0,0), (-1,1), "Helvetica-Bold"),
("FONTSIZE", (0,0), (-1,-1), 7.5),
("BACKGROUND", (0,2), (-1,2), C_LRED),
("BACKGROUND", (0,-1),(-1,-1),C_LRED),
("GRID", (0,0), (-1,-1), 0.4, colors.HexColor("#cccccc")),
("TOPPADDING", (0,0), (-1,-1), 3),
("BOTTOMPADDING", (0,0), (-1,-1), 3),
("LEFTPADDING", (0,0), (-1,-1), 5),
("RIGHTPADDING", (0,0), (-1,-1), 5),
("VALIGN", (0,0), (-1,-1), "MIDDLE"),
("ROWBACKGROUNDS", (0,3), (-1,-2), [C_WHITE, C_GREY]),
]
t.setStyle(TableStyle(style))
return t
dual_scales = Table(
[[scale_table(low_scale), Spacer(6, 1), scale_table(high_scale)]],
colWidths=[82*mm, 6*mm, 82*mm]
)
story.append(dual_scales)
story.append(sp(4))
story.append(amber_box(
"STANDARD SCALE (General Ward): Add 2 units to Low Scale values above for most adult patients. "
"Reassess scale intensity daily. Goal: 70–180 mg/dL."))
story.append(sp(8))
# ═══════════════════════════════════════════════════════════════════
# SECTION 5 — GLUCOSE TARGETS
# ═══════════════════════════════════════════════════════════════════
story.append(section_header("5. GLUCOSE TARGETS BY CLINICAL SETTING"))
story.append(sp(4))
tgt_data = [
[Paragraph("<b>Setting</b>", sWht),
Paragraph("<b>Pre-meal Target</b>", sWht),
Paragraph("<b>Post-meal / Random</b>", sWht),
Paragraph("<b>HbA1c Target</b>", sWht),
Paragraph("<b>Key Notes</b>", sWht)],
["OPD — Young/Healthy T2DM",
"80–130 mg/dL", "< 180 mg/dL", Paragraph("<b>< 7.0%</b>", sBold),
"Strict; no hypoglycaemia"],
["OPD — Elderly / Frail / CVD",
"100–150 mg/dL", "< 200 mg/dL", "< 8.0–8.5%",
"Avoid hypoglycaemia (fall risk)"],
[Paragraph("<b>Pregnancy (GDM)</b>", sBold),
"< 95 mg/dL", "1 h: < 140 / 2 h: < 120", "< 6.0–6.5%",
"Tightest targets; monitor closely"],
["Non-ICU Ward",
"100–140 mg/dL", "140–180 mg/dL", "Per pre-admission",
"Hold metformin during acute illness"],
[Paragraph("<b>ICU (General / Post-op)</b>", sBold),
"—", Paragraph("<b>140–180 mg/dL</b>", sBold), "—",
"NICE-SUGAR: tight control (80-110) → ↑ mortality"],
["ICU — Cardiac Surgery",
"—", "140–180 mg/dL", "—",
"Insulin infusion preferred; avoid < 110"],
["DKA — Active phase",
"—", "250–300 (don't drop fast)", "—",
"When < 250 → add D5 to IVF; keep insulin running"],
]
story.append(std_table(tgt_data, [38*mm, 28*mm, 36*mm, 22*mm, 46*mm]))
story.append(sp(8))
# ═══════════════════════════════════════════════════════════════════
# SECTION 6 — DKA PROTOCOL
# ═══════════════════════════════════════════════════════════════════
story.append(section_header("6. DKA / HHS EMERGENCY PROTOCOL"))
story.append(sp(4))
# DKA vs HHS comparison
comp_data = [
[Paragraph("<b>Feature</b>", sWht),
Paragraph("<b>DKA</b>", sWht),
Paragraph("<b>HHS</b>", sWht)],
["Typical patient", "T1DM (any age)", "T2DM — elderly"],
["Glucose",
Paragraph("<b>250–600 mg/dL</b>", sBold),
Paragraph("<b>> 600 mg/dL</b>", sBold)],
["pH",
Paragraph("<b>< 7.3 (acidotic)</b>", sAlert),
"> 7.3 (near normal)"],
["HCO3", "< 18 mEq/L", "Normal (> 18)"],
["Ketones", "+++ (blood > 3 mmol/L)", "Absent / trace"],
["Osmolality", "< 320 mOsm/kg", Paragraph("<b>> 320 mOsm/kg</b>", sBold)],
["Anion gap", "> 12 (HAGMA)", "Normal"],
["Primary Rx",
Paragraph("<b>Insulin + Fluids</b>", sBold),
Paragraph("<b>FLUIDS first, then insulin</b>", sBold)],
["Mortality", "< 5%", Paragraph("<b>8–25%</b>", sAlert)],
]
story.append(std_table(comp_data, [38*mm, 62*mm, 62*mm]))
story.append(sp(5))
story.append(Paragraph("DKA Management — Phase Sequence", sH2))
phases_data = [
[Paragraph("<b>Phase</b>", sWht),
Paragraph("<b>Action</b>", sWht),
Paragraph("<b>Detail / Dose</b>", sWht)],
[Paragraph("<b>1 — FLUIDS</b>\n(start immediately)", sBold),
"0.9% Normal Saline IV",
"Hour 1–2: 1 L/h → Hours 3–4: 500 mL/h → Hours 5–12: 250 mL/h\n"
"Total 24 h: 5–8 L. When glucose < 250: switch to D5% in 0.45% NaCl"],
[Paragraph("<b>2 — POTASSIUM</b>\n(before insulin!)", sBold),
"KCl replacement",
"K+ < 3.5: Give KCl 20–40 mEq/h IV for 1–2 h BEFORE starting insulin\n"
"K+ 3.5–5.5: Add KCl 20 mEq/L to each IV bag\n"
"K+ > 5.5: Start insulin; recheck K+ in 1 h. Target K+: 3.5–5.0"],
[Paragraph("<b>3 — INSULIN</b>\n(after 1 L fluid + K+>3.5)", sBold),
"Regular Insulin IV infusion",
"Bolus: 0.1 u/kg IV push, THEN\n"
"Infusion: 0.1 u/kg/h (50 units in 50 mL NS = 1 u/mL via syringe pump)\n"
"Target: glucose falls 50–75 mg/dL/h\n"
"When glucose < 250: reduce to 0.02–0.05 u/kg/h; add dextrose to IVF"],
[Paragraph("<b>4 — BICARBONATE</b>\n(only if severe)", sBold),
"NaHCO3 100 mEq in 400 mL\nsterile water over 2 h",
"ONLY if pH < 7.1. Risk: hypokalaemia, cerebral oedema.\n"
"Do NOT give routinely. Recheck pH after 2 h."],
[Paragraph("<b>5 — TRANSITION\nto SC Insulin</b>", sBold),
"Resolution criteria (ALL 3):",
"Glucose < 200 AND HCO3 ≥ 18 AND pH > 7.3 AND Anion gap ≤ 12\n"
"Give Glargine SC (80% prior TDD) AT LEAST 2–4 h BEFORE stopping IV insulin"],
]
phases_t = Table(phases_data, colWidths=[33*mm, 45*mm, 88*mm])
phases_t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), C_NAVY),
("TEXTCOLOR", (0,0), (-1,0), C_WHITE),
("FONTNAME", (0,0), (-1,0), "Helvetica-Bold"),
("FONTSIZE", (0,0), (-1,-1), 7.5),
("VALIGN", (0,0), (-1,-1), "TOP"),
("TOPPADDING", (0,0), (-1,-1), 4),
("BOTTOMPADDING", (0,0), (-1,-1), 4),
("LEFTPADDING", (0,0), (-1,-1), 5),
("RIGHTPADDING", (0,0), (-1,-1), 5),
("GRID", (0,0), (-1,-1), 0.4, colors.HexColor("#cccccc")),
("BACKGROUND", (0,1), (0,1), C_LTBL),
("BACKGROUND", (0,2), (0,2), C_AMBER2),
("BACKGROUND", (0,3), (0,3), C_LRED),
("BACKGROUND", (0,4), (0,4), C_AMBER2),
("BACKGROUND", (0,5), (0,5), C_LGRN),
]))
story.append(phases_t)
story.append(sp(5))
# DKA monitoring table
story.append(Paragraph("DKA Monitoring Frequency", sH2))
mon_data = [
[Paragraph("<b>Parameter</b>", sWht),
Paragraph("<b>Frequency</b>", sWht),
Paragraph("<b>Target</b>", sWht)],
["Capillary glucose", "Every 1 h", "Fall 50–75 mg/dL/h; < 200 for transition"],
["Serum K+", "Every 2 h", "3.5–5.0 mEq/L (CRITICAL)"],
["VBG / ABG", "Every 2 h", "pH > 7.3; HCO3 > 18"],
["Anion gap", "Every 4 h", "≤ 12 mEq/L (DKA resolved)"],
["Urine output", "Continuous (IDC)", "> 0.5 mL/kg/h"],
["ECG", "Continuous", "Watch for hypokalaemia changes (flat T, U waves)"],
["Neuro / GCS", "Every 1 h", "GCS improving; watch for cerebral oedema"],
]
story.append(std_table(mon_data, [40*mm, 38*mm, 88*mm]))
story.append(sp(4))
story.append(red_box(
"⚠ CRITICAL RULE: Check K+ BEFORE starting insulin. "
"If K+ < 3.5 → HOLD insulin → replace K+ first. "
"Insulin drives K+ into cells → fatal hypokalaemia if not corrected first."))
story.append(sp(8))
# ═══════════════════════════════════════════════════════════════════
# SECTION 7 — SPECIAL SITUATIONS
# ═══════════════════════════════════════════════════════════════════
story.append(section_header("7. SPECIAL CLINICAL SITUATIONS"))
story.append(sp(4))
spec_data = [
[Paragraph("<b>Situation</b>", sWht),
Paragraph("<b>Insulin Adjustment</b>", sWht),
Paragraph("<b>Key Caution</b>", sWht)],
["NPO / Fasting (pre-op)",
"Give 50–75% of basal only; HOLD all bolus insulin",
"Resume bolus only when patient eating"],
["Renal failure (eGFR < 30)",
"Reduce TDD by 25–50%; monitor closely q4 h",
"Insulin cleared more slowly → accumulates → hypoglycaemia"],
["Liver failure",
"Reduce TDD by 25%; hypoglycaemia common",
"Reduced gluconeogenesis → unpredictable glucose"],
["Steroid-induced (prednisolone OD)",
"NPH morning or ↑ afternoon bolus; peak 4–8 h post-dose",
"Glucose rises in afternoon; fasting glucose may be normal"],
["Sick day (T1DM)",
"NEVER stop insulin; check ketones q4 h if glucose > 300",
"Even if not eating: reduce bolus; maintain basal fully"],
["ICU → SC transition",
"80% of 24 h IV insulin used = SC TDD; basal 50% + bolus 50%",
"Give SC 2–4 h BEFORE stopping IV infusion (lag time!)"],
["Pregnancy (GDM/T1DM)",
"Insulin requirements ↑ 2–3× in T3; monitor more frequently",
"Avoid oral agents except Metformin (insulin preferred)"],
["Post-bariatric surgery",
"Significant reduction often possible; may need to ↓ TDD 50–80%",
"Risk of late dumping / reactive hypoglycaemia; check glucose 1 h post-meal"],
]
story.append(std_table(spec_data, [40*mm, 65*mm, 60*mm]))
story.append(sp(8))
# ═══════════════════════════════════════════════════════════════════
# SECTION 8 — T2DM DRUG LADDER
# ═══════════════════════════════════════════════════════════════════
story.append(section_header("8. T2DM ORAL DRUG LADDER (ADA 2024 Algorithm)"))
story.append(sp(4))
ladder_data = [
[Paragraph("<b>Step</b>", sWht),
Paragraph("<b>Drug / Class</b>", sWht),
Paragraph("<b>Dose</b>", sWht),
Paragraph("<b>HbA1c ↓</b>", sWht),
Paragraph("<b>Weight</b>", sWht),
Paragraph("<b>Hypo Risk</b>", sWht),
Paragraph("<b>Key Indication / Caution</b>", sWht)],
[Paragraph("<b>1</b>", sBold), "Metformin",
"500–2000 mg BID", "1.0–1.5%", "Neutral", "None",
"First-line always; avoid eGFR < 30, contrast, acute illness"],
[Paragraph("<b>2A</b>\n(CVD)", sBold),
"GLP-1 RA (Semaglutide, Liraglutide)",
"Sema: 0.25→1 mg SC/wk", "1.5–2.0%",
Paragraph("<b>↓↓ 5–15 kg</b>", sGreen), "None",
"CV mortality ↓ (LEADER, SUSTAIN-6); avoid MEN2/thyroid Ca"],
[Paragraph("<b>2B</b>\n(HF/CKD)", sBold),
"SGLT-2i (Empagliflozin, Dapagliflozin)",
"Empa 10–25 mg OD", "0.7–1.0%",
Paragraph("<b>↓ 2–3 kg</b>", sGreen), "None",
"HF hospitalisation ↓, CKD progression ↓; avoid eGFR < 30"],
[Paragraph("<b>2C</b>\n(Cost)", sBold),
"Sulfonylurea (Gliclazide MR)",
"30–120 mg OD morning", "1.5–2.0%",
Paragraph("<b>↑ 2 kg</b>", sAlert), Paragraph("<b>HIGH</b>", sAlert),
"Cheapest; avoid glibenclamide in elderly/CKD"],
[Paragraph("<b>2D</b>\n(Safe)", sBold),
"DPP-4i (Sitagliptin, Vildagliptin)",
"Sita 100 mg OD", "0.5–0.8%", "Neutral", "None",
"Well tolerated; dose-reduce in CKD; avoid saxagliptin in HF"],
[Paragraph("<b>3</b>", sBold),
"Add 3rd agent or Basal Insulin",
"Glargine 0.1–0.2 u/kg hs", "3–4%+",
Paragraph("<b>↑</b>", sAlert), Paragraph("<b>YES</b>", sAlert),
"If HbA1c > 9%: start basal insulin + continue Metformin"],
]
story.append(std_table(ladder_data,
[14*mm, 36*mm, 28*mm, 16*mm, 16*mm, 16*mm, 50*mm]))
story.append(sp(4))
story.append(amber_box(
"STOP Sulfonylurea when starting insulin (double hypoglycaemia risk). "
"CONTINUE Metformin with insulin (reduces insulin dose by ~30%). "
"HOLD SGLT-2i 3–4 days before major surgery (euglycaemic DKA risk)."))
story.append(sp(8))
# ═══════════════════════════════════════════════════════════════════
# SECTION 9 — HYPOGLYCAEMIA MANAGEMENT
# ═══════════════════════════════════════════════════════════════════
story.append(section_header("9. HYPOGLYCAEMIA RECOGNITION & MANAGEMENT"))
story.append(sp(4))
hypo_data = [
[Paragraph("<b>Severity</b>", sWht),
Paragraph("<b>Glucose</b>", sWht),
Paragraph("<b>Symptoms</b>", sWht),
Paragraph("<b>Treatment</b>", sWht)],
[Paragraph("<b>Level 1 (Alert)</b>", sBold),
"54–70 mg/dL",
"Sweating, tremor, anxiety, palpitations, hunger",
"15–20 g fast carbs PO (4 glucose tabs / 150 mL juice / 3 tsp sugar)\n"
"Recheck in 15 min; repeat if still < 70"],
[Paragraph("<b>Level 2 (Significant)</b>", sBold),
"< 54 mg/dL",
"Confusion, slurred speech, altered behaviour",
"Same as Level 1 if conscious\n"
"If impaired: Glucagon 1 mg IM/SC or D50W 25 mL IV"],
[Paragraph("<b>Level 3 (Severe)</b>", sBold),
"Any (with unconsciousness)",
"Seizure, unresponsive, coma",
"D50W 50 mL IV push IMMEDIATELY\n"
"Then D10% 100 mL/h infusion until glucose > 100 mg/dL\n"
"Glucagon 1 mg IM if no IV access\n"
"Recheck glucose q15 min × 4"],
]
hypo_t = Table(hypo_data, colWidths=[28*mm, 22*mm, 52*mm, 66*mm])
hypo_t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), C_NAVY),
("TEXTCOLOR", (0,0), (-1,0), C_WHITE),
("FONTNAME", (0,0), (-1,0), "Helvetica-Bold"),
("FONTSIZE", (0,0), (-1,-1), 7.5),
("VALIGN", (0,0), (-1,-1), "TOP"),
("TOPPADDING", (0,0), (-1,-1), 4),
("BOTTOMPADDING", (0,0), (-1,-1), 4),
("LEFTPADDING", (0,0), (-1,-1), 5),
("RIGHTPADDING", (0,0), (-1,-1), 5),
("GRID", (0,0), (-1,-1), 0.4, colors.HexColor("#cccccc")),
("BACKGROUND", (0,1), (-1,1), C_AMBER2),
("BACKGROUND", (0,2), (-1,2), colors.HexColor("#ffe4cc")),
("BACKGROUND", (0,3), (-1,3), C_LRED),
]))
story.append(hypo_t)
story.append(sp(4))
story.append(green_box(
"RULE OF 15: 15 g carbs → wait 15 min → recheck. If still < 70 → repeat. "
"After recovery: give 15–20 g long-acting carbs (bread / biscuits / milk). "
"Identify and address cause: excess insulin dose, missed meal, exercise, alcohol, renal failure."))
story.append(sp(8))
# ═══════════════════════════════════════════════════════════════════
# SECTION 10 — CLINICAL PEARLS
# ═══════════════════════════════════════════════════════════════════
story.append(section_header("10. CLINICAL PEARLS — MASTER LIST"))
story.append(sp(4))
pearls = [
("TDD Starting Dose",
"0.4 u/kg (conservative) to 0.5 u/kg (standard) to 0.6–0.8 u/kg (obese/ICU). "
"ALWAYS start low → titrate up every 3 days based on fasting glucose."),
("HbA1c & Anaemia",
"HbA1c is UNRELIABLE in haemolytic anaemia, iron-deficiency, haemoglobinopathies, "
"and after recent blood transfusion. Use fructosamine or eAG instead."),
("DKA: K+ before Insulin",
"ALWAYS check K+ before starting insulin. If K+ < 3.5 → replace first. "
"Insulin shifts K+ intracellularly → fatal arrhythmia if uncorrected."),
("DKA: Insulin Stops Ketogenesis",
"Goal of insulin in DKA is to STOP ketone production, NOT primarily to drop glucose. "
"When glucose < 250: add dextrose and KEEP insulin running until anion gap closes."),
("IV → SC Insulin Transition",
"Give SC Glargine (0.3–0.5 u/kg) at least 2–4 hours BEFORE stopping IV infusion. "
"SC insulin takes 2–4 h to become active. Skipping overlap = rebound DKA."),
("Metformin Rules",
"HOLD metformin: eGFR < 30, acute illness, contrast CT (hold 48 h before and after), "
"major surgery, heart failure (class III–IV), hepatic failure."),
("SGLT-2i Safety",
"HOLD 3–4 days before major surgery (euglycaemic DKA risk). Causes genital infections (~10%): "
"counsel hygiene. Contraindicated eGFR < 30. Benefits: HF hospitalisation ↓, CKD progression ↓."),
("ICU Glucose Target",
"Target 140–180 mg/dL in ICU (NICE-SUGAR trial, 2009). Tight control (80–110 mg/dL) "
"significantly INCREASES mortality in ICU patients. Avoid hypoglycaemia at all costs."),
("Steroid-Induced Hyperglycaemia",
"Glucose peaks 4–8 h post-dose. If on once-daily prednisolone in morning: "
"use NPH (Insulatard) in morning OR increase afternoon/dinner bolus. Fasting glucose may appear normal."),
("Never Stop Insulin — T1DM Sick Day",
"Even if T1DM patient is vomiting and not eating: NEVER stop insulin (may reduce to 50–75%). "
"Absence of insulin → DKA even without eating. Check ketones q4 h if glucose > 300."),
("GLP-1 Agonist Initiation",
"Start semaglutide SC at 0.25 mg/week × 4 weeks, then 0.5 mg/week. "
"Slow titration prevents nausea. Oral semaglutide: take 30 min before first food/drink of day "
"with ≤ 120 mL plain water ONLY."),
("Glargine Administration",
"Give at the SAME time each day (bedtime preferred). Cannot be mixed with any other insulin. "
"Clear solution (NOT milky — milky = NPH). Inject SC; do not inject IV."),
]
pearl_rows = []
for title, text in pearls:
pearl_rows.append([
Paragraph(f"<b>{title}</b>", sBold),
Paragraph(text, sBody)
])
pearl_t = Table(pearl_rows, colWidths=[40*mm, 125*mm])
pearl_style = [
("FONTSIZE", (0,0), (-1,-1), 7.5),
("TOPPADDING", (0,0), (-1,-1), 4),
("BOTTOMPADDING", (0,0), (-1,-1), 4),
("LEFTPADDING", (0,0), (-1,-1), 5),
("RIGHTPADDING", (0,0), (-1,-1), 5),
("VALIGN", (0,0), (-1,-1), "TOP"),
("GRID", (0,0), (-1,-1), 0.3, colors.HexColor("#dddddd")),
("BACKGROUND", (0,0), (0,-1), C_LTBL),
]
for i in range(0, len(pearl_rows), 2):
pearl_style.append(("BACKGROUND", (1,i), (1,i), C_WHITE))
if i+1 < len(pearl_rows):
pearl_style.append(("BACKGROUND", (1,i+1), (1,i+1), C_GREY))
pearl_t.setStyle(TableStyle(pearl_style))
story.append(pearl_t)
story.append(sp(6))
story.append(Paragraph(
"Sources: Rosen's Emergency Medicine · Miller's Anesthesia 10e · Harrison's Principles of "
"Internal Medicine 22e · Creasy & Resnik's Maternal-Fetal Medicine · "
"ADA Standards of Care 2024 · NICE-SUGAR Trial (NEJM 2009)",
sNote))
# ── build ────────────────────────────────────────────────────────────────────
doc.build(story, onFirstPage=page_bg, onLaterPages=page_bg)
print(f"PDF written to {OUTPUT}")
cd /home/daytona/workspace/insulin-ref && python3 build_pdf.py 2>&1
ls -lh /home/daytona/workspace/insulin-ref/Insulin_Quick_Reference.pdf
Insulin Quick Reference
PDF Document · PDF
What's inside the 10-section quick-reference card:
| Section | Content |
|---|---|
| 1. Diagnosis | ADA 2024 criteria table (FPG / OGTT / HbA1c / Random); HbA1c → eAG conversion table with interpretation |
| 2. Insulin Types | All 6 types with onset, peak, duration, and clinical use |
| 3. Dosing Formulas | TDD by weight table (50–100 kg); Basal/Bolus 50:50 split; ISF formula + worked example; ICR formula; Glargine 3-3-3 titration rule |
| 4. Sliding Scale | Two side-by-side scales - Low Scale (elderly/CKD) and High Scale (obese/steroids/ICU), both colour-coded with red alert rows |
| 5. Glucose Targets | OPD, elderly, pregnancy, non-ICU ward, ICU, cardiac surgery, DKA active phase |
| 6. DKA / HHS Protocol | DKA vs HHS comparison table; 5-phase DKA sequence (Fluids → K+ → Insulin → Bicarb → Transition); monitoring frequency table; red alert K+ rule |
| 7. Special Situations | NPO, renal failure, liver failure, steroids, sick-day rules, ICU transition, pregnancy, post-bariatric |
| 8. T2DM Drug Ladder | Step-by-step with doses, HbA1c reduction %, weight effect, hypoglycaemia risk, indications |
| 9. Hypoglycaemia | 3-level severity table with treatment for each; Rule of 15 |
| 10. Clinical Pearls | 12 key pearls covering TDD, DKA K+, ICU targets, metformin rules, SGLT-2i safety, glargine tips |
Create clinical case scenarios with dosing answers
mkdir -p /home/daytona/workspace/clinical-cases && python3 -c "from reportlab.lib.pagesizes import A4; print('ok')"
Create clinical case scenarios with dosing answers
mkdir -p /home/daytona/workspace/clinical-cases && ls /home/daytona/workspace/