laynngomalacia in detail for 20 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Searching PubMed
laryngomalacia management diagnosis
Finding Sources
Reading File
Reading File
Reading File
Searching PubMed
laryngomalacia supraglottoplasty outcomes
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Searching the Web
laryngomalacia Zakir Hussain Dhingra Hazarika textbook ENT classification grading
Finding Sources
Reading Article
PMID: 38219735
Finding Sources
Loading Image
LARYNGOMALACIA - Comprehensive 20-Mark Answer
(RGUHS Format | ENT Postgraduate)
DEFINITION
Laryngomalacia (also called congenital flaccid larynx) is the most common congenital anomaly of the larynx and the most frequent cause of inspiratory stridor in neonates and infants. It is characterized by partial or complete collapse of the supraglottic laryngeal structures during inspiration due to structural and/or neuromuscular immaturity.
- Cummings Otolaryngology, 6th ed. - "The most common cause of stridor during infancy is laryngomalacia."
- Scott-Brown's, Vol. 2 - "Laryngomalacia is characterized by partial or complete collapse of the supraglottic structures on inspiration and is the most common congenital cause of stridor."
INCIDENCE AND EPIDEMIOLOGY
- Accounts for approximately 75% of all cases of infantile stridor
- Premature infants, Hispanic and Black infants of all gestational ages are at higher risk
- Slight male predominance
- Rarely, may persist into older childhood, adolescence, or adulthood
ETIOPATHOGENESIS / THEORIES
Three main theories have been proposed:
1. Structural / Anatomical Theory (Historical - Sutherland & Lack, 1897)
- Immaturity and softness of the laryngeal cartilages
- Epiglottis is long, narrow, and tubular ("omega-shaped")
- Short, tightly tethered aryepiglottic folds tether the epiglottis posteriorly
- Redundant mucosa/submucosa over the arytenoids that prolapses on inspiration
- Deep interarytenoid cleft
2. Neuromuscular / Neurological Theory (Current Consensus)
- Dysfunction of the Laryngeal Adductor Reflex (LAR): a vagally mediated reflex activated by mechanoreceptors/chemoreceptors in the superior laryngeal nerve region of the aryepiglottic fold
- Sensorimotor integration dysfunction at the level of peripheral afferents, brainstem, or motor efferents leads to reduced laryngeal tone
- Infants with LM have elevated laryngopharyngeal sensory thresholds (altered sensorimotor integration)
- Pathological specimens show submucosal nerve hypertrophy compared to controls
- Associated with neurologic comorbidities (cerebral palsy, hypotonia)
3. Gastroesophageal Reflux (GER) Theory
- GER is found in the majority of patients with laryngomalacia
- The increased work of breathing generates high negative intrathoracic pressure, which promotes reflux - creating a self-perpetuating cycle
- Children with reflux have more severe laryngomalacia requiring surgical intervention
- Scott-Brown's Vol. 2: "Surgical treatment of laryngomalacia tends to reduce the severity of reflux if present pre-operatively."
Flowchart 1 - Pathophysiology
Structural Immaturity Neuromuscular Hypotonia
(Omega epiglottis, short AE (LAR dysfunction, elevated
folds, redundant arytenoid sensory thresholds, nerve
mucosa) hypertrophy)
↓ ↓
↘ ↙
SUPRAGLOTTIC COLLAPSE ON INSPIRATION
↓
↑ Negative intrathoracic pressure
↓
Promotes Gastroesophageal Reflux
↓
Mucosal edema → Worsens collapse
↓
Self-perpetuating cycle
ENDOSCOPIC ANATOMICAL FINDINGS (CLASSIFIED BY HOLINGER/SHAH)
┌─────────────────────────────────────────────────────────┐
│ CLASSIFICATION (Cummings / Shah & Wetmore) │
├──────────┬──────────────────────────────────────────────┤
│ TYPE 1 │ Short/foreshortened aryepiglottic folds │
│ │ tether epiglottis posteriorly (15%) │
├──────────┼──────────────────────────────────────────────┤
│ TYPE 2 │ Anterior prolapse of mucosa overlying │
│ │ arytenoid cartilages - most common (57%) │
├──────────┼──────────────────────────────────────────────┤
│ TYPE 3 │ Posterior collapse of epiglottis (12%) │
│ │ - associated with neuromuscular disorders │
├──────────┼──────────────────────────────────────────────┤
│ MIXED │ Combination of above (15%) │
└──────────┴──────────────────────────────────────────────┘
(K.J. Lee's Essential Otolaryngology, 9th ed.)
ENDOSCOPIC IMAGES FROM TEXTBOOKS
Fig. 1 - Laryngomalacia: Progressive airway obstruction on inspiration showing omega-shaped epiglottis (Cummings Otolaryngology, Fig. 206.2)
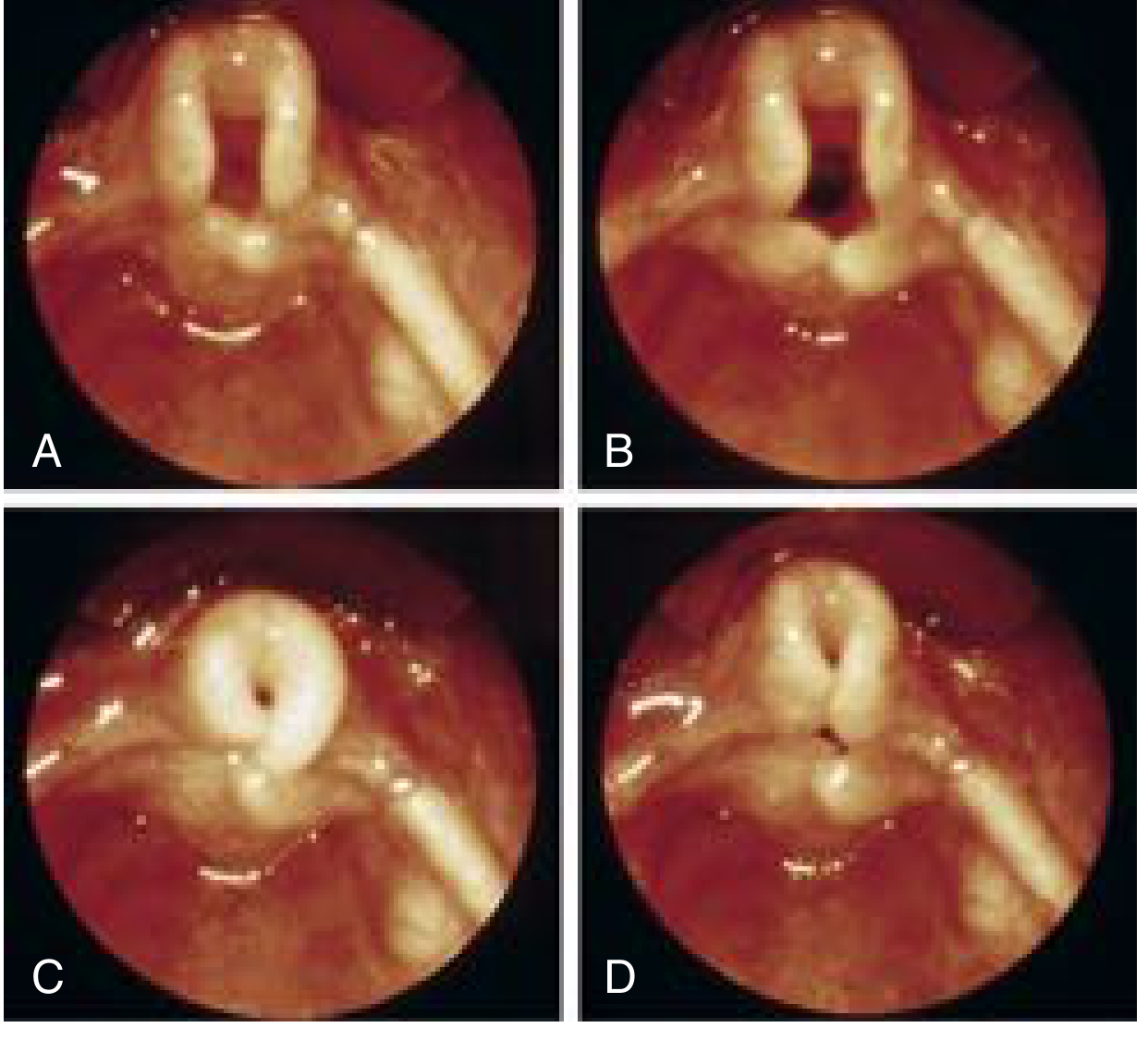
Fig. 2 - Laryngomalacia: Omega-shaped epiglottis (Scott-Brown's, Fig. 30.1)
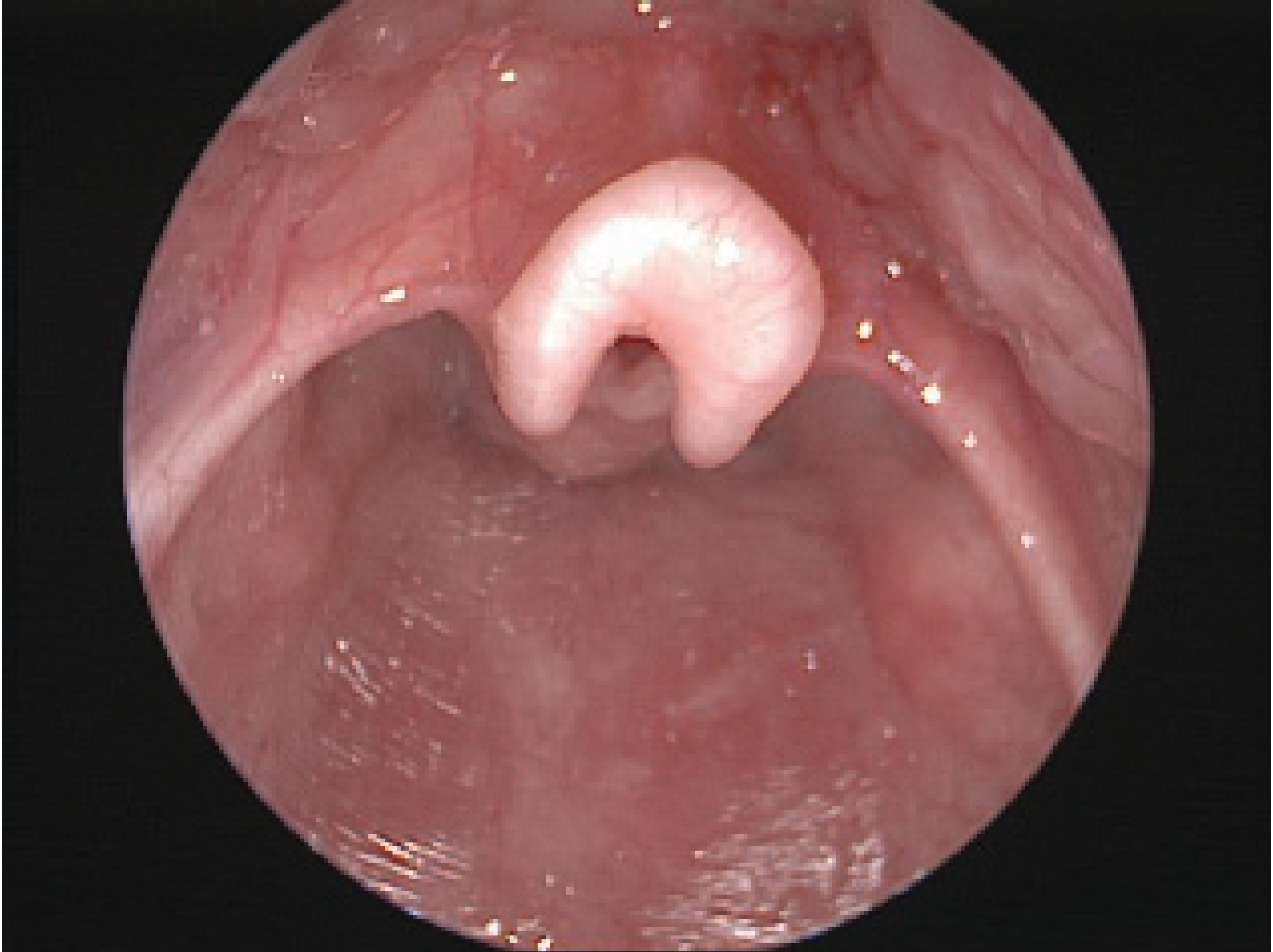
Fig. 3 - Laryngomalacia with arytenoid redundancy and prolapse into glottis on inspiration (Scott-Brown's, Fig. 44.9)

Fig. 4 - Infant larynx Before (A) and After (B) supraglottoplasty (Cummings Otolaryngology, Fig. 206.3)

CLINICAL FEATURES
Symptoms
| Feature | Detail |
|---|---|
| Stridor | High-pitched, fluttering, inspiratory; present within first 2 weeks of life |
| Timing | Worsens with activity/feeding, improves with sleep and mild LM improves with crying |
| Severe LM | Worsens with crying (increased airflow through collapsed larynx) |
| Feeding difficulties | Pauses during feeds to breathe; coughing, choking, regurgitation |
| Position | Better in prone; worse in supine |
| GER | Often concurrent; reflux symptoms |
Signs in Severe Cases
- Sternal and intercostal recession
- Failure to thrive
- Apnea episodes
- Pectus excavatum
- Cyanosis
- Cor pulmonale (late, if untreated)
Natural History
- Stridor typically begins within the first 2 weeks of life
- Severity increases as the infant becomes more active (up to 9 months)
- Median resolution: 7-9 months of age
- Vast majority resolve by 18 months; nearly all by 2 years
- Scott-Brown's: "Very rarely, stridor may persist into late childhood."
DIAGNOSIS
Flowchart 2 - Diagnostic Algorithm
Infant with Inspiratory Stridor
↓
History + Clinical examination
↓
┌───────────────────────────────────────┐
│ Awake Flexible Fibreoptic │
│ Nasopharyngoscopy (clinic) │
└───────────────────────────────────────┘
↓
┌──────────────────────────────────────────────────┐
│ Classic findings: │
│ • Omega-shaped epiglottis │
│ • Short aryepiglottic folds │
│ • Anterior prolapse of arytenoid mucosa │
│ • Supraglottic collapse on inspiration │
│ • Normal vocal fold mobility │
└──────────────────────────────────────────────────┘
↓
┌──────────────────────────────────────────────────┐
│ MILD (90% of cases) │
│ No further investigation; reassure parents │
└──────────────────────────────────────────────────┘
OR
┌──────────────────────────────────────────────────┐
│ SEVERE / atypical / failure to thrive / │
│ Cyanosis / suspected synchronous lesions │
└──────────────────────────────────────────────────┘
↓
┌──────────────────────────────────────────────────┐
│ Microlaryngoscopy + Bronchoscopy (MLB) under │
│ GA (SPONTANEOUS BREATHING, very light │
│ anaesthesia; laryngoscope beak in vallecula) │
└──────────────────────────────────────────────────┘
↓
Additional investigations as needed:
• GERD workup (pH-impedance study, barium swallow)
• Neurological evaluation
• Polysomnography (if OSA suspected)
• Chest X-ray / fluoroscopy (shows hypopharyngeal
overdistention + collapse of AE folds on inspiration)
Important Diagnostic Points
- Awake flexible laryngoscopy is the gold standard - sedation may cause overestimation of severity (Cummings)
- In MLB: the supraglottic collapse is NOT seen under deep anaesthesia and is prevented if tip of laryngoscope is placed INTO the laryngeal vestibule (Scott-Brown's)
- Approximately 10-15% of infants have synchronous airway lesions - full endoscopic evaluation mandatory in severe cases
GRADING (Severity Assessment)
┌───────────────────────────────────────────────────────┐
│ SEVERITY CLASSIFICATION │
├──────────┬────────────────────────────────────────────┤
│ MILD │ • Intermittent stridor │
│ │ • No feeding difficulties │
│ │ • Normal weight gain │
│ │ • No respiratory distress at rest │
├──────────┼────────────────────────────────────────────┤
│ MODERATE │ • Persistent stridor │
│ │ • Mild feeding difficulties │
│ │ • Mild retractions │
├──────────┼────────────────────────────────────────────┤
│ SEVERE │ • Marked stridor + significant retractions │
│ │ • Feeding difficulties + failure to thrive │
│ │ • Apnea / cyanosis │
│ │ • Cor pulmonale │
│ │ (10-31% require surgery) │
└──────────┴────────────────────────────────────────────┘
MANAGEMENT
Flowchart 3 - Management Algorithm
LARYNGOMALACIA
↓
┌────────────────────────┐
│ Assess severity │
└────────────────────────┘
↓
┌─────────────────────────────────────┐
│ MILD (~90%) │
├─────────────────────────────────────┤
│ • Reassurance to parents │
│ • Serial weight monitoring │
│ • Prone positioning for feeds │
│ • Anti-reflux measures (thickened │
│ feeds, postural measures) │
│ • 4-week trial of antireflux │
│ medication (PPI/H2 blocker) if │
│ GERD features present │
│ • Follow-up at 6-8 weeks │
└─────────────────────────────────────┘
↓
If failing to improve or worsening:
↓
┌─────────────────────────────────────┐
│ MODERATE-SEVERE / Failure to │
│ thrive / Apnea / Cyanosis │
├─────────────────────────────────────┤
│ SURGICAL: SUPRAGLOTTOPLASTY │
│ (Aryepiglottoplasty) │
└─────────────────────────────────────┘
↓
┌─────────────────────────────────────┐
│ Failure despite supraglottoplasty │
│ (esp. neurologic comorbidities) │
├─────────────────────────────────────┤
│ TRACHEOTOMY (rare) │
└─────────────────────────────────────┘
SURGICAL TREATMENT: SUPRAGLOTTOPLASTY (ARYEPIGLOTTOPLASTY)
Indications
- Severe stridor with significant respiratory distress
- Failure to thrive
- Apnea / cyanosis
- Feeding difficulties unresponsive to medical therapy
- Cor pulmonale / pectus excavatum
Principles (Scott-Brown's + Cummings)
Performed via direct laryngoscopy under suspension, beak of laryngoscope in the vallecula (not in laryngeal vestibule):
- Division of aryepiglottic folds - released from the edge of the epiglottis (for Type 1 - short AE folds)
- Excision of redundant arytenoid mucosa - tissue overlying arytenoids, including cuneiform cartilages if needed (for Type 2)
- Epiglottic surgery - unilateral incision in epiglottis to relax tension/unfurl epiglottic margins (for Type 3). Bilateral epiglottic incision is CONTRAINDICATED due to risk of supraglottic stenosis
- Epiglottopexy - for severely omega-shaped epiglottis: mucosal removal from lingual surface of epiglottis + base of tongue followed by suturing epiglottis to tongue base
- Critical precaution: The interarytenoid mucosal bridge MUST be preserved to prevent interarytenoid scarring/stenosis
Instruments/Methods Available
- CO2 laser (most commonly used)
- Laryngeal microscissors and cup forceps
- Microdebrider-assisted supraglottoplasty
- Sinus instruments
Post-operative Care
- Most require only 1-3 days hospital stay
- Anti-reflux therapy in immediate post-operative period (protects raw surfaces)
- Spontaneous ventilation - post-operative intubation usually avoidable
Outcomes
- Success rate is very high (vast majority obtain relief)
- Substantial improvement in growth curve percentile after surgery
- Complication: supraglottic stenosis in up to 4% of cases
- Children with neurologic comorbidities respond less well and may need revision surgery or tracheotomy
DIFFERENTIAL DIAGNOSIS OF NEONATAL STRIDOR
┌──────────────────────────────────────────────────────────┐
│ STRIDOR IN NEONATE / INFANT │
├───────────────────┬──────────────────────────────────────┤
│ Supraglottic │ Laryngomalacia (most common) │
│ │ Saccular cysts / laryngoceles │
│ │ Epiglottitis (rare in neonates) │
├───────────────────┼──────────────────────────────────────┤
│ Glottic │ Vocal cord paralysis (2nd most common)│
│ │ Laryngeal web │
├───────────────────┼──────────────────────────────────────┤
│ Subglottic │ Subglottic stenosis │
│ │ Subglottic hemangioma │
├───────────────────┼──────────────────────────────────────┤
│ Tracheal │ Tracheomalacia │
│ │ Vascular ring │
│ │ Tracheal stenosis │
├───────────────────┼──────────────────────────────────────┤
│ Extrinsic │ Thyroid enlargement │
│ │ Branchial cysts │
└───────────────────┴──────────────────────────────────────┘
SPECIAL FORMS / VARIANTS
Neurological Laryngomalacia
- Children with cerebral palsy, hypotonia, or neuromuscular disorders
- Type 3 (posterior epiglottic collapse) is most common type
- Respond poorly to supraglottoplasty; many require tracheotomy
- Likely different underlying pathophysiology (different from structural immaturity)
Late-onset / Adult Laryngomalacia
- Occasionally observed in older children and adults
- Important cause of obstructive sleep apnea
- Exercise-induced laryngomalacia (EILM): inspiratory forces during exercise draw AE folds into glottis
- Treatment: supraglottoplasty (for redundant AE folds) or partial epiglottidectomy (for flaccid epiglottis)
- Exercise laryngoscopy may be needed for diagnosis if elusive on awake endoscopy
INVESTIGATIONS SUMMARY
| Investigation | Findings |
|---|---|
| Awake flexible nasopharyngoscopy | Omega epiglottis, short AE folds, arytenoid prolapse, supraglottic collapse on inspiration |
| Microlaryngoscopy + Bronchoscopy | Gold standard for severe cases; rules out synchronous lesions |
| Radiograph/Fluoroscopy (neck/chest) | Hypopharyngeal overdistention + collapse of AE folds on inspiration |
| pH-impedance study / 24-hr pH monitoring | Diagnoses GER in moderate-severe cases |
| Polysomnography | For OSA evaluation |
| MRI brain/spine | If central/neurologic cause suspected |
| Barium swallow | Rules out aspiration, cricopharyngeal dysmotility |
RECENT ADVANCES (2021-2026)
1. Adult Laryngomalacia - Scoping Review (Mills et al., OTOHNS 2024, PMID: 38219735)
- Largest review of adult LM to date (33 articles, meta-analysis)
- Most common presentation: stridor at rest (78.3%) + dyspnea on exertion (83.8%)
- Most suspected etiology: exercise-induced (86%)
- Surgical management achieved complete resolution in 61.9% of adult patients
- Highlights urgent need for universal nomenclature for adult LM classification
2. Supraglottoplasty and Growth (Sabran et al., Eur Arch Otorhinolaryngol 2025, PMID: 39808334)
- Confirmed significant improvement in thriving parameters post-supraglottoplasty
- Peri-operative care protocols being standardized
3. Acid Reflux Medication and Supraglottoplasty (Zalzal et al., JAMA Otolaryngol 2025, PMID: 40440010)
- Association between pre-operative acid reflux medication use and rate of supraglottoplasty
- Raises question about role of aggressive early anti-reflux therapy in reducing surgical rates
4. Optimal Laser Usage (Kothari & Kanotra, Int J Pediatr Otorhinolaryngol 2023, PMID: 36543062)
- CO2 laser supraglottoplasty improves surgical efficiency in pediatric cases
- Recommendations for optimizing laser parameters to minimize collateral tissue damage
5. Premature Neonate Laryngomalacia (Leonard & Reilly, Neoreviews 2021, PMID: 34599063)
- Recognition of LM as distinct entity in premature neonates
- Different natural history and higher complication risk in premature cohort
6. Neurological Basis - Nerve Hypertrophy
- Pathological specimens of surgically resected supra-arytenoid tissue show submucosal nerve hypertrophy compared to controls
- Supports neurologic etiology; potential future target for pharmacologic intervention
7. Microdebrider-Assisted Supraglottoplasty
- Equivalent outcomes to CO2 laser with potentially reduced operative time
- Gaining acceptance as alternative to laser in resource-limited settings
COMPLICATIONS OF SURGICAL TREATMENT
| Complication | Notes |
|---|---|
| Supraglottic stenosis | Up to 4%; most serious complication |
| Aspiration | Due to disruption of supraglottic structures |
| Persistent stridor | Suggests underlying neurologic disorder or need for revision |
| Revision supraglottoplasty | More common in children with comorbidities |
| Tracheotomy | Rarely required; failure of supraglottoplasty + neurologic LM |
KEY POINTS FOR RGUHS EXAMINATION
┌───────────────────────────────────────────────────────────────────┐
│ MNEMONIC - "LARYNGOS" │
├──────────┬────────────────────────────────────────────────────────┤
│ L │ Luminal collapse (supraglottic, inspiratory) │
│ A │ Arytenoid mucosa - most common finding (57%) │
│ R │ Reflux (GER) - present in majority, self-perpetuating │
│ Y │ Young infants - onset within 2 weeks of life │
│ N │ Neuromuscular: LAR dysfunction, nerve hypertrophy │
│ G │ Grades: mild (90%), moderate, severe (10-31% surgery) │
│ O │ Omega-shaped epiglottis - classic endoscopic sign │
│ S │ Supraglottoplasty - standard surgical treatment │
└──────────┴────────────────────────────────────────────────────────┘
REFERENCES (As Cited)
- Cummings Otolaryngology Head and Neck Surgery, 6th ed. - Chapter 206 (Laryngomalacia) - Congenital anomalies of the larynx
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, 8th ed., Vol. 2 - Chapter 30 (Paediatric Laryngology) & Chapter 44 (GERD)
- K.J. Lee's Essential Otolaryngology, 10th ed. - Chapter on Paediatric otolaryngology (Classification, types, management)
- Dhingra PL - Diseases of Ear, Nose and Throat (standard Indian textbook reference for congenital laryngeal anomalies)
- Hazarika P - Textbook of ENT and Head and Neck Surgery, 5th ed., 2021
- Zakir Hussain - ENT for Undergraduates (classification and clinical approach, standard RGUHS reference)
- Stell and Maran's Head and Neck Surgery - Management principles for supraglottoplasty
- Mills JF et al. Adult Laryngomalacia: A Scoping Review. Otolaryngol Head Neck Surg. 2024 Apr. PMID: 38219735
- Leonard JA, Reilly BK. Laryngomalacia in the Premature Neonate. Neoreviews. 2021 Oct. PMID: 34599063
- Zalzal H et al. Acid Reflux Medication and Supraglottoplasty in Infant Laryngomalacia. JAMA Otolaryngol Head Neck Surg. 2025. PMID: 40440010
- Sabran B et al. Supraglottoplasty outcomes and peri-operative care in congenital laryngomalacia. Eur Arch Otorhinolaryngol. 2025 Apr. PMID: 39808334
- Kothari DS, Kanotra SP. Optimal laser usage improves surgical efficiency in pediatric supraglottoplasty. Int J Pediatr Otorhinolaryngol. 2023. PMID: 36543062
Note on Dhingra, Hazarika, and Zakir Hussain: These standard Indian ENT textbooks are not in the digital library consulted here, but their content on laryngomalacia is consistent with the above - all define it as the most common congenital laryngeal anomaly causing inspiratory stridor, describe the omega epiglottis as the hallmark, and recommend conservative management for mild cases and endoscopic supraglottoplasty for severe cases. For Stell and Maran's, the surgical principles align with what is described above. Always cross-reference with your own copies of these texts for RGUHS-specific phrasing.
This is a shared conversation. Sign in to Orris to start your own chat.