What causes hypertension
Reading File
Searching the Web
causes of hypertension pathophysiology 2025
Finding Sources
Searching PubMed
"hypertension" AND "pathophysiology"
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have excellent, comprehensive textbook content. Let me compile the full answer:
Causes of Hypertension
Hypertension is a continuously distributed disorder affecting roughly 45-50% of adults. It is divided into primary (essential) hypertension (90-95% of cases) and secondary hypertension (~5-10%), where a specific underlying cause is identifiable.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 462
- Symptom to Diagnosis: An Evidence-Based Guide, 4th ed.
1. Primary (Essential) Hypertension
No single cause is found. It results from a complex interaction of genetic and environmental factors that converge on two key mechanisms:
A. Reduced renal sodium excretion ("pressure natriuresis resetting")
When the kidneys fail to excrete adequate sodium at normal arterial pressure, fluid volume rises, cardiac output increases, and peripheral vasoconstriction follows - pushing blood pressure higher until a new equilibrium is reached, but at an elevated set point.
B. Increased peripheral vascular resistance
Vasoconstrictive forces (angiotensin II, catecholamines, endothelin) outweigh vasodilators (nitric oxide, kinins, prostaglandins), causing sustained arteriolar constriction.
Contributing factors in essential hypertension:
| Factor | Mechanism |
|---|---|
| Genetics | >500 genetic variants linked to BP; twin studies confirm heritability. Rare single-gene mutations (e.g., ENaC-γ in Liddle syndrome) cause exaggerated renal sodium retention |
| High dietary sodium | Strong evidence links salt intake to hypertension prevalence |
| Obesity | Increases blood volume, activates RAAS, causes sympathetic overdrive, promotes insulin resistance |
| Physical inactivity | Reduces vascular compliance and NO production |
| Stress / sympathetic activation | Catecholamine release raises heart rate and vascular tone |
| Smoking | Acute vasoconstriction; promotes endothelial dysfunction long-term |
| Age | Arterial stiffness increases systolic BP; endothelial dysfunction accumulates |
| Alcohol | Chronic heavy use is an independent risk factor |
2. Secondary Hypertension
These causes are identifiable and potentially reversible. The major categories are:
Renal Causes (most common secondary cause)
- Renal artery stenosis (renovascular hypertension) - reduced flow to the glomerulus triggers renin release, activating RAAS, leading to vasoconstriction and sodium/water retention
- Chronic kidney disease (CKD)
- Acute glomerulonephritis
- Polycystic kidney disease
- Renal vasculitis
- Renin-producing tumors
Endocrine / Adrenal Causes
- Primary hyperaldosteronism (Conn syndrome) - one of the most frequent secondary causes; excess aldosterone causes sodium retention and potassium loss
- Pheochromocytoma - tumor secreting catecholamines (epinephrine/norepinephrine), causing episodic or sustained hypertension
- Cushing syndrome - excess glucocorticoids promote sodium retention
- Hyperthyroidism - increases cardiac output and heart rate
- Congenital adrenal hyperplasia - enzyme defects lead to excess mineralocorticoid activity
- Acromegaly - growth hormone excess
- Hyperparathyroidism
Cardiovascular / Vascular Causes
- Coarctation of the aorta - a mechanical obstruction causing upper-body hypertension
- Aortic stiffness / arteriosclerosis (contributes to isolated systolic hypertension in the elderly)
Other Causes
- Obstructive sleep apnea - hypoxia and sympathetic surges during apnoeic episodes raise BP
- Pregnancy-induced (preeclampsia)
- Ureteral or bladder outlet obstruction
Drug-Induced Hypertension
A wide range of medications can raise blood pressure:
- Oral contraceptive pills (OCPs)
- NSAIDs / COX-2 inhibitors
- Corticosteroids
- Sympathomimetics (decongestants, amphetamines, stimulants like modafinil)
- Cyclosporine and tacrolimus (calcineurin inhibitors)
- Erythropoietin
- Cocaine and alcohol
The RAAS: The Central Mechanism
The renin-angiotensin-aldosterone system (RAAS) sits at the heart of blood pressure control and is dysregulated in many forms of hypertension:
- Juxtaglomerular cells release renin in response to low renal perfusion, low sodium, or elevated catecholamines
- Renin cleaves angiotensinogen → angiotensin I
- ACE (in vascular endothelium) converts it → angiotensin II
- Angiotensin II causes: direct vasoconstriction + aldosterone release + tubular sodium reabsorption → blood pressure rises
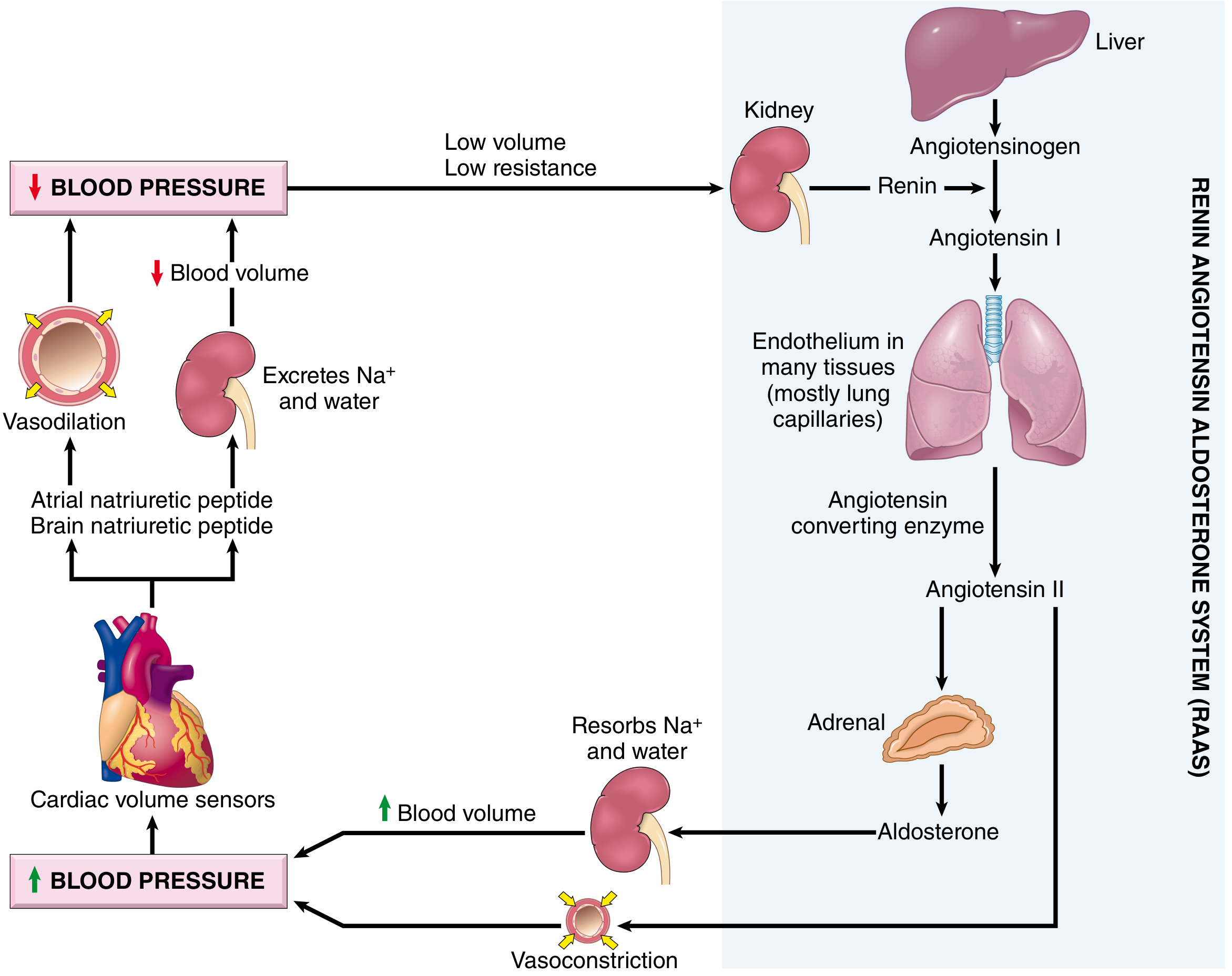
RAAS and natriuretic peptide interplay in blood pressure regulation - Robbins Pathology, Fig. 11.4
Summary
| Type | Prevalence | Key Drivers |
|---|---|---|
| Essential hypertension | 90-95% | Genetics, high sodium, obesity, inactivity, stress, ageing |
| Renal secondary | ~2-3% | RAS activation, fluid retention |
| Endocrine secondary | ~1-2% | Aldosterone, catecholamines, glucocorticoids |
| Drug-induced | variable | RAAS activation, vasoconstriction, sodium retention |
The majority of hypertensive patients will never have a single identified cause. Management focuses on both correcting reversible contributors and blocking the common pathways (RAAS blockade with ACE inhibitors/ARBs, volume control with diuretics, and vasodilation with calcium channel blockers).
- Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 462-464
- Symptom to Diagnosis: An Evidence-Based Guide, 4th Edition
- Rosen's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.