Explain spinal cord anatomy
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have everything needed for a thorough, well-illustrated answer. Let me compile it.
Spinal Cord Anatomy
Overview
The spinal cord is a thin, tubular extension of the central nervous system (CNS) contained within the bony spinal canal. It originates at the medulla oblongata (at the foramen magnum) and continues caudally, terminating as the conus medullaris at approximately the L1-L2 disc level in adults (can range from T12 to L2/L3). In neonates it extends as low as L3-L4 due to differential growth. The adult cord is approximately 46 cm long. - Harrison's Principles of Internal Medicine, 22E
A fine fibrous extension called the filum terminale (pial part) continues from the apex of the conus medullaris down to the coccyx, anchoring the cord. The subarachnoid space below the conus (down to S2) contains the cauda equina - the collection of lumbosacral nerve roots that travel down before exiting their respective foramina. - Gray's Anatomy for Students
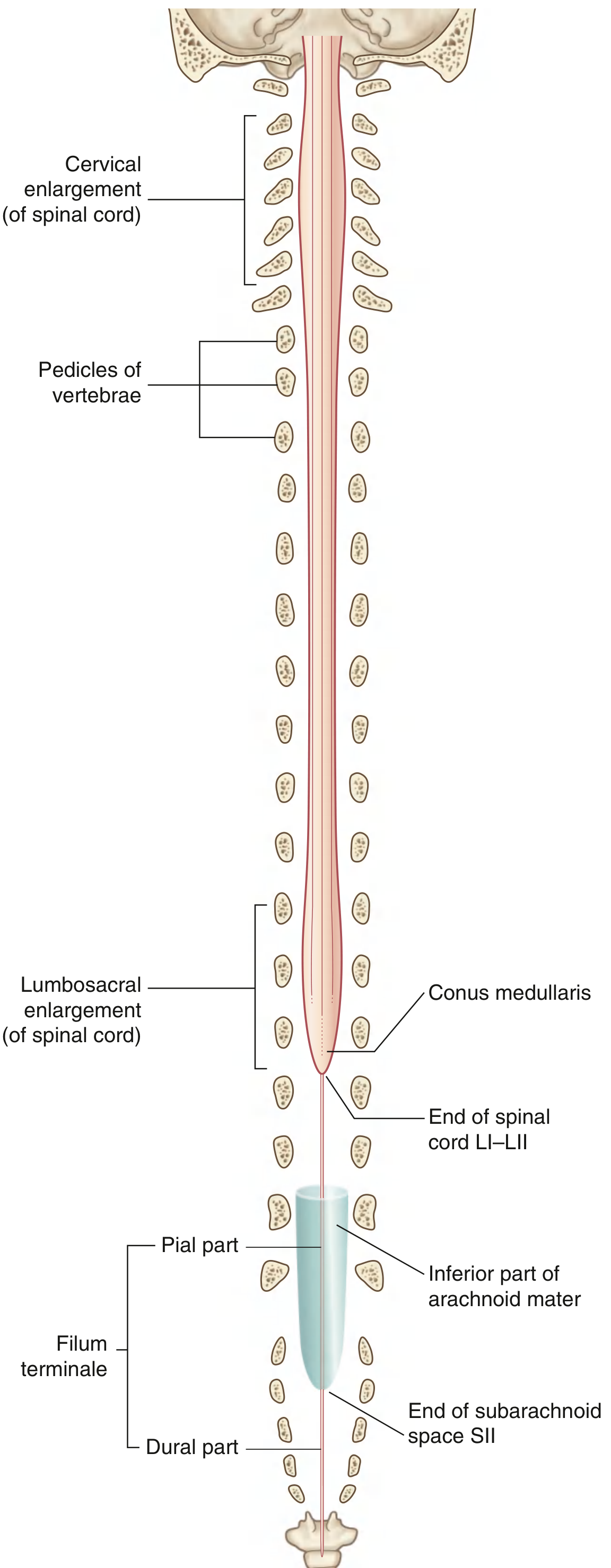
Fig. 2.53 - Gray's Anatomy for Students: The spinal cord with enlargements, conus medullaris, and filum terminale.
Segments and Spinal Nerves
The cord has 31 segments, each defined by a pair of entering dorsal (sensory) roots and exiting ventral (motor) roots:
- 8 cervical (C1-C8)
- 12 thoracic (T1-T12)
- 5 lumbar (L1-L5)
- 5 sacral (S1-S5)
- 1 coccygeal
An important clinical rule: C1-C7 nerves exit above their same-numbered vertebra; C8 exits below C7; all subsequent nerves exit below their same-numbered vertebra. This arises because there are 8 cervical cord segments but only 7 cervical vertebrae. The mismatch between cord level and vertebral level increases as you descend - sacral cord segments sit at the T11-L1 vertebral levels. - Harrison's Principles, 22E
External Surface Markings
The external cord surface has several longitudinal fissures and sulci: - Gray's Anatomy for Students
- Anterior median fissure - deep groove along the entire anterior surface
- Posterior median sulcus - shallow groove along the posterior surface
- Posterolateral sulci (bilateral) - where posterior nerve rootlets enter the cord
- Anterolateral sulci - where anterior (motor) rootlets exit
Enlargements
The cord is not uniform in diameter. Two enlargements correspond to limb innervation: - Gray's Anatomy for Students
| Enlargement | Cord Levels | Limb |
|---|---|---|
| Cervical enlargement | C5-T1 | Upper limbs (brachial plexus) |
| Lumbosacral enlargement | L1-S3 | Lower limbs (lumbosacral plexus) |
These enlargements have proportionally more gray matter in the ventral horns due to the large number of lower motor neurons supplying the limbs.
Meninges and Protective Coverings
Three membranes (continuous with cranial meninges) enclose the cord: - Campbell's Operative Orthopaedics, 15E
- Pia mater - innermost layer, closely applied to cord surface
- Arachnoid mater - middle, delicate membrane
- Dura mater - tough outermost sheath
The subarachnoid space (between pia and arachnoid) contains cerebrospinal fluid (CSF). The epidural space (outside the dura) contains fat and a venous plexus. The denticulate ligaments are lateral tooth-like projections of pia that anchor the cord to the dura between nerve roots.
Internal Structure: Gray Matter
Internally, the cord has a butterfly/H-shaped central gray matter (rich in neuronal cell bodies) surrounded by white matter (myelinated tracts). A small central canal runs the full length, connecting with the fourth ventricle. - Neuroanatomy through Clinical Cases, 3E
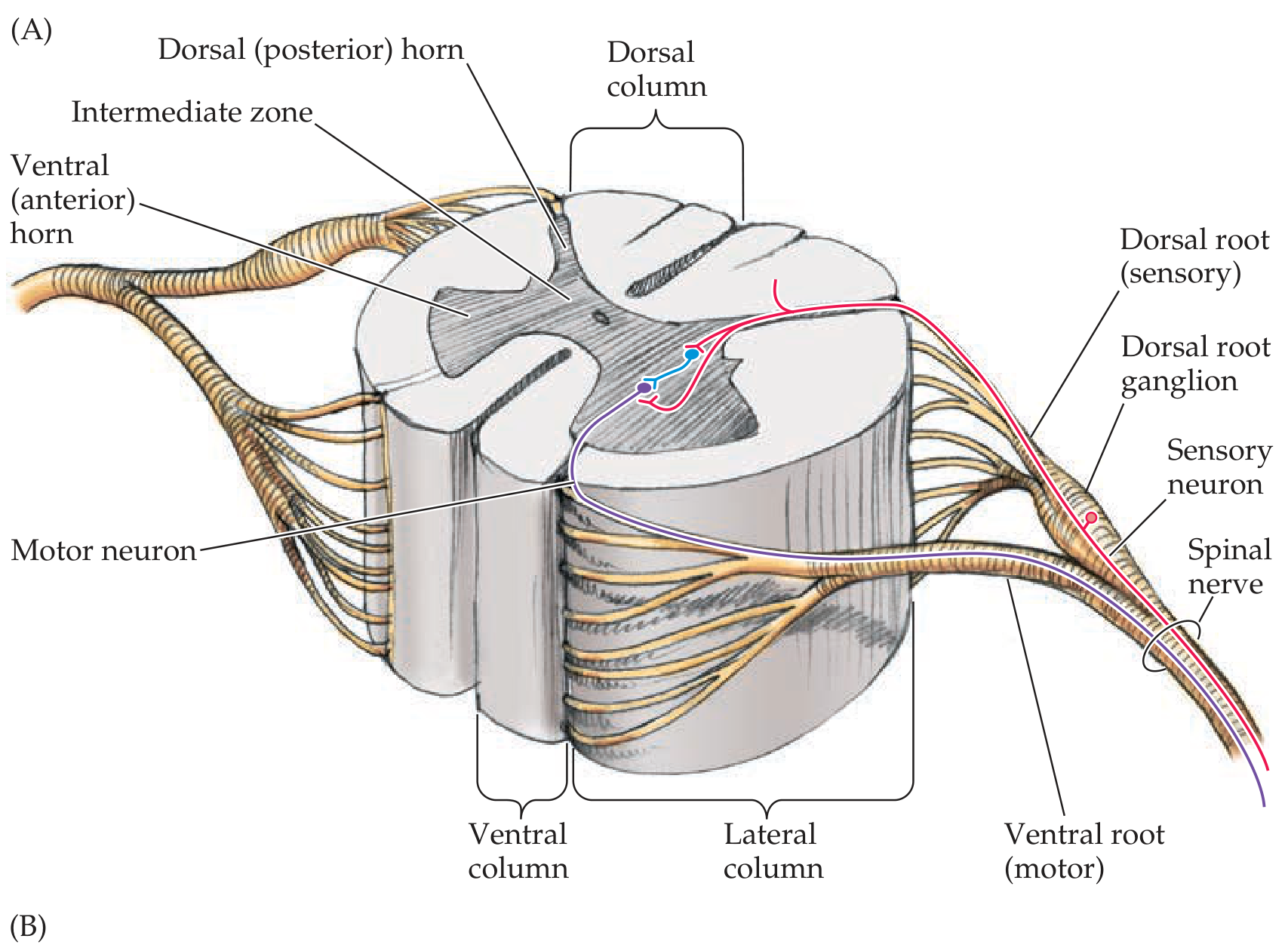
Gray matter, white matter columns, dorsal (sensory) and ventral (motor) roots - Neuroanatomy through Clinical Cases, 3E.
The gray matter has three columns on each side:
| Column | Function |
|---|---|
| Dorsal (posterior) horn | Sensory processing - receives afferent input |
| Lateral (intermediate) horn | Autonomic neurons (T1-L2: sympathetic preganglionic; S2-S4: parasympathetic) |
| Ventral (anterior) horn | Motor neurons - sends efferent output to muscles |
Rexed's Laminae
Swedish anatomist Bror Rexed described 10 cytoarchitectural layers within the gray matter: - Localization in Clinical Neurology, 8E and Neuroanatomy through Clinical Cases, 3E
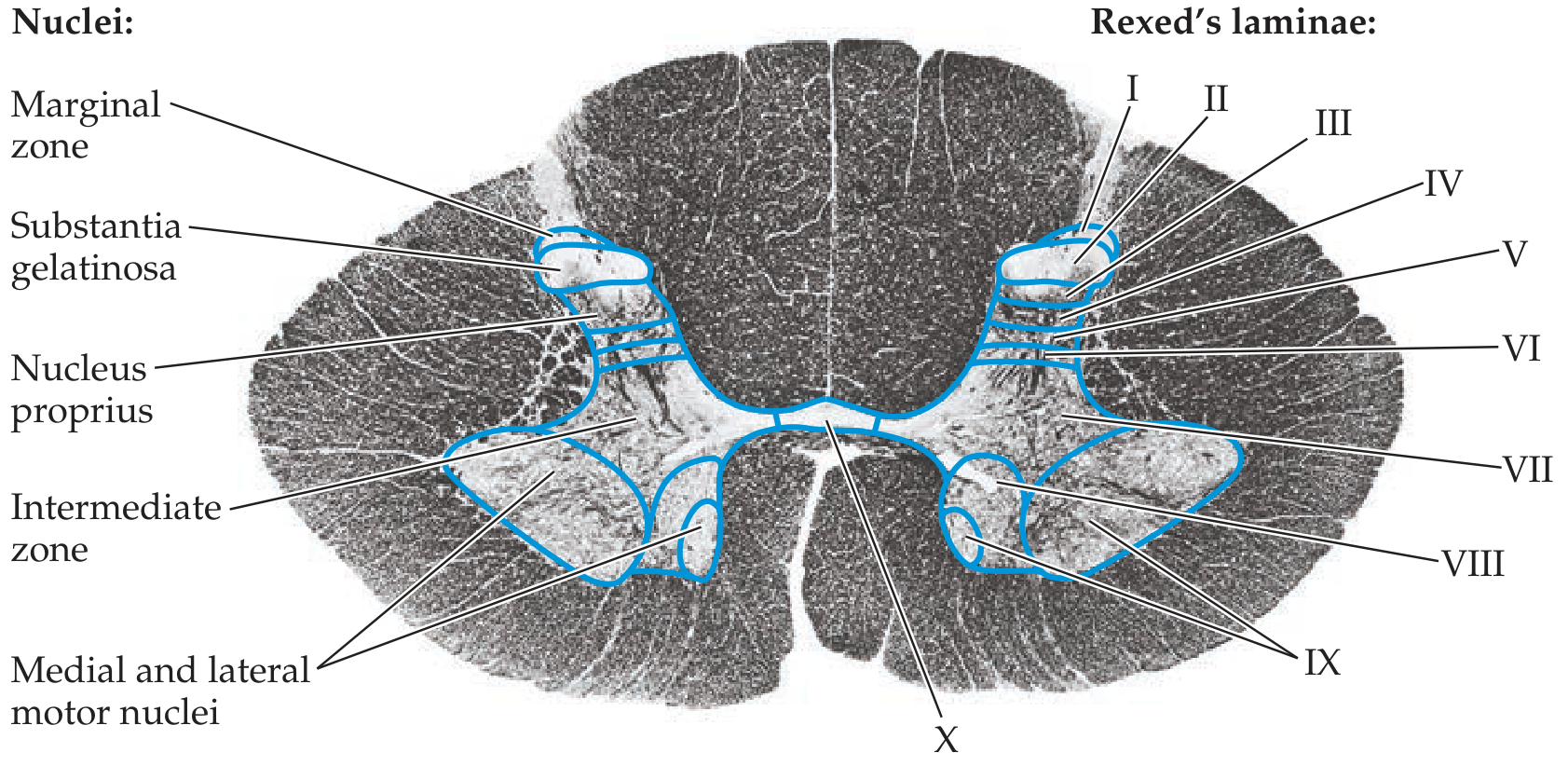
Rexed's laminae (I-X) with named nuclei - Neuroanatomy through Clinical Cases, 3E.
| Lamina | Region | Key Nuclei / Function |
|---|---|---|
| I | Dorsal horn tip | Marginal zone (nucleus posteromarginalis) - pain/temperature |
| II | Dorsal horn | Substantia gelatinosa of Rolando - pain modulation |
| III-IV | Dorsal horn | Nucleus proprius - sensory integration |
| V | Neck of dorsal horn | Receives nociceptive and visceral input |
| VI | Base of dorsal horn | Proprioceptive and cutaneous input |
| VII | Intermediate zone | Clarke's nucleus (spinocerebellar), intermediolateral nucleus (sympathetic) |
| VIII | Ventral horn (medial) | Commissural interneurons |
| IX | Ventral horn | Alpha and gamma motor neuron columns |
| X | Around central canal | Gray commissure |
Alpha motor neurons (lamina IX) innervate extrafusal skeletal muscle fibers. Gamma motor neurons innervate intrafusal fibers of muscle spindles, regulating stretch reflex sensitivity.
Internal Structure: White Matter
The white matter is organized into three bilateral funiculi (columns): - Localization in Clinical Neurology, 8E
- Dorsal (posterior) funiculus - between dorsomedial and dorsolateral sulci
- Lateral funiculus - between dorsolateral and ventrolateral sulci
- Ventral (anterior) funiculus - between ventrolateral sulcus and anterior median fissure
The white matter is thickest in the cervical cord (where all ascending fibers have entered and most descending fibers haven't yet terminated) and thinnest in the sacral cord (which is mostly gray).
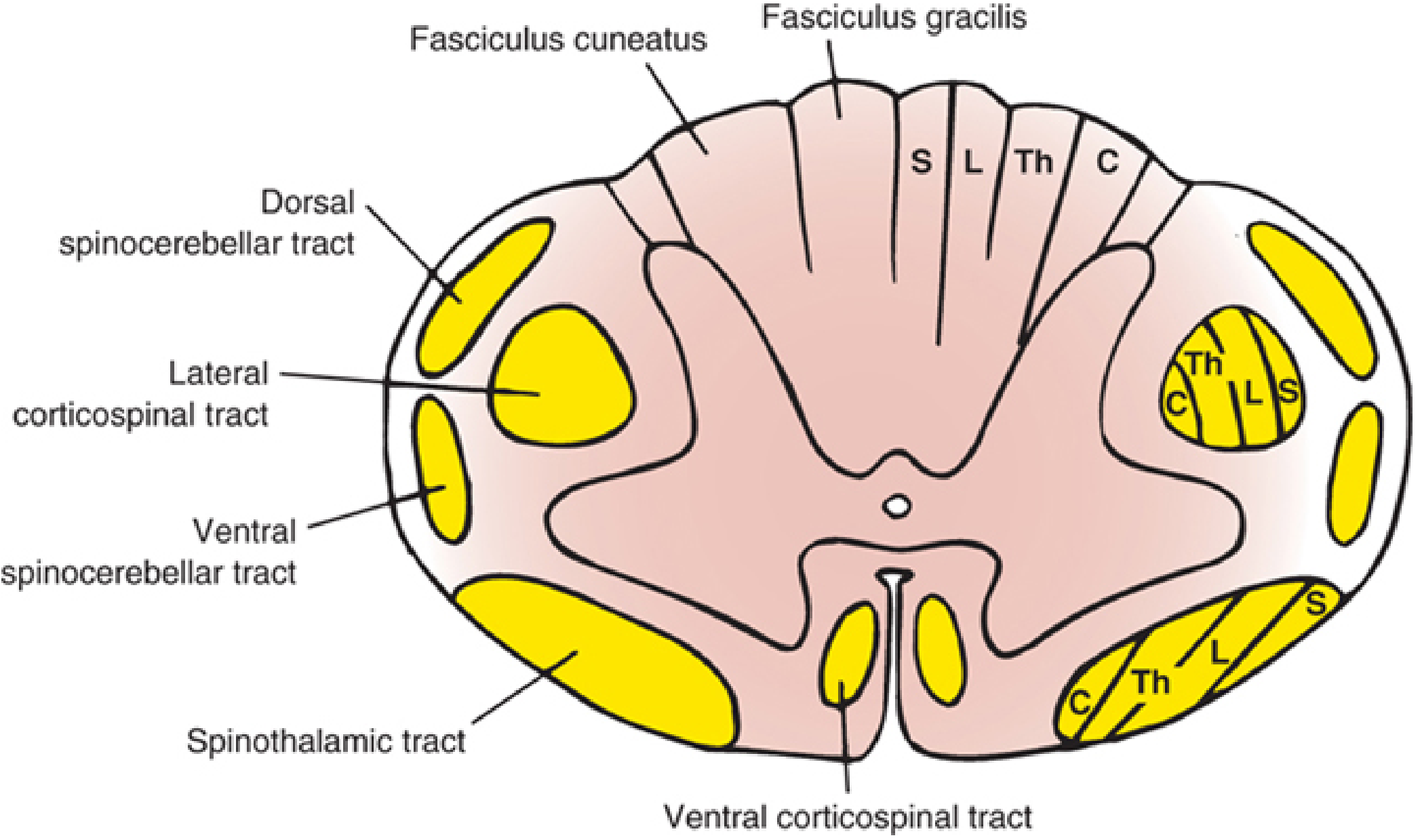
Major tracts and somatotopic lamination - Localization in Clinical Neurology, 8E. Note: in the spinothalamic and corticospinal tracts, sacral fibers are most peripheral.
Key Ascending (Sensory) Tracts
| Tract | Location | Modality | Decussation |
|---|---|---|---|
| Fasciculus gracilis | Dorsal funiculus (medial) | Deep touch, proprioception, vibration from lower body (sacral-T7) | At medulla (nucleus gracilis) |
| Fasciculus cuneatus | Dorsal funiculus (lateral) | Deep touch, proprioception, vibration from upper body (T6-C1) | At medulla (nucleus cuneatus) |
| Lateral spinothalamic tract | Lateral funiculus | Pain and temperature | Crosses via ventral white commissure within 1-2 segments of entry |
| Ventral spinothalamic tract | Ventral funiculus | Light touch (crude) | Crosses via ventral white commissure |
| Dorsal spinocerebellar tract | Lateral funiculus (posterior) | Unconscious proprioception from lower limbs | Ipsilateral (uncrossed) |
| Ventral spinocerebellar tract | Lateral funiculus (anterior) | Unconscious proprioception | Crossed (then recrosses in cerebellum) |
The lateral spinothalamic tract shows clear somatotopic lamination: sacral fibers lie most ventrolaterally (peripheral), and cervical fibers most dorsomedially (central). This explains why central cord lesions (e.g., syrinx) spare sacral sensation ("sacral sparing"). - Campbell's Operative Orthopaedics, 15E
Key Descending (Motor) Tracts
| Tract | Location | Origin | Function |
|---|---|---|---|
| Lateral corticospinal tract | Lateral funiculus | Contralateral motor cortex (decussates in medulla) | Voluntary movement of distal limbs (~90% of fibers) |
| Ventral corticospinal tract | Ventral funiculus | Ipsilateral cortex (crosses at segmental level) | Axial and proximal muscles (~10%) |
| Rubrospinal tract | Lateral funiculus | Red nucleus | Limb movement (less significant in humans) |
| Vestibulospinal tract | Ventral/lateral funiculus | Lateral vestibular nucleus | Postural tone, extensor facilitation |
| Reticulospinal tracts | Ventral/lateral funiculi | Medullary and pontine reticular formation | Muscle tone, autonomic function |
The lateral corticospinal tract is somatotopically arranged with cervical fibers most medial and sacral fibers most lateral - the reverse of the spinothalamic tract. - Localization in Clinical Neurology, 8E
Vascular Supply
The cord receives blood from three longitudinal arteries and their segmental reinforcements: - Bradley and Daroff's Neurology in Clinical Practice
- Anterior spinal artery (ASA) - single vessel formed by branches of both vertebral arteries; runs in the anterior median fissure; supplies the anterior 2/3 of the cord (anterior horns, spinothalamic tracts, corticospinal tracts)
- Posterior spinal arteries (PSA x2) - paired vessels from the posterior inferior cerebellar arteries; supply the posterior 1/3 (dorsal columns)
- Radicular/segmental arteries - reinforce the ASA and PSA at intervals; the largest is the artery of Adamkiewicz (arteria radicularis magna), which typically enters at T9-T12 on the left and is the dominant supply to the lower thoracic and lumbosacral cord
The mid-thoracic cord (T4-T8) is a watershed zone with relatively poor blood supply, making it especially vulnerable to ischemia.
Clinical correlate: ASA occlusion causes anterior cord syndrome - bilateral motor loss (corticospinal) and loss of pain/temperature (spinothalamic) below the lesion, with sparing of dorsal column function (vibration, proprioception). - Bradley and Daroff's Neurology in Clinical Practice
Summary: Major Spinal Cord Syndromes and Their Anatomic Basis
| Syndrome | Lesion Site | Deficits |
|---|---|---|
| Complete transection | All tracts | Total motor + sensory loss below lesion |
| Brown-Séquard (hemisection) | One lateral half | Ipsilateral motor + proprioception loss; contralateral pain/temperature loss |
| Central cord syndrome | Central gray + medial white | Arms > legs weakness; sacral sparing of sensation |
| Anterior cord syndrome | Anterior 2/3 (ASA territory) | Motor + pain/temperature loss; vibration/proprioception preserved |
| Posterior cord syndrome | Dorsal columns | Loss of vibration, proprioception, discriminative touch; motor intact |
Sources: Neuroanatomy through Clinical Cases, 3E | Localization in Clinical Neurology, 8E | Harrison's Principles of Internal Medicine, 22E | Gray's Anatomy for Students | Campbell's Operative Orthopaedics, 15E | Bradley and Daroff's Neurology in Clinical Practice
Can explain from snell
Finding Sources
Finding Sources
Finding Sources
Snell's Clinical Neuroanatomy is not available in the library. Here is the complete list of anatomy/neurology/neuroscience books that are in the collection:
Anatomy:
- Gray's Anatomy for Students
- General Anatomy and Musculoskeletal System (Thieme Atlas)
- Netter's Atlas of Human Anatomy
- Color Atlas of Human Anatomy Vol. 1, 2, 3
- Imaging Anatomy (Bones, Joints, Vessels and Nerves)
- Color Atlas of Ultrasound Anatomy
Neurology / Neuroanatomy / Neuroscience:
- Neuroanatomy through Clinical Cases, 3rd Ed. (Blumenfeld)
- Adams and Victor's Principles of Neurology, 12th Ed.
- Bradley and Daroff's Neurology in Clinical Practice
- Localization in Clinical Neurology, 8e
- Principles of Neural Science, 6th Ed. (Kandel)
- Neuroscience: Exploring the Brain, 5th Ed.
- Plum and Posner's Diagnosis and Treatment of Stupor and Coma
Snell's is not among them. The closest equivalent for a Snell-style systematic regional neuroanatomy approach would be Blumenfeld's Neuroanatomy through Clinical Cases - which is exactly what I drew on heavily in the previous explanation. That book covers spinal cord anatomy in the same organized, clinically-grounded style that Snell is known for.
Would you like me to go deeper into the spinal cord content from Blumenfeld (tracts, clinical correlations, level-by-level cross sections), or from Gray's Anatomy for Students which also covers it very systematically?
This is a shared conversation. Sign in to Orris to start your own chat.