Electroretinogram for 20marks
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
I now have comprehensive, well-illustrated content from two authoritative textbooks. Let me compile the full 20-mark answer.
Electroretinogram (ERG)
Definition
The electroretinogram (ERG) is a diagnostic test that measures the electrical activity of the retina in response to a light stimulus. When photoreceptors and other retinal neurons are stimulated by light, ionic flow (principally Na⁺ and K⁺) is induced, generating a potential difference that can be recorded from the corneal surface.
— Kanski's Clinical Ophthalmology, 10th ed.
Principle & Recording Setup
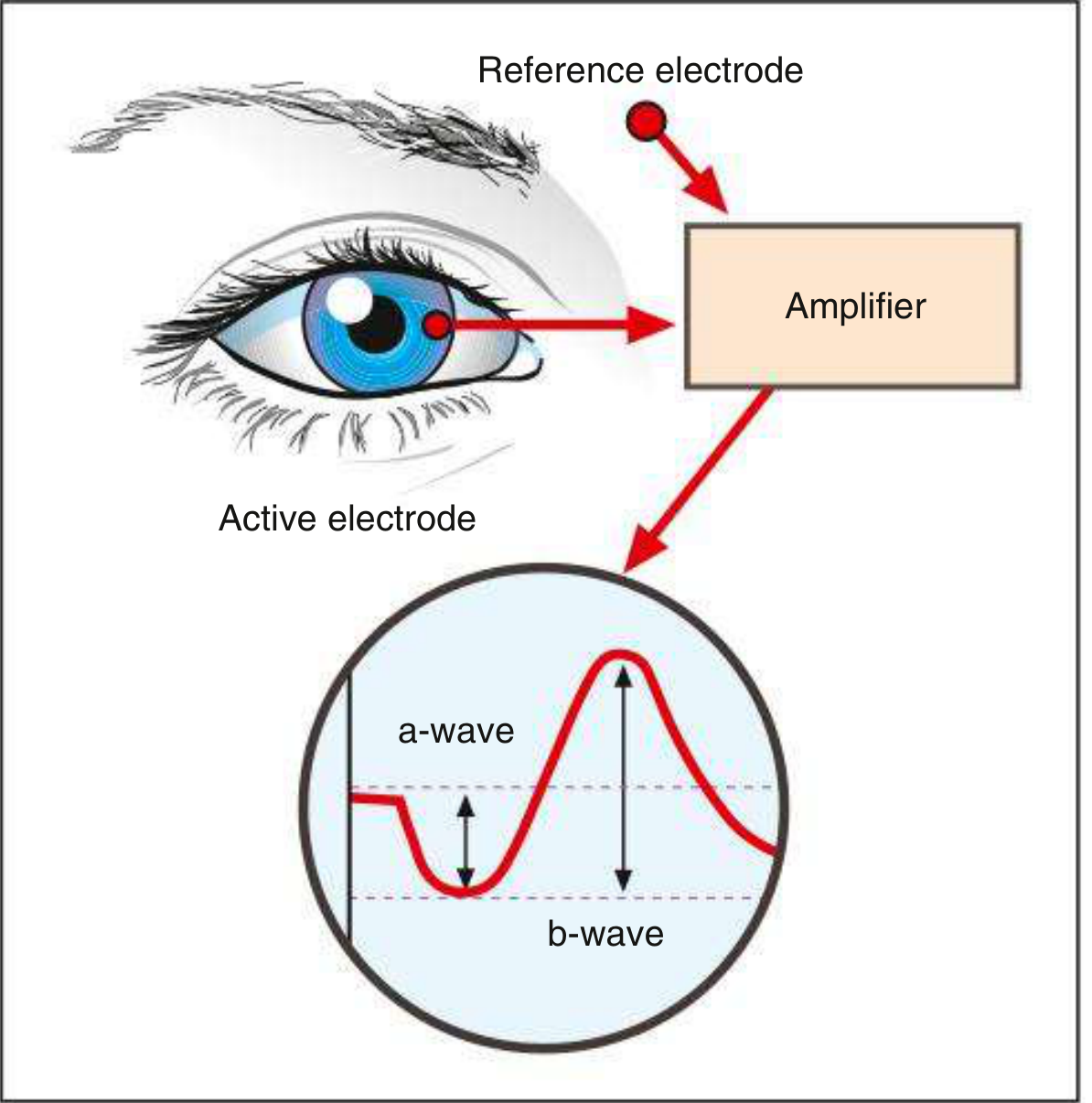
- An active (corneal) electrode — placed on or near the cornea (contact lens electrode)
- A reference electrode — placed on the forehead or earlobe
- A ground electrode — placed elsewhere on the body
- The potential difference between the two electrodes is amplified and displayed
The ERG is a summed mass response of the entire retina; normal results therefore do not exclude focal pathology.
Components of the Normal ERG Waveform
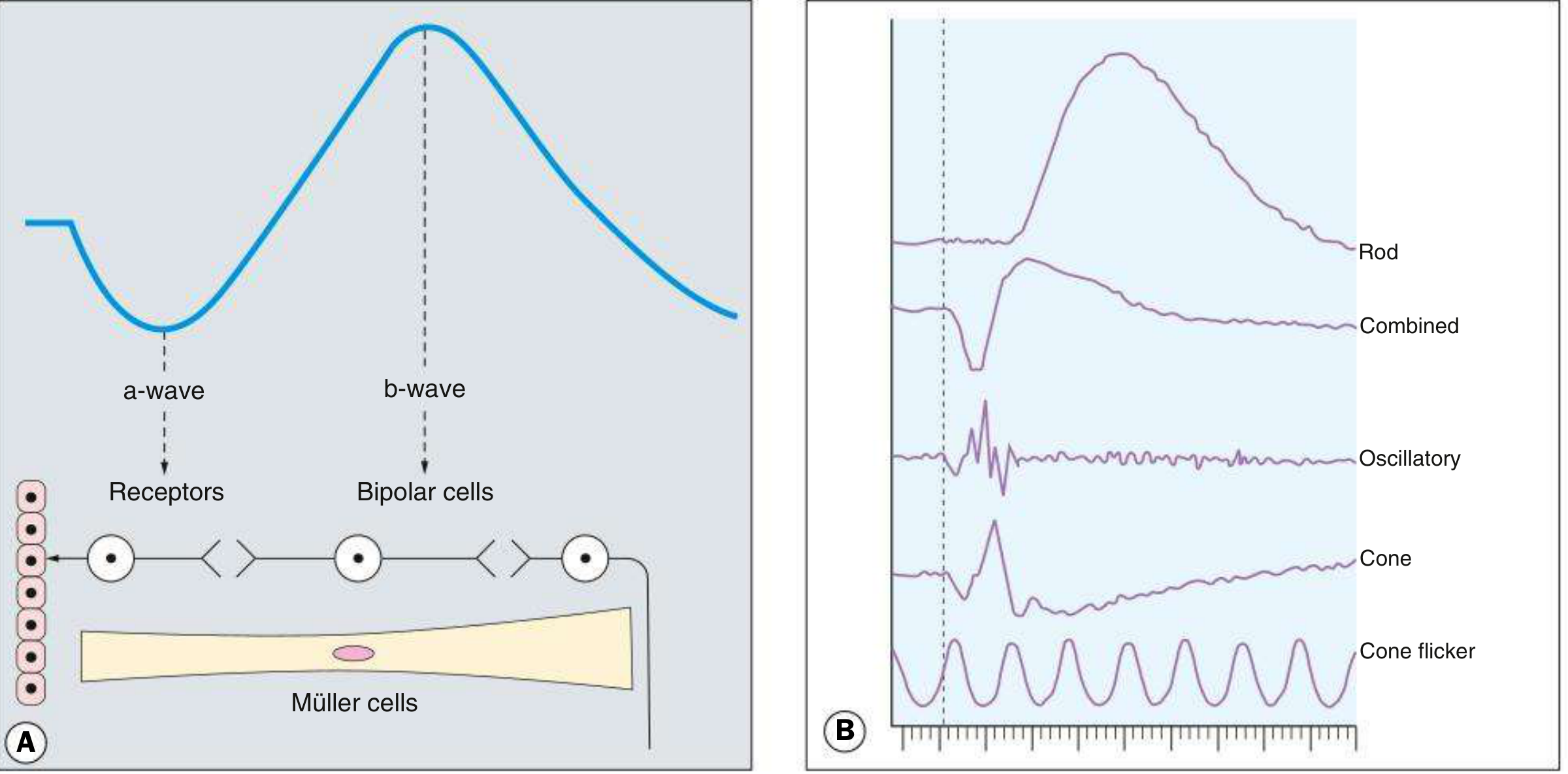
The normal ERG is predominantly biphasic:
| Component | Deflection | Origin | Significance |
|---|---|---|---|
| a-wave | Initial corneal-negative (downward) deflection | Photoreceptors (rods & cones) — hyperpolarization | Reflects photoreceptor integrity |
| b-wave | Subsequent large positive (upward) deflection | Müller cells & bipolar cells (ON-bipolar cells) — depolarization | Dependent on functional photoreceptors; most clinically useful |
| c-wave | Third negative deflection | RPE + photoreceptors | Less commonly measured clinically |
| Oscillatory potentials | Wavelets on the ascending limb of the b-wave | Inner retinal amacrine cells | Reflect inner retinal inhibitory processing |
Key measurements:
- Amplitude of b-wave — measured from the a-wave trough to the b-wave peak
- Latency — time from stimulus to commencement of the a-wave
- Implicit time — time from stimulus to b-wave peak
- b:a ratio — a reduced ratio indicates inner retinal dysfunction
Types of ERG
1. Full-field ERG (Ganzfeld ERG)
- Standardised by the International Society for Clinical Electrophysiology of Vision (ISCEV)
- Uses diffuse stimulation of the entire retina
- Consists of 6 standard recordings (ISCEV 2022 update)
- Assesses generalised retinal disorders; cannot detect localised pathology
Scotopic (dark-adapted) responses — after ≥20 min dark adaptation:
- Dim flash (0.01 cd·s/m²) → rod-only response: small b-wave, barely visible a-wave
- Bright white flash → combined rod-cone response: prominent a-wave and b-wave
- Oscillatory potentials → bright flash with modified recording parameters
Photopic (light-adapted) responses — after 10 min light adaptation (to suppress rods):
- Bright single flash → cone a- and b-wave
- 30 Hz flicker → isolates cones (rods cannot follow >20 Hz); measures cone b-wave amplitude and implicit time
2. Multifocal ERG (mfERG)
- Produces topographical maps of retinal function across the macular region
- Patient fixates on an array of flickering hexagons (scaled for photoreceptor density — smaller stimulus at the fovea where density is high)
- Results displayed as a 3D plot resembling the hill of vision
- Used in: early cone-rod dystrophies (occult macular dystrophy), autoimmune retinopathies (normal fundal appearance), macular RP
3. Pattern ERG (PERG)
- Uses pattern-reversal stimulus (same as VEP)
- Targets retinal ganglion cell function
- Used to detect subtle optic neuropathy and early glaucoma
4. Focal ERG
- Assesses macular function specifically
- Rarely used clinically
Interpretation Patterns
| ERG Pattern | Meaning | Associated Conditions |
|---|---|---|
| Extinguished (flat) ERG | No recordable responses | Advanced retinitis pigmentosa, cancer-associated retinopathy (CAR) |
| Electronegative ERG (b-wave < a-wave) | Impaired photoreceptor-to-bipolar cell signalling | CRAO, congenital stationary night blindness (CSNB), melanoma-associated retinopathy (MAR), X-linked retinoschisis |
| Selectively impaired rod responses | Rod-cone dystrophy | Retinitis pigmentosa |
| Selectively impaired cone responses | Cone/cone-rod dystrophy | Cone dystrophy |
| Reduced oscillatory potentials | Inner retinal amacrine cell dysfunction | Early diabetic retinopathy, mild CRVO |
| Prolonged implicit time | Delayed retinal signal transmission | Clinically significant in various dystrophies |
Clinical Applications
- Diagnosis of inherited retinal dystrophies — retinitis pigmentosa, cone-rod dystrophy, CSNB, Leber congenital amaurosis
- Monitoring disease progression in dystrophies and uveitis (e.g., birdshot retinopathy)
- Drug toxicity monitoring — e.g., hydroxychloroquine, vigabatrin toxicity
- Detecting retinal ischaemia — CRAO, CRVO, diabetic retinopathy
- Paraneoplastic retinopathies — CAR (extinguished ERG), MAR (electronegative ERG)
- Intraocular foreign body (IOFB) — serial ERGs to monitor for siderosis
- Screening before surgery — assessing retinal function when media are opaque (dense cataract, vitreous haemorrhage) before vitreoretinal surgery
- Neonatal/paediatric evaluation — visual function in infants unable to cooperate with subjective tests
Comparison: ERG vs EOG
| Feature | ERG | EOG (Electro-oculogram) |
|---|---|---|
| What it measures | Mass retinal electrical activity | Standing potential (cornea-positive, fundus-negative) |
| Origin | Photoreceptors, bipolar/Müller cells, RPE | RPE and photoreceptors |
| Key result | Wave amplitudes & implicit times | Arden ratio (light peak ÷ dark trough) |
| Normal Arden ratio | — | ≥1.85 |
| Classic disorder | Retinitis pigmentosa (extinguished ERG) | Best disease (markedly reduced EOG, normal ERG) |
Important Points for Examination
- ERG is a mass retinal response — cannot detect localised disease
- The b-wave is larger than the a-wave under normal conditions
- Dark adaptation for 30 min is required before scotopic testing; 10 min light adaptation for photopic testing
- An electronegative ERG (b/a ratio <1) is a critical diagnostic clue for CSNB, MAR, CRAO
- Retinitis pigmentosa → rods affected first → scotopic ERG reduced earlier than photopic
- Pattern ERG assesses ganglion cells; mfERG maps macular function
- Standardised by ISCEV (International Society for Clinical Electrophysiology of Vision)
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th edition | Bradley and Daroff's Neurology in Clinical Practice
Cystoid maculae edema
Checking Date & Time
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have comprehensive content with excellent images. Let me compile the full answer.
Cystoid Macular Edema (CME)
Definition
Cystoid macular edema (CME) is the accumulation of fluid in the outer plexiform layer (OPL) and inner nuclear layer (INL) of the retina at the macula, forming tiny cyst-like (cystoid) cavities. It is not a disease but a non-specific manifestation of any condition causing macular oedema.
Fluid initially accumulates intracellularly in Müller cells, with subsequent rupture and coalescence of smaller cavities. Over time, progression to a foveal lamellar hole may occur, causing irreversible central visual loss.
— Kanski's Clinical Ophthalmology, 10th ed.
Pathophysiology
The key mechanism is breakdown of the inner or outer blood-retinal barrier (BRB):
- Disruption of tight junctions in retinal vascular endothelium (inner BRB) or RPE (outer BRB)
- Accumulation of fluid in the perifoveal Henle fibre layer (OPL), which has an oblique orientation — this causes the characteristic petaloid pattern on fluorescein angiography
- Müller cells initially buffer excess fluid; when overwhelmed, intracellular oedema ruptures to form extracellular cystic spaces
- Prostaglandins and VEGF are key mediators of vascular permeability
Etiology / Causes
Postoperative (most common overall)
- Irvine-Gass syndrome — after cataract extraction (peak incidence 6–10 weeks post-op)
- Risk factors: vitreous loss, vitreous incarceration in the wound, iris prolapse, anterior chamber IOL, secondary IOL, diabetes, uveitis, topical prostaglandin use
- After laser photocoagulation, cryotherapy, vitreoretinal surgery
Retinal Vascular Disease
- Diabetic macular oedema (most common cause of CME globally)
- Central retinal vein occlusion (CRVO) and branch RVO (BRVO)
Inflammatory
- Intermediate uveitis (pars planitis) — particularly associated
- Severe or chronic uveitis of any type
- Retinal vasculitis: Eales disease, Behçet syndrome, sarcoidosis, MS, CMV retinitis
Drug-induced
- Topical prostaglandin analogues (latanoprost, bimatoprost)
- Topical epinephrine / dipivefrin
- Nicotinic acid (high dose)
- Taxane chemotherapy drugs
Retinal Dystrophies
- Retinitis pigmentosa (RP)
- Dominant cystoid macular oedema (inherited form)
Vitreomacular Traction
- Epiretinal membrane (ERM)
- Vitreomacular traction syndrome
Others
- AMD (neovascular / MNV)
- Retinal telangiectasias (Coats disease, idiopathic macular telangiectasia)
- Fundus tumours (retinal capillary haemangioma)
- Systemic conditions: chronic renal failure, hypertension, collagen vascular disease
- Subfoveal choroidal neovascularisation
Symptoms
- Decreased central visual acuity (especially for near tasks)
- Metamorphopsia (distortion of straight lines)
- Micropsia (objects appear smaller)
- Central scotoma on Amsler grid testing
- Subtle CME may be asymptomatic
Signs
On Slit-lamp / Fundoscopy
- Irregularity and blunting of the foveal light reflex
- Macular thickening with or without small intraretinal cysts in the foveal region (best seen with red-free light using a fundus contact lens)
- Loss of the foveal depression
- Multiple cystoid (honey-comb) areas in the sensory retina
- Optic disc swelling may be present (especially in Irvine-Gass)
- A lamellar hole may be visible in advanced cases
- Vitreous cells, dot haemorrhages depending on etiology
Investigations
1. Histology

Cystic spaces (white lacunae) in the OPL and INL on H&E section.
2. Fluorescein Angiography (FA/IVFA)
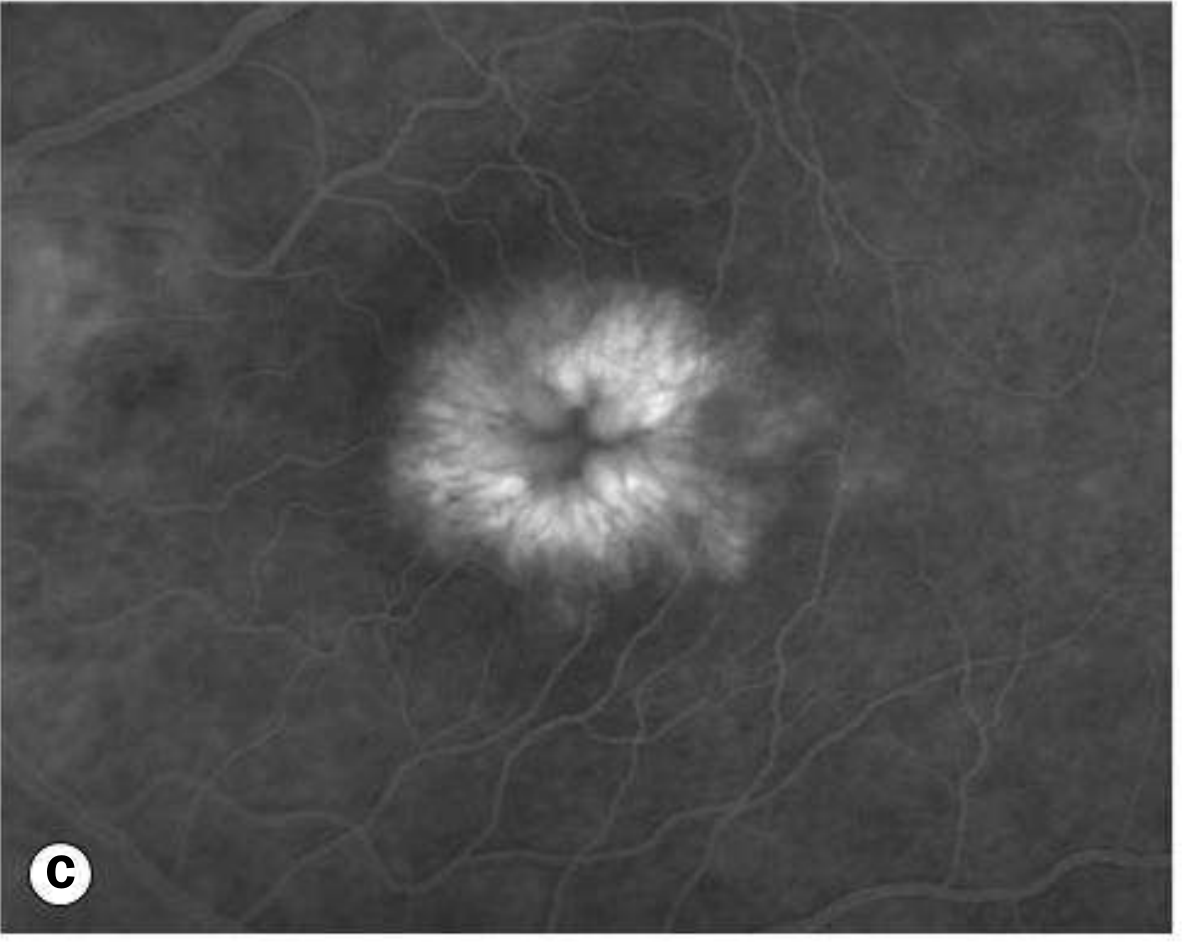
- Early phase: leakage from perifoveal capillaries
- Late phase: classic "flower-petal" (petaloid) pattern of hyperfluorescence — dye accumulates in microcystic spaces in the OPL arranged around the fovea
- Optic nerve head leakage in Irvine-Gass syndrome
- No fluorescein leakage in pseudo-CME (X-linked retinoschisis, nicotinic acid maculopathy)
3. Optical Coherence Tomography (OCT) — Gold Standard
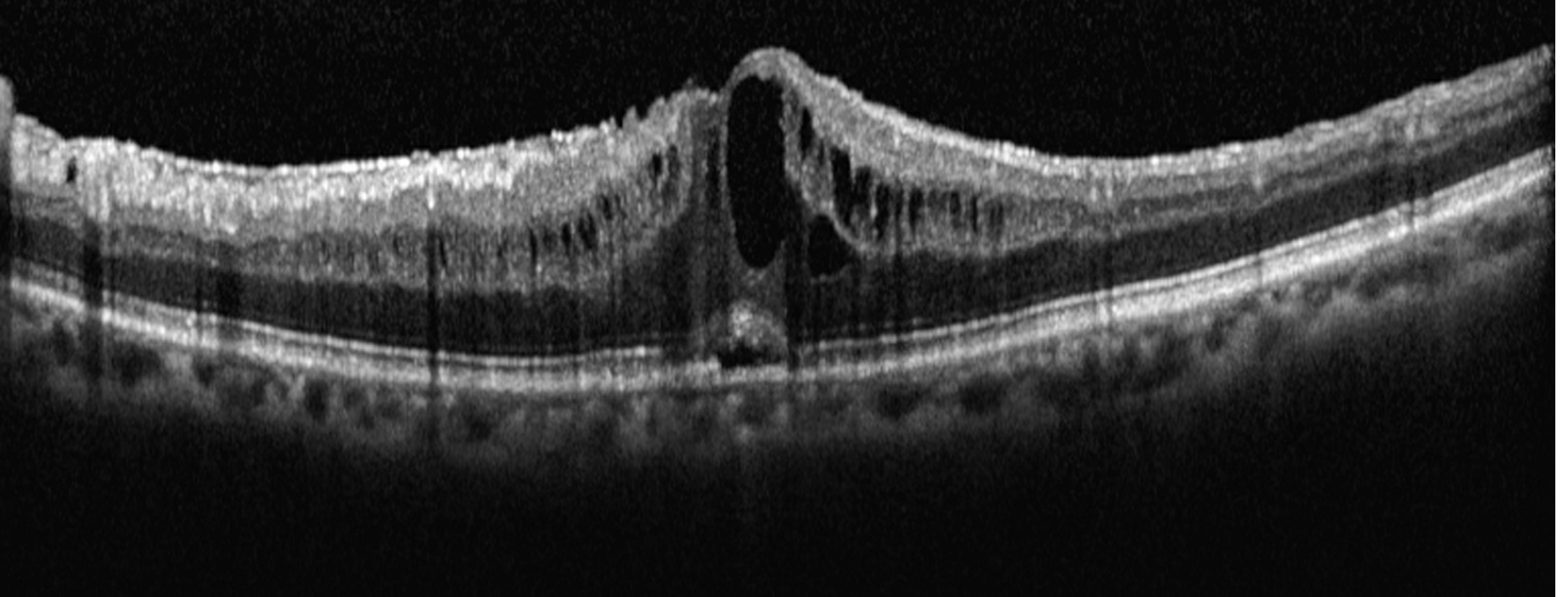
- Retinal thickening with cystic hyporeflective spaces (dark lacunae)
- Loss of the foveal depression (flat or dome-shaped foveal profile)
- Can quantify macular thickness and monitor treatment response
- May demonstrate lamellar hole in advanced cases
4. Other
- Amsler grid: central blurring and distortion
- ERG may be abnormal in RP-associated CME
- Fasting blood glucose / HbA1c for diabetic aetiology
Differential Diagnosis
| Condition | Key Differentiating Feature |
|---|---|
| Central serous chorioretinopathy | Subretinal fluid (not intraretinal cysts); smoke-stack on FA |
| X-linked retinoschisis | No FA leakage (pseudo-CME); spoke-wheel on OCT |
| Macular hole | Full-thickness defect on OCT; Watzke-Allen sign |
| Subfoveal CNV (wet AMD) | Subretinal fluid, haemorrhage; CNV membrane on FA |
| Nicotinic acid maculopathy | Drug history; no FA leakage |
| Myopic foveal schisis | High myopia; no FA leakage |
Treatment
General principle: treat the underlying cause.
Step 1 — Address Causative Factors
- Discontinue topical prostaglandin analogues, epinephrine, dipivefrin, or nicotinic acid
- Vitrectomy/YAG laser lysis of vitreous wick if present (Irvine-Gass with vitreous traction)
- Control diabetes, manage uveitis
Step 2 — Topical Therapy (first-line for post-surgical CME)
| Drug | Dose |
|---|---|
| Topical NSAIDs — ketorolac 0.5% | QID |
| Bromfenac 0.09% | BD |
| Nepafenac 0.3% | Daily |
| Topical steroids — prednisolone acetate 1% | QID (combined with NSAIDs) |
Step 3 — Periocular / Intravitreal Injections
- Sub-Tenon triamcinolone 40 mg/mL (0.5–1 mL)
- Intravitreal triamcinolone 1–4 mg
- Intravitreal anti-VEGF (bevacizumab 1.25 mg) — especially for diabetic/RVO-related CME
- Intravitreal dexamethasone implant (Ozurdex 0.7 mg)
- Intravitreal ranibizumab / aflibercept for diabetic macular oedema and RVO
Step 4 — Systemic Therapy
- Systemic steroids — prednisolone 40 mg/day for 5 days, then taper
- Systemic NSAIDs — indomethacin 25 mg TID × 6 weeks
- Carbonic anhydrase inhibitors (CAIs) — dorzolamide 2% TID topically or acetazolamide 500 mg PO (particularly useful in RP-related CME and uveitic CME)
Step 5 — Surgical
- Pars plana vitrectomy — for tractional CME (ERM, VMT), refractory cases, or vitreous wick incarceration
- Grid laser photocoagulation — for diabetic macular oedema (largely superseded by anti-VEGF)
Complications
- Foveal lamellar hole — from coalescence of cystic spaces → irreversible visual loss
- Chronic CME → photoreceptor atrophy → permanent central scotoma
- Secondary epiretinal membrane formation
Key Points for Exam
| Point | Detail |
|---|---|
| Most common cause | Diabetic retinopathy (globally); Irvine-Gass (post-cataract) |
| Characteristic FA finding | Petaloid / flower-petal pattern of late hyperfluorescence |
| Investigation of choice | OCT (non-invasive, quantitative) |
| Layers involved | Outer plexiform layer + inner nuclear layer |
| Unique feature of Irvine-Gass | Optic disc leakage on FA |
| Pseudo-CME | No FA leakage — key differentiator |
| First-line treatment (post-op) | Topical NSAIDs ± steroids |
| Anti-VEGF use | Diabetic macular oedema + RVO-related CME |
| CAI use | RP-related and uveitic CME |
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed. | The Wills Eye Manual, 8th ed.
This is a shared conversation. Sign in to Orris to start your own chat.