Mastoidectomy
Reading File
Finding Sources
Finding Sources
Searching PubMed
"mastoidectomy"[MeSH Terms] AND "outcomes"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Now I have comprehensive content to write a thorough answer on mastoidectomy.
Mastoidectomy
Definition
Mastoidectomy is a surgical procedure involving the removal of the mastoid cortex and air cell system of the temporal bone. It forms the cornerstone of otologic surgery and is used to manage disease processes ranging from chronic suppurative otitis media and cholesteatoma to cochlear implantation and skull base tumors.
Cummings Otolaryngology Head and Neck Surgery, p. 2741
Surgical Anatomy
The mastoid bone is the posterior part of the temporal bone. Key surface landmarks include:
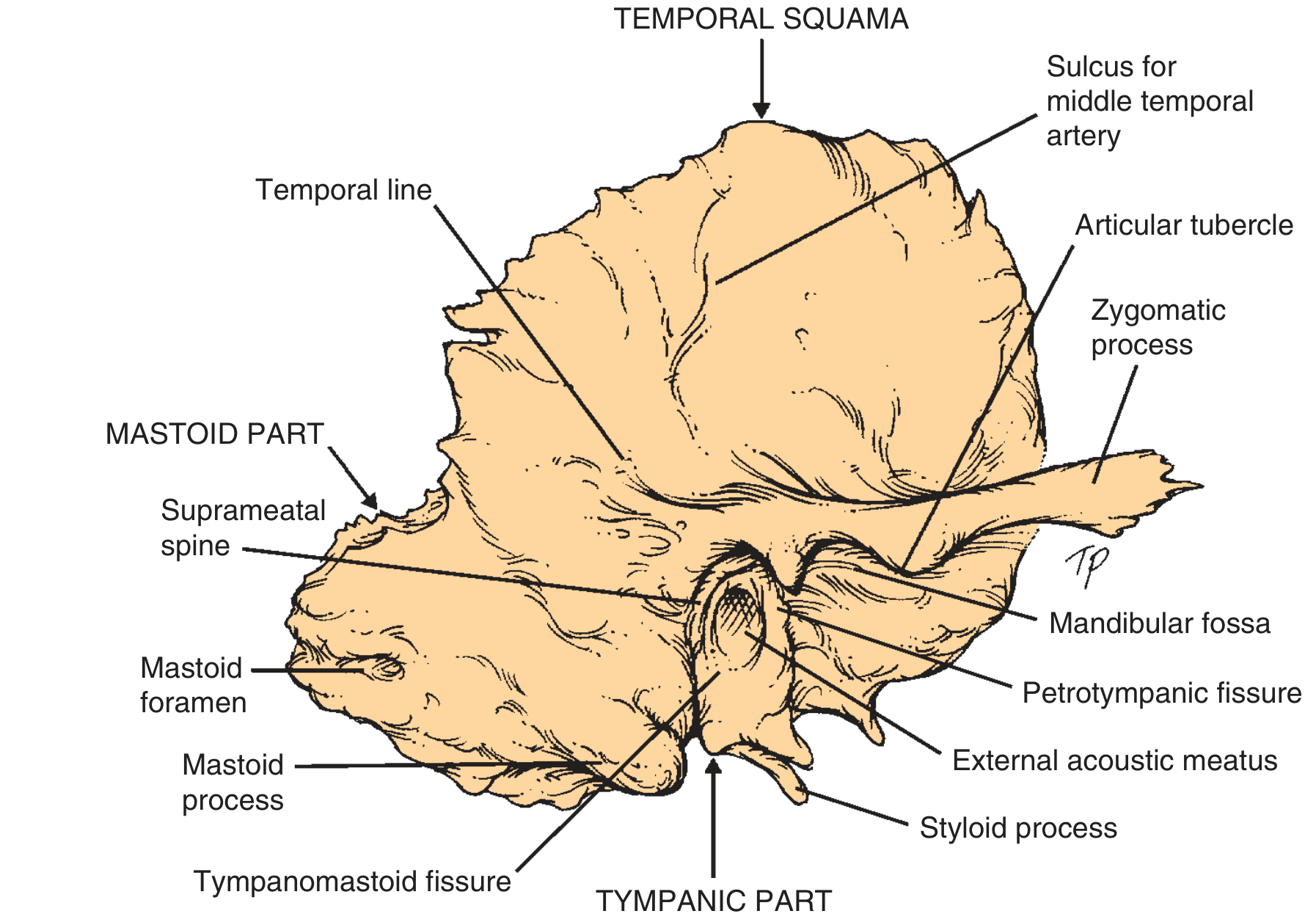
Fig. 143.1 Right temporal bone, lateral view - Cummings Otolaryngology
Critical surgical landmarks during mastoidectomy:
- Temporal line - approximates the floor of the middle cranial fossa (tegmen)
- Sigmoid sinus - posterior limit of dissection
- Mastoid antrum - key landmark connecting to the middle ear via the aditus ad antrum
- Short process of the incus and dome of the lateral semicircular canal - the "pointer" to the facial nerve
- Facial nerve (mastoid segment) - runs from the second genu downward through the stylomastoid foramen; must be identified and protected
- Digastric ridge - inferior landmark for the descending facial nerve
- Facial recess - bounded laterally by the chorda tympani, medially by the facial nerve, superiorly by the fossa incudis
Indications (Box 143.1)
| Category | Examples |
|---|---|
| Chronic ear disease | Chronic otitis media, cholesteatoma |
| Acute infection | Acute suppurative mastoiditis, subperiosteal abscess, coalescent mastoiditis |
| Facial nerve | Idiopathic (Bell's palsy) or traumatic facial nerve palsy |
| Vestibular | Meniere's disease (endolymphatic sac decompression), BPPV (posterior canal occlusion), superior canal dehiscence syndrome, vestibular neurectomy |
| Skull base | Cerebellopontine angle tumors, petrous apex cholesterol granuloma |
| CSF leak | Spontaneous CSF leak, encephaloceles |
| Implants | Cochlear implantation, auditory brainstem implant (translabyrinthine) |
| Malignancy | Temporal bone / parotid malignancy resection |
Nomenclature
The terminology for mastoid surgery is notoriously confusing. The standard procedures are:
| Procedure | Key Feature |
|---|---|
| Simple mastoidectomy | Removes cortex + limited air cells; used for acute mastoiditis drainage |
| Canal wall-up (CWU) / intact canal mastoidectomy | Complete air cell exenteration while preserving the bony EAC wall |
| Canal wall-down (CWD) mastoidectomy | Removes superior and posterior canal walls; creates an open mastoid bowl |
| Radical mastoidectomy | CWD + removal of tympanic membrane, ossicles, and posterior EAC wall; no attempt at hearing preservation |
| Modified radical (Bondy) mastoidectomy | Epitympanic cholesteatoma exteriorized; uninvolved middle ear left intact; matrix maintained as cavity lining |
| Mastoid obliteration | Mastoid cavity filled with autogenous or alloplastic material |
| Canal reconstruction mastoidectomy | Temporary removal of bony EAC, then reconstruction after disease clearance |
| Retrograde mastoidectomy | Disease approached from the tympanum working posteriorly into the mastoid |
Cummings Otolaryngology, Box 143.2, p. 2742
Surgical Technique (Canal Wall-Up)
Steps (Box 143.3)
- Incision: C-shaped postauricular incision ~1 cm behind the postauricular crease; inject 1% lidocaine with 1:100,000 epinephrine
- Exposure: Two periosteal incisions (along temporal line + perpendicular to mastoid tip) to fully expose the mastoid cortex
- First burr cuts: Along the temporal line and tangential to the EAC posteriorly
- Antrum identification: Remove mastoid cortex to identify the antrum (largest mastoid air cell, directly posterior to the EAC)
- Key landmark identification: Tegmen (superiorly), sigmoid sinus (posteriorly)
- Exenteration: Remove all mastoid air cells between these boundaries
- Thinning the canal wall: Thin the posterior and superior EAC walls to improve visualization
- Identify incus and lateral SCC: The short process of the incus and dome of the lateral semicircular canal are consistent "pointers" to the facial nerve
- Facial nerve skeletonization: The mastoid segment is identified running from the second genu to the stylomastoid foramen
- Facial recess opening (posterior tympanotomy): The triangle bounded by chorda tympani (laterally), facial nerve (medially), and fossa incudis (superiorly) is opened - provides access to the round window, promontory, IS joint, eustachian tube orifice
- Epitympanum opening: Required for cholesteatoma tracking to the ossicular heads/supratubal recess; requires removal of incus remnant/malleus head if eroded
Note: Continuous facial nerve monitoring is standard for CWU mastoidectomy and all subsequent complex procedures.
Canal Wall-Down Mastoidectomy
Involves thorough removal of all mastoid air cells + aggressive saucerization of cortical edges + complete removal of the superior and posterior canal walls + meatoplasty. The tympanic membrane is usually reconstructed. This creates an open "mastoid bowl" that is continuous with the EAC.
CWU vs CWD: Comparative Considerations
| Feature | Canal Wall-Up | Canal Wall-Down |
|---|---|---|
| Anatomy preserved | Yes | No |
| Residual cholesteatoma rate | Higher (~42% pediatric) | Lower (~12% pediatric) |
| Postop monitoring of disease | Requires second-look surgery | Direct visualization in clinic |
| Healing time | Faster | Slower (months of epithelialization) |
| Water exposure tolerance | Good | Problematic |
| Hearing aid use | Well tolerated | Increased infection risk |
| Long-term bowl maintenance | Not needed | May need regular debridements |
| Hearing outcomes | Similar | Similar |
Indications for CWD over CWU:
- Only-hearing ear (single surgery preferred)
- Poor anesthetic risk
- Unreliable follow-up
- Low-lying tegmen + anterior sigmoid sinus (small cavity limits access)
- Horizontal SCC (HSCC) fistula with extensive bone erosion
- Deep sinus tympani (inaccessible via facial recess alone)
Cummings Otolaryngology, p. 2745-2746
Variant Techniques
Modified Radical (Bondy) Mastoidectomy
Specifically for cholesteatoma limited to the epitympanum. The superior/posterior canal wall over the epitympanum is removed to exteriorize the disease. The middle ear proper is not entered, and the cholesteatoma matrix is preserved as a lining. Unlike retrograde mastoidectomy, the canal and tympanic membrane defects are not repaired.
Mastoid Obliteration
Various materials used: autogenous bone/cartilage, free or vascularized soft tissue, bioactive glass (S53P4 - subject of a 2026 meta-analysis), or other alloplastic materials. Used as primary procedure or at second-look surgery.
Canal Reconstruction Mastoidectomy
Developed by Gantz et al. The bony EAC wall is temporarily removed using microsagittal saw cuts, disease is cleared, and the canal wall is then replaced in its native position (with mitered locking cuts). Cortical bone chips block the epitympanum and facial recess. The mastoid is then obliterated with bone pate. Benefits: CWD-level exposure during surgery + canal wall-up benefits postoperatively (no bowl, water tolerance).
Retrograde Mastoidectomy
Approaches cholesteatoma from the tympanum working posteriorly. Described by Dornhoffer as involving temporary upper canal wall removal followed by reconstruction.
Endoscopic-Assisted Mastoidectomy
Rigid endoscopes (including 45-degree scopes) provide visualization of recesses (sinus tympani, facial recess, anterior epitympanum) inaccessible to the straight microscope. However, endoscopy does not reduce cholesteatoma recidivism rates following primary surgery.
Complications
| Complication | Notes |
|---|---|
| Facial nerve injury | Most feared; continuous intraoperative monitoring is standard |
| Hearing loss (sensorineural) | Drill heat/vibration transmitted to inner ear; irrigation and diamond burrs near ossicles |
| Perilymph fistula / labyrinthine fistula | Semicircular canal erosion by cholesteatoma; managed by keeping matrix intact over fistula in some cases |
| Sigmoid sinus injury | Venous bleeding; controlled with Surgicel/pressure |
| Dural breach / CSF leak | Middle cranial fossa or posterior fossa dura |
| Chorda tympani injury | Taste disturbance, dry mouth |
| Meningitis | Rare but serious |
| Residual / recurrent cholesteatoma | Leading cause of surgical failure |
| Mastoid bowl problems | Chronic discharge, granulations, water intolerance (CWD cavities) |
Key Historical Notes
- Ambrose Pare (16th century): Proposed drainage for King Charles II (operation refused; king died)
- Jean Petit (late 1700s): First successful mastoid trephination
- Sir William Wilde (1853): First postauricular incision
- Schwartz & Eysell (1873): Reintroduced cortical mastoidectomy for acute infections
- Zaufal (1890): Described the radical mastoidectomy (removal of TM, ossicles, posterior canal wall)
- Bondy (early 1900s): Modified radical procedure preserving the middle ear
Shambaugh Surgery of the Ear, p. 1772-1786
Sources
- Cummings Otolaryngology Head and Neck Surgery, Ch. 143, pp. 2741-2749
- Shambaugh Surgery of the Ear, Ch. on Mastoid Surgery, pp. 1751-1790
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 2, Ch. 103
Recent literature note: A 2026 systematic review and meta-analysis (PMID 41940705) evaluated mastoid obliteration using S53P4 bioactive glass granules - this represents an active area of current research into obliteration materials for canal-down cavities.
This is a shared conversation. Sign in to Orris to start your own chat.