
photo-1783871930142.jpg
Answer ths questions
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
I now have comprehensive information to answer both questions fully. Let me compile the answers.
Question 1: Blood Supply of the Femoral Head (Adult & Child) + Garden Type I and Type III NOF Fracture
Blood Supply of the Femoral Head
In the Adult
The blood supply reaches the femoral head via three sources (in order of importance):
-
Medial Femoral Circumflex Artery (MFCA) - the dominant supply. Its deep branch runs around the base of the femoral neck, travels as retinacular (capsular) vessels along the femoral neck, and terminates as multiple superior retinacular arteries penetrating the femoral head. The MFCA contributes approximately 82% of femoral head perfusion. Its branches are arranged into four groups - lateral, medial, anterior, and posterior - of which the lateral group is the largest contributor.
-
Lateral Femoral Circumflex Artery (LFCA) - provides the anterior nutrient artery to the femoral neck, contributing approximately 18% of femoral head perfusion. Its contribution to the femoral head itself is relatively minor.
-
Artery of the Ligamentum Teres - a branch of the obturator artery (or MFCA). It is small and variable in adults, and generally insufficient alone to maintain viability of the entire femoral head after a displaced fracture.
An additional contributor - the inferior gluteal artery - anastomoses with the MFCA along the inferior border of piriformis and may become compensatory after MFCA injury.
The retinacular vessels are most vulnerable in displaced subcapital fractures, as displacement tears these vessels, risking AVN.
In the Child
In children, the blood supply pattern differs significantly - this is why pediatric neck of femur fractures (and conditions like Perthes disease) are so devastating:
- The physis (growth plate) acts as a barrier - vessels cannot cross it freely
- The artery of the ligamentum teres is more prominent and contributes significantly in young children (unlike in adults where it is minor)
- The retinacular vessels from MFCA still run along the neck but must pass around the growth plate, making them more vulnerable
- The metaphyseal vessels contribute through the neck but are blocked from crossing the open physis into the epiphysis
- In very young children, the epiphysis is supplied almost entirely by vessels coursing around the periphery of the femoral neck (largely the MFCA retinacular branches)
As the child ages and the physis begins to close, the adult pattern of supply gradually takes over. This explains why Legg-Calve-Perthes disease (avascular necrosis of the femoral head in children) results from an unknown blockage in this precarious supply.
Garden Classification of Neck of Femur Fractures
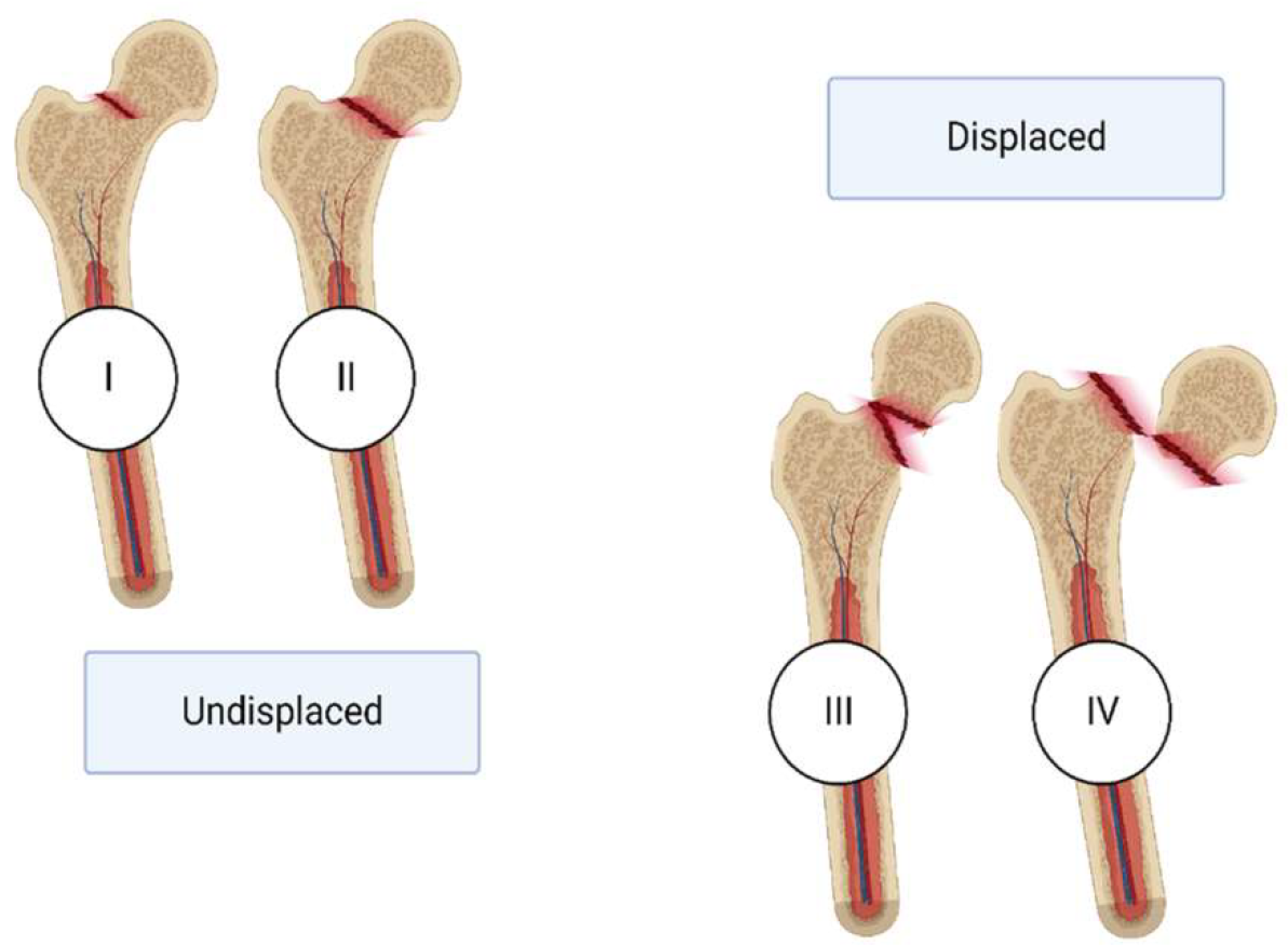
| Stage | Description | Simplified |
|---|---|---|
| Garden I | Incomplete or impacted fracture in valgus | Undisplaced |
| Garden II | Complete fracture without displacement - fragments align anatomically | Undisplaced |
| Garden III | Complete fracture with partial displacement - angulated/rotated but not fully out of alignment | Displaced |
| Garden IV | Fully displaced fracture - complete loss of anatomical alignment | Displaced |
Garden Type I
- An incomplete or valgus-impacted fracture of the femoral neck
- The trabecular pattern of the femoral head appears continuous on X-ray (head appears in slight valgus)
- The fracture is stable - the lateral cortex remains intact and acts as a hinge
- Carries the lowest risk of AVN among the four types
- Union rate approaches 100%
- Conservative/minimally invasive fixation (cannulated screws) is often adequate
Garden Type III
- A complete fracture with partial displacement - the femoral head is rotated or angulated, but NOT completely separated
- On X-ray, the trabecular pattern of the head does not align with that of the acetabulum (unlike Type IV where the head "self-reduces" to align with the acetabulum)
- The retinacular vessels are significantly compromised, leading to substantial AVN risk
- Union rate approximately 93% but with much higher failure and AVN risk than Types I/II
- Requires operative fixation (younger patients) or arthroplasty (elderly)
Question 2: Management of NOF in a 30-Year-Old Male, 3 Hours Post-Injury + Complications + Pauwels Classification
Management of NOF Fracture in a 30-Year-Old (Young Adult), Presenting at 3 Hours
In a young, active 30-year-old male, the priority is head preservation - arthroplasty is generally avoided because of the long life expectancy and desire for native joint function.
Initial Steps
- Emergency workup: ATLS protocol if high-energy trauma (common cause in young adults - MVA, fall from height), assess neurovascular status of the limb
- Imaging: AP pelvis, cross-table lateral hip X-ray; CT may be needed to characterize fracture pattern
- Classify the fracture: Garden stage and Pauwels angle are assessed
Surgical Management (Goal: Urgent Reduction and Internal Fixation)
Since the patient presented at 3 hours post-injury (well within the "golden period"), urgent operative intervention is indicated:
- Emergency closed reduction (or open reduction if closed fails) followed by internal fixation with cannulated cancellous screws - usually 3 screws placed in an inverted triangle configuration. This is the standard operation for young adults.
- Dynamic Hip Screw (DHS) - preferred for more vertical (Pauwels Type III / basicervical) fractures where shear forces require more rigid fixation
- The short time from injury is critical: early decompression (capsulotomy) and reduction minimize the tamponade effect on the retinacular vessels and may reduce AVN risk
Most Common Serious Complication: Avascular Necrosis (AVN) of the Femoral Head
AVN is the most feared complication in a young patient with a displaced neck of femur fracture. The mechanism is:
- Mechanical disruption of the retinacular vessels by the fracture/displacement
- Tamponade effect from elevated intracapsular haematoma pressure, compressing vessels
- Rotational displacement disrupting the ligamentum teres vessels
AVN may present months to years after fracture fixation with pain, collapse, and arthritis.
Two Operations to Manage AVN of the Femoral Head (in a young patient):
-
Free Vascularized Fibula Graft (VFBG)
- Preferred in early-stage AVN (pre-collapse)
- A segment of fibula with its peroneal artery and vein is harvested and implanted into the femoral head through a core decompression tunnel
- It provides mechanical support AND a new blood supply to the necrotic head
- Aims to prevent collapse and preserve the native femoral head
-
Total Hip Arthroplasty (THA)
- Indicated when AVN has progressed to femoral head collapse and secondary arthritis (late-stage disease, Ficat Stage III-IV)
- In young patients, this is considered a last resort due to implant longevity concerns (revision surgery likely in their lifetime)
- Modern uncemented THA with advanced bearings (ceramic-on-ceramic) is used to minimize wear
Other options (not first-choice for a 30-year-old) include core decompression (early stage), and various osteotomies (e.g., transtrochanteric rotational osteotomy - Sugioka procedure) to rotate the necrotic segment away from the weight-bearing zone.
Pauwels Classification of Neck of Femur Fractures - Clinical Significance
Introduced by Friedrich Pauwels, this system classifies NOF fractures based on the angle of the fracture line from the horizontal on an AP radiograph:
| Type | Angle from Horizontal | Dominant Force at Fracture Site | Stability |
|---|---|---|---|
| Type I | < 30° | Predominantly compressive | Most stable |
| Type II | 30° - 50° | Mixed compressive and shear | Intermediate |
| Type III | > 50° (near vertical) | Predominantly varus and shearing | Least stable - highest risk |
Clinical Significance
- Type I (horizontal fracture) - compressive forces tend to impact the fracture, promoting union. May be amenable to less aggressive fixation.
- Type III (vertical fracture) - shear forces act across the fracture line, resisting union and making standard cannulated screw fixation inadequate. These fractures have a higher rate of non-union and fixation failure and may require a dynamic hip screw or fixed-angle device (e.g., proximal femoral locking plate) to resist the shear forces.
- The Pauwels angle thus guides the choice of implant - the more vertical the fracture, the stronger the fixation required.
Limitations: Pauwels classification has relatively poor interobserver reliability (kappa ~0.46) compared to Garden's (~0.76), and its clinical predictive value for union vs. non-union has been questioned by Parker et al., who found no statistically significant difference in Pauwels angles between united and non-united fractures.
Sources: Rockwood and Green's Fractures in Adults 10th ed. 2025 | Gray's Anatomy for Students | Campbell's Operative Orthopaedics 15th ed. 2026 | Osteosynthesis, Hemiarthroplasty, Total Hip Arthroplasty (Textbook) | Grainger & Allison's Diagnostic Radiology
This is a shared conversation. Sign in to Orris to start your own chat.