DVT approach
Reading File
Finding Sources
Finding Sources
Searching PubMed
"deep vein thrombosis" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have everything I need for a comprehensive DVT approach. Here is the full structured answer:
Deep Vein Thrombosis (DVT) - Clinical Approach
Anatomy
DVT involves thrombosis of the deep venous system. Key veins at risk (proximal to distal):
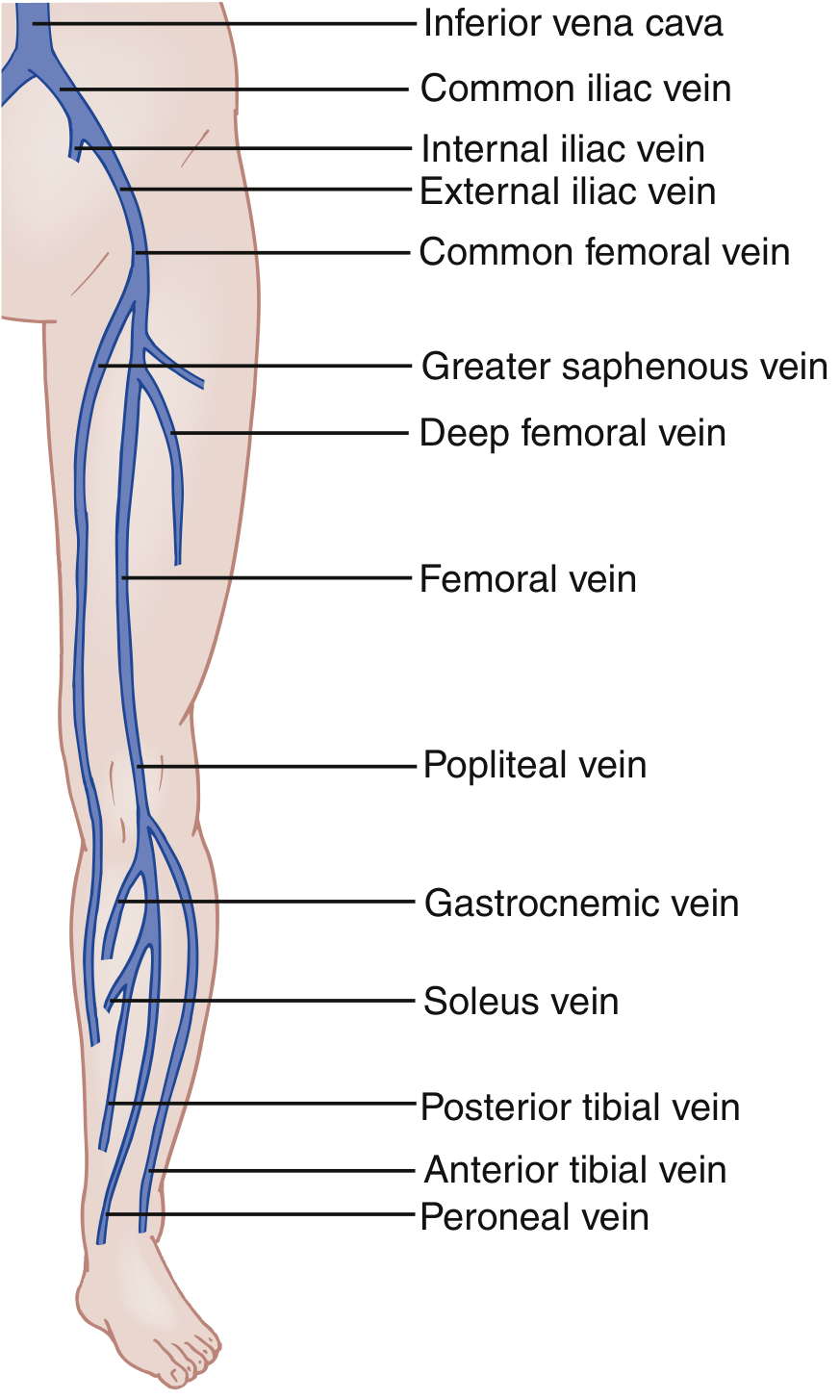
Leg vein anatomy. A 3-point ultrasound covers common femoral, femoral, and popliteal veins. Whole-leg US adds the saphenous, posterior tibial, peroneal, and gastrocnemius veins.
- Proximal DVT: common femoral, femoral, popliteal - higher PE risk
- Distal (calf) DVT: posterior tibial, peroneal, anterior tibial, gastrocnemius, soleus veins
Pathophysiology - Virchow's Triad
- Venous stasis - immobility, prolonged travel, bed rest, cardiac failure
- Endothelial injury - surgery, trauma, catheter insertion
- Hypercoagulable state - malignancy, pregnancy, thrombophilia (Factor V Leiden, antiphospholipid syndrome, protein C/S deficiency), oral contraceptive use
Clinical Features
Symptoms and signs are often subtle and nonspecific:
- Unilateral limb pain, swelling, warmth, erythema
- Tenderness along the deep venous distribution
- Dilation of superficial collateral veins
- Rarely a palpable venous cord
- Homans' sign (calf pain on dorsiflexion): neither sensitive nor specific - not reliable
- Bilateral DVT is found in <10% of patients
Upper extremity DVT: >90% occur with an indwelling catheter. Without a device, think Paget-Schroetter syndrome (effort-induced thoracic outlet syndrome in young athletes). - Rosen's Emergency Medicine, p. 1196
Differential Diagnosis
| Condition | Key Distinguishing Feature |
|---|---|
| Venous insufficiency | Chronic, bilateral, history of varicosities |
| Cellulitis | Concurrent DVT only ~3%; fever more prominent |
| Baker cyst (ruptured) | Posterior knee fullness, history of knee disease |
| Muscle/tendon injury | History of trauma or exertion |
| Calf hematoma | Sudden onset, no fever |
| Asymmetric edema (CHF) | Bilateral, responds to diuresis |
| Arterial insufficiency/claudication | Exertional, absent pulses |
Step 1: Pretest Probability - Wells Score for DVT
| Clinical Feature | Points |
|---|---|
| Active cancer (treated within 6 months or palliative) | +1 |
| Paralysis, paresis, or recent plaster immobilization of lower extremities | +1 |
| Recently bedridden ≥3 days or major surgery within 12 weeks | +1 |
| Localized tenderness along the deep venous system | +1 |
| Entire leg swollen | +1 |
| Calf swelling ≥3 cm larger than asymptomatic side (measured 10 cm below tibial tuberosity) | +1 |
| Pitting edema confined to the symptomatic leg | +1 |
| Collateral superficial veins (non-varicose) | +1 |
| Previously documented DVT | +1 |
| Alternative diagnosis at least as likely as DVT | -2 |
Score <2 = Low probability | Score ≥2 = Intermediate/High probability
- Bailey & Love's Surgery 28th Ed, p. 345
Step 2: Diagnostic Algorithm
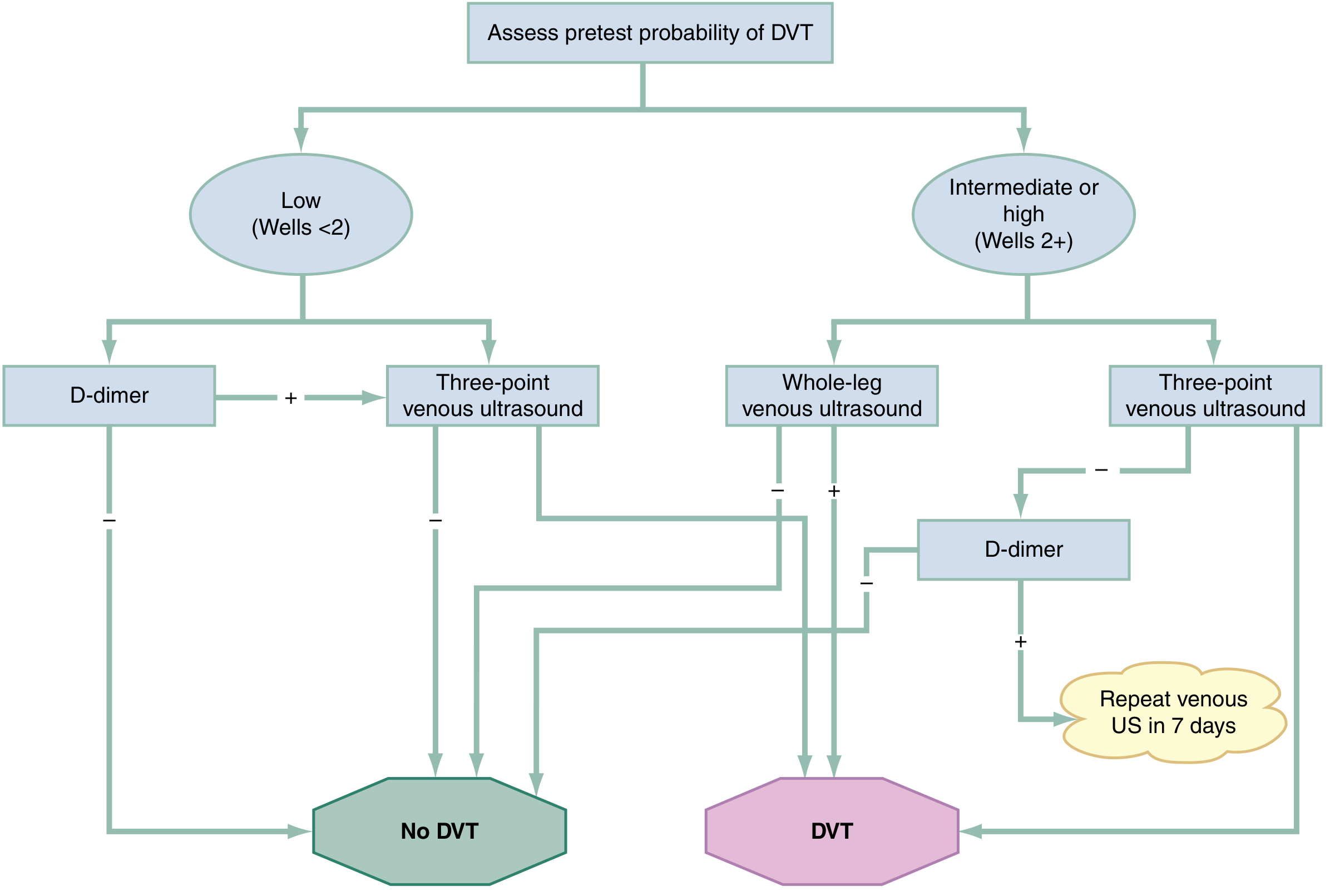
Low probability (Wells <2):
- Send D-dimer
- Negative D-dimer → DVT excluded, no imaging needed
- Positive D-dimer → 3-point venous ultrasound (CFV, femoral, popliteal)
Intermediate/High probability (Wells ≥2):
- Go directly to imaging (do not rely on D-dimer alone)
- Whole-leg ultrasound preferred (adds distal veins)
- OR 3-point ultrasound + D-dimer:
- Negative US + negative D-dimer → DVT excluded
- Negative US + positive D-dimer → repeat US in 7 days (to catch distal DVT that may propagate)
D-dimer Caveats
D-dimer is highly sensitive but not specific. False positives occur with:
- Pregnancy, postpartum
- Active malignancy
- Advanced age
- Recent surgery (within 1 month)
- Rheumatologic disease (SLE, RA)
- Sickle cell disease, hemodialysis
Note: Warfarin use can cause false-negative D-dimer results. - Rosen's Emergency Medicine, p. 1199
Imaging
- Compression ultrasound: first-line; incompressibility of the vein is diagnostic
- MRI venography: when iliac/IVC thrombus suspected or US inconclusive
- CT venography: combined with CT-PA when PE also suspected
Step 3: Management
Anticoagulation - First-line
Initiate as soon as diagnosis confirmed (or while awaiting imaging if high pretest probability).
| Anticoagulant | Initial Dose | Key Restriction |
|---|---|---|
| Rivaroxaban (preferred DOAC) | 15 mg PO BID x21 days, then 20 mg OD | CrCl <30 mL/min - avoid |
| Apixaban (preferred DOAC) | 10 mg PO BID x7 days, then 5 mg BID | CrCl <25 mL/min - avoid |
| Dabigatran | 150 mg BID (after 5-10 days LMWH) | CrCl <30 - avoid |
| Enoxaparin (LMWH) | 1 mg/kg SC q12h or 1.5 mg/kg q24h | CrCl <30 - reduce dose/avoid |
| Fondaparinux | 5-10 mg SC once daily | CrCl <30 - avoid; no HIT risk |
| UFH | 70-80 U/kg bolus, then 17-18 U/kg/h IV | Use in renal failure, pregnancy, high-risk PE |
| Warfarin | Bridge with LMWH/UFH; target INR 2-3 | Requires monitoring; many drug interactions |
DOACs (rivaroxaban, apixaban) are first-choice for most DVT patients - they do not require LMWH bridging, have fewer bleeding complications (especially intracranial), and need no monitoring. - Rosen's Emergency Medicine, p. 1199
Special situations:
- Pregnancy: DOACs contraindicated - use LMWH throughout
- Active cancer: LMWH traditionally preferred; DOACs also shown safe and effective
- Severe renal failure (CrCl <30): use UFH IV
- Antiphospholipid antibody syndrome: warfarin (DOACs may have higher recurrence rate)
- Liver failure: DOACs and LMWH may be contraindicated
Duration of Anticoagulation
| Situation | Duration |
|---|---|
| First DVT - provoked (transient risk factor, e.g. post-surgery) | 3 months |
| First DVT - unprovoked | ≥3 months; consider indefinite |
| Recurrent DVT | Indefinite |
| Active malignancy | Indefinite or until cancer resolved |
| Antiphospholipid syndrome | Indefinite |
Isolated Distal (Calf) DVT
Controversial. ~15% propagate proximally without treatment.
- Favor anticoagulation if: ongoing risk (cancer, immobility), severe symptoms, clot >5 cm, close to popliteal, prior VTE
- Favor surveillance (serial US in 7 days) if: high bleeding risk, no propagation risk factors
- A 2025 meta-analysis (PMID: 40400471) specifically addressed anticoagulation for isolated distal DVT - evidence supports treatment in high-risk patients
IVC Filter
- Reserved for patients who cannot be anticoagulated (active bleeding, very high bleeding risk)
- Temporary/retrievable filters preferred; retrieve once anticoagulation is safe
- Does NOT replace anticoagulation when it can be used
Endovascular Intervention (Catheter-Directed Thrombolysis / Mechanical Thrombectomy)
- Consider for iliofemoral DVT with high clot burden
- Aim: reduce post-thrombotic syndrome (PTS)
- Required for phlegmasia cerulea/alba dolens - a limb-threatening emergency:
- Massive iliofemoral occlusion → entire limb swollen, cyanotic
- May have associated arterial spasm (phlegmasia alba dolens = painful pale leg)
- Treat urgently with CDT, percutaneous thrombectomy, or surgical thrombectomy
- Transfer immediately if intervention not available - Bailey & Love's Surgery 28th Ed.
Step 4: Bleeding Risk Assessment
Use VTE-BLEED Score to guide duration decisions:
| Factor | Points |
|---|---|
| Active cancer | 2 |
| Male with uncontrolled hypertension | 1 |
| Anemia | 1.5 |
| History of bleeding | 1.5 |
| Renal dysfunction (CrCl 30-60 mL/min) | 1.5 |
| Age ≥60 years | 1.5 |
High score (≥2) = high bleeding risk - shorter duration or surveillance strategy preferred.
Absolute contraindications to anticoagulation include active intracranial bleeding, recent CNS surgery, large aortic aneurysm with severe hypertension, and stable aortic dissection. - Rosen's Emergency Medicine
Step 5: Additional Considerations
Thrombophilia Workup
- Consider after unprovoked DVT, especially in young patients, recurrent events, unusual sites, or strong family history
- Test for: Factor V Leiden, Prothrombin G20210A mutation, Protein C & S deficiency, Antithrombin III, Antiphospholipid antibodies, Homocysteine
- Do NOT test during acute event or while on anticoagulation (most proteins are consumed or altered acutely)
Malignancy Screening
- Unprovoked DVT warrants age-appropriate cancer screening
- Extensive occult cancer workup (CT abdomen/pelvis) in selected cases
Superficial Vein Thrombosis (SVT)
- If involving the greater saphenous vein above the knee, risk of propagation to DVT
- If thrombus is within 3 cm of the saphenofemoral junction: treat with therapeutic-dose anticoagulation ≥30 days
- Otherwise: prophylactic-dose anticoagulation for 45 days (reduces extension and PE)
Post-Thrombotic Syndrome (PTS)
- Long-term complication of DVT: chronic pain, swelling, skin changes, venous ulceration
- Compression stockings (grade 2, 30-40 mmHg) used for ≥2 years post-DVT to reduce risk
DVT Prophylaxis (Surgical/ICU Patients)
Risk stratification by surgery type:
- High risk: pelvic surgery, hip/knee arthroplasty, major trauma
- Medium risk: abdominal, gynecological, urological surgery
- Low risk: maxillofacial, cardiothoracic, neurosurgery
Methods:
- LMWH (enoxaparin) - preferred over UFH in high-risk (orthopedic) patients; lower HIT incidence
- Graduated compression stockings (avoid if PAD, neuropathy, severe edema)
- Sequential compression devices (pneumatic pumps)
- UFH for patients with renal failure (CrCl <30)
- Harrison's Principles of Internal Medicine 22E, p. 2340
Key Sources: Rosen's Emergency Medicine, p. 1196-1201 | Bailey & Love's Short Practice of Surgery 28th Ed., p. 345 | Harrison's Principles of Internal Medicine 22E | Recent evidence: PMID 40400471 (distal DVT anticoagulation, Haematologica 2025)
This is a shared conversation. Sign in to Orris to start your own chat.