I now have everything needed for a comprehensive, well-structured NRP guide. Let me compile the full answer:
NRP Guide — Neonatal Resuscitation Program
(Per Nelson Pediatrics & AHA/AAP NRP Guidelines)
Full Algorithm at a Glance
STEP 1 — Before the Baby is Delivered: Pre-Delivery Preparation
The NRP algorithm starts before birth, not at the moment of delivery.
A. Antenatal Counseling
- Review maternal history and identify risk factors that predict a need for resuscitation
- Key questions to ask (NRP Pre-Delivery History — Box 159.3):
- What is the estimated gestational age?
- Is this a multiple gestation?
- Is meconium present in the amniotic fluid?
- Is there a history of vaginal bleeding?
- Were medications given or drugs taken by the mother?
- Was there documented maternal fever?
- Did the mother have routine prenatal care? Any abnormalities on prenatal ultrasound?
B. Team Briefing
- Designate roles before delivery — at least one qualified provider whose sole responsibility is the neonate must attend every delivery
- High-risk deliveries require a provider capable of full resuscitation including intubation
- Communicate the plan, assign tasks (airway, compressions, medications, documentation)
- NRP emphasizes simulation-based teamwork: implementation of TeamSTEPPS principles improves communication and reduces medication errors
C. Equipment & Room Temperature Check
Room temperature: Set warmer to pre-warmed setting. Hypothermia is an independent risk factor for neonatal mortality; hyperthermia risks neonatal encephalopathy.
Equipment checklist (Box 159.2):
| Category | Items |
|---|
| PPE | Gown, gloves, eye protection |
| Warmth | Blankets, plastic wrap (for preterm/omphalocele), radiant warmer |
| Airway suctioning | Bulb syringe, suction + catheters (5, 8, 10 Fr) |
| Ventilation | Self-inflating bag (450 & 750 mL), flow-inflating bag (250 & 450 mL), masks (premature/newborn/infant sizes) |
| Intubation | Laryngoscope + straight blades (00, 0, 1), ETT with stylets (2.5, 3.0, 3.5, 4 mm uncuffed), CO₂ detector, scissors + tape |
| Vascular access | Umbilical catheters (3.5 & 5 Fr), hemostats, drapes, gloves, povidone-iodine, scalpel, umbilical tape, 3-way stopcock |
| Monitoring | Timing device, pulse oximeter, cardiac monitor |
| Special | Meconium aspirator |
| Medications | Epinephrine (1:10,000), normal saline / lactated Ringer's for volume |
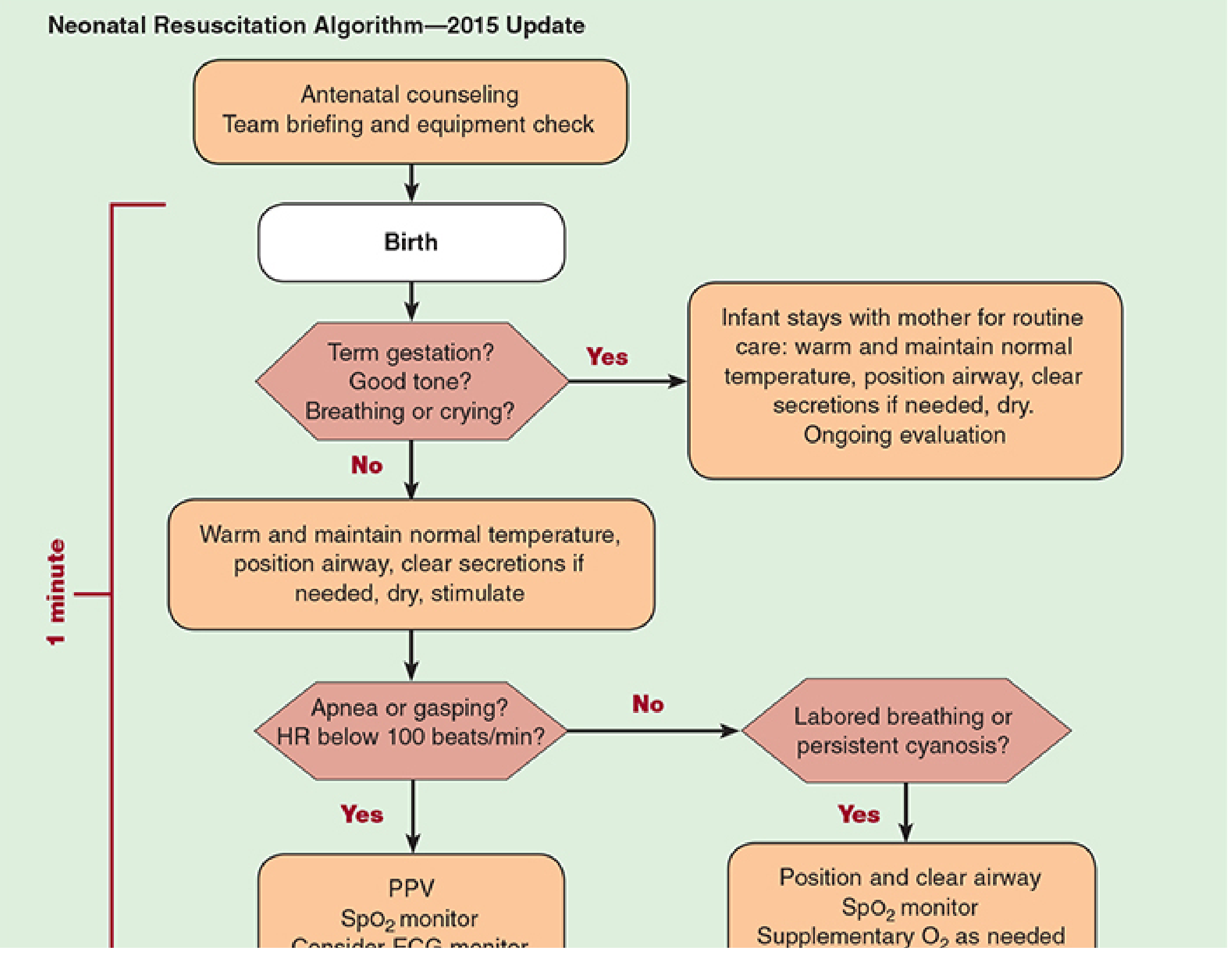
STEP 2 — At Birth: The 3 Rapid Assessment Questions
As soon as the baby is delivered, simultaneously ask:
1. Term gestation?
2. Good muscle tone?
3. Breathing or crying?
| All 3 = YES | Any 1 = NO |
|---|
| Infant stays with mother for routine care: warm & maintain temperature, position airway, clear secretions if needed, dry, ongoing evaluation | Proceed to initial steps under the warmer (Step 3) |
STEP 3 — Initial Steps (All answers NOT fully "Yes" → 60-second clock starts)
Under the radiant warmer, perform simultaneously:
- Warm and maintain normal temperature (36.5–37.5°C)
- Dry immediately; replace wet blankets with dry/warm ones
- Leave baby uncovered to facilitate radiant warming and team access
- Position the airway
- Supine, neck in slight extension (not hyperextended)
- Place a rolled towel (~1 inch) under the shoulders (not under neck) to align posterior pharynx, larynx, and trachea
- Clear secretions if needed (only if obvious obstruction, poor tone, or meconium with bradycardia)
- Suction mouth first, then nose (to prevent aspiration if baby gasps after nasal suction)
- Use ≤100 mmHg suction; avoid deep/vigorous suctioning — causes vagal bradycardia and apnea
- Dry
- Stimulate (rub back, flick soles of feet)
All of this must be completed within 1 minute ("Golden Minute").
STEP 4 — After Initial Steps: Apneic / Gasping / HR <100 bpm?
→ Begin Positive Pressure Ventilation (PPV)
- Rate: 40–60 breaths/min ("breathe-two-three, breathe-two-three")
- Initial pressures: Up to 40 cmH₂O for first breaths; thereafter ≤30 cmH₂O
- Starting O₂: Term infants — begin with 21% O₂ (room air); preterm <35 weeks — begin with 21–30% O₂
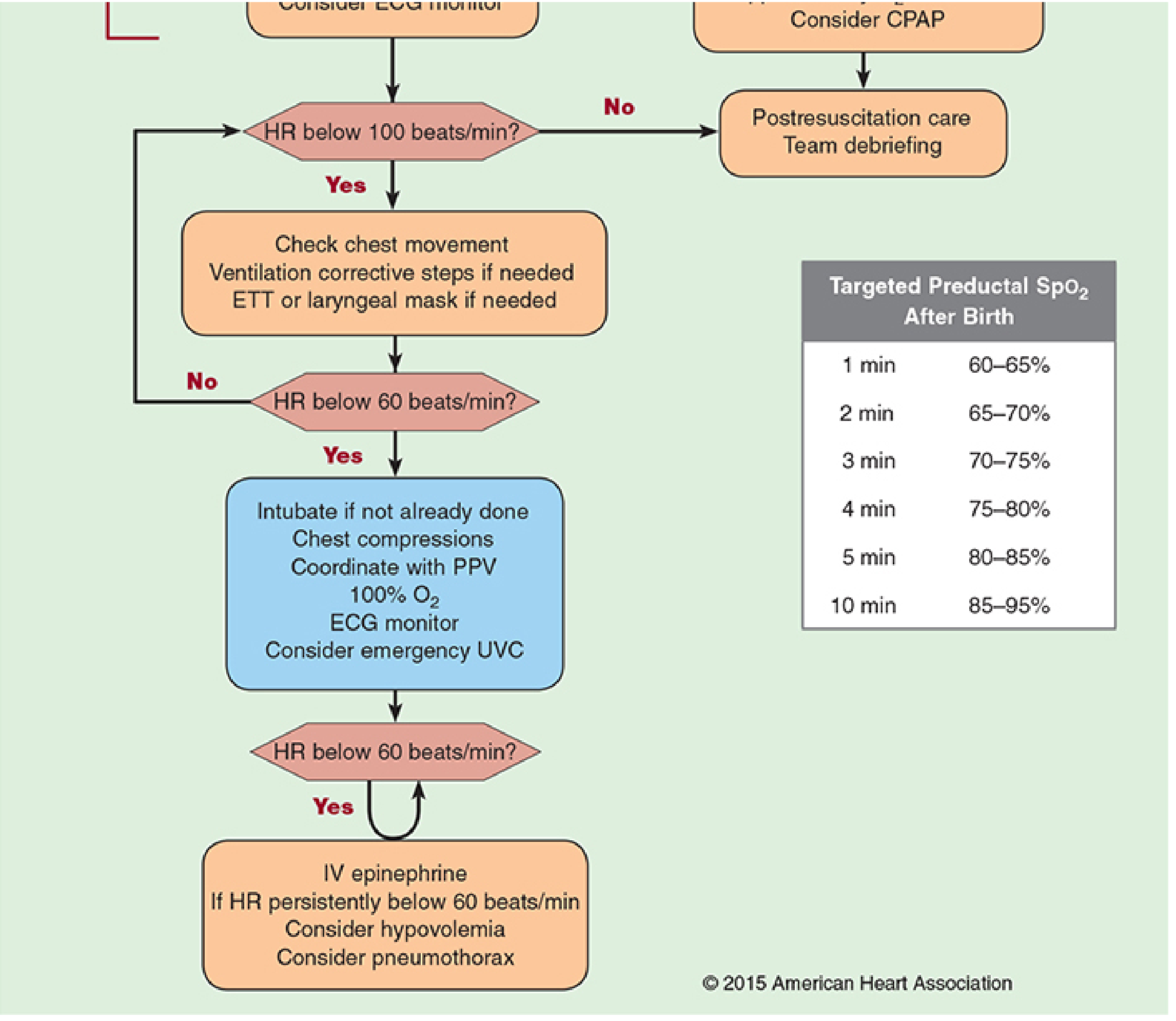
- SpO₂ monitoring: Attach pulse oximeter to the right hand or wrist (preductal) — see targeted SpO₂ table below
- Consider ECG/cardiac monitor for continuous heart rate assessment
Targeted Preductal SpO₂ After Birth:
| Time After Birth | Target SpO₂ |
|---|
| 1 min | 60–65% |
| 2 min | 65–70% |
| 3 min | 70–75% |
| 4 min | 75–80% |
| 5 min | 80–85% |
| 10 min | 85–95% |
If HR ≥100 and breathing improves → assess for labored breathing or persistent cyanosis → consider CPAP/supplemental O₂ → postresuscitation care
STEP 5 — PPV Done, but Still Apneic/Gasping and HR <100 bpm?
→ Ventilation Corrective Steps (MR. SOPA)
Check for chest rise first. If inadequate, perform corrective steps in order:
| Letter | Step |
|---|
| M | Mask adjustment — ensure tight seal, reposition mask |
| R | Reposition airway — slight neck extension, check head position |
| S | Suction mouth and nose — clear secretions |
| O | Open mouth — open slightly, consider oral airway |
| P | Pressure increase — increase PIP in small increments |
| A | Airway alternative — ETT or laryngeal mask airway (LMA) |
ETT sizes by weight:
| Birth Weight | ETT Size |
|---|
| <1 kg | 2.5 mm |
| 1–2 kg | 3.0 mm |
| >2 kg | 3.5 mm |
- ETT depth ("tip to lip") = 6 cm + weight in kg
- Confirm placement with capnography (CO₂ detector)
- Exclude right mainstem intubation by bilateral auscultation
STEP 6 — HR <60 bpm After Adequate PPV?
→ Chest Compressions + Escalation
- Intubate if not already done (ETT preferred for coordinated compressions)
- Chest compressions:
- Technique: 2-thumb encircling technique (preferred) or 2-finger technique
- Depth: ⅓ of AP chest diameter
- Rate: 3 compressions : 1 breath at 90 compressions + 30 breaths/min (120 events/min)
- Coordinate PPV with compressions — do not deliver simultaneously
- Switch to 100% O₂ during compressions
- Attach cardiac monitor (ECG) if not already done — ECG gives faster and more accurate HR than pulse oximetry in this phase
- Consider umbilical vein catheterization (UVC) for emergency vascular access
- Insert 3.5F or 5F umbilical catheter just below skin level with free backflow — do not advance into liver (risk of hypertonic solution injury)
STEP 7 — HR Still <60 bpm After Compressions + PPV?
→ Medications + Rule Out Reversible Causes
A. Epinephrine (FIRST LINE)
- Dose: 0.01–0.03 mg/kg IV (0.1–0.3 mL/kg of 1:10,000 solution)
- Route: IV (umbilical vein catheter preferred) → if no IV access yet: endotracheal route (1 mL saline flush) — note ETT absorption is unreliable, higher doses may be needed
- Repeat: Every 3–5 minutes if HR remains <60 bpm
B. Consider & Treat Reversible Causes
| Cause | Clue | Action |
|---|
| Hypovolemia | Pallor, poor tone, poor response to resuscitation, low BP | 10 mL/kg isotonic NS or lactated Ringer's IV (or O-negative blood if severe anemia) |
| Pneumothorax | Unequal breath sounds, unilateral chest rise | Needle decompression (2nd intercostal space, midclavicular) |
| Tension pneumothorax | Same as above, worsening despite resuscitation | Emergent needle/chest drain |
Nearly ⅔ of premature infants requiring resuscitation are hypovolemic at birth — always consider this.
Other medications in specific situations:
- Naloxone 0.1 mg/kg IV (or 0.2 mg/kg IM): only if respiratory depression from maternal opioids in last 4 hours — do NOT give if mother is a chronic opioid user (precipitates withdrawal)
- Sodium bicarbonate 2 mEq/kg (0.5 mEq/mL, 4.2% solution): only for documented severe metabolic acidosis with adequate ventilation, or prolonged resuscitation >5 min; infuse slowly ≤1 mEq/kg/min
STEP 8 — Baby Survives: Post-Resuscitation Care
Immediate stabilization:
- Continue monitoring: oxygenation, ventilation, perfusion, temperature, blood glucose
- Check blood glucose — up to 10% of neonates have hypoglycemia (glucose <35 mg/dL), especially those delivered by C-section
NICU Admission:
- Any neonate requiring: umbilical line, intubation, medications, or extensive resuscitation → transfer to NICU with personnel skilled in neonatal resuscitation
- If feasible and safe, allow parents to see, touch, and hold the baby before transport
Therapeutic Hypothermia (if HIE suspected):
- Indicated for moderate to severe hypoxic-ischemic encephalopathy (HIE)
- Target temp: 33.5–34.5°C for 72 hours, initiated within 6 hours of birth, then gradual rewarming over ≥4 hours
- Signs of evolving brain injury: abnormal consciousness, seizures, hypotonia, hyporeflexia
- Monitor for complications: thrombocytopenia, hypotension
Common post-resuscitation complications to watch for:
Hypoglycemia · Transient tachypnea of the newborn · Meconium aspiration syndrome · Pneumothorax · Electrolyte disturbances · Hyperbilirubinemia · Sepsis
Team Debriefing:
- Conduct a structured debrief with the full team after every resuscitation
- Review: what went well, what could improve, communication breakdowns, medication errors
- NRP emphasizes debriefing as a core component of the curriculum — simulation-based training with debriefing has been shown to improve provider confidence, technical skills, and patient outcomes
Quick Summary Flow
PRE-DELIVERY
Antenatal counseling → Team briefing → Equipment/room check
↓
BIRTH
Term? Tone? Breathing/crying?
↓ ALL YES → Routine care with mother
↓ ANY NO ↓
Warm · Position · Suction (if needed) · Dry · Stimulate (≤1 min)
↓
Apneic/gasping or HR <100?
↓ YES
PPV + SpO₂ monitor ± ECG
↓
HR still <100 or no chest rise?
↓ YES
MR.SOPA corrective steps → Intubate if needed
↓
HR <60?
↓ YES
Intubate + Chest compressions (3:1) + 100% O₂ + ECG + UVC
↓
HR still <60?
↓ YES
IV Epinephrine (repeat q3-5 min) + Rule out hypovolemia/pneumothorax
↓
HR ≥60 / improving
↓
Post-resuscitation care → NICU → Team debrief
Sources: Nelson Textbook of Pediatrics (9781260473797) — Fetal & Neonatal Resuscitation; Nelson's Emergency Medicine (9780323757898) — Ch. 159 Neonatal Resuscitation; Morgan & Mikhail's Clinical Anesthesiology (9781260473797)