Teach me hepatitis
Reading File
Finding Sources
Searching the Web
hepatitis types overview clinical features pathophysiology 2024
Reading File
Finding Sources
Searching Images
hepatitis virus types comparison clinical features
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile the full teaching response.
Hepatitis — A Complete Guide
Hepatitis means inflammation of the hepatic parenchyma. It can be caused by viruses (the most common cause), alcohol, drugs/toxins, autoimmune disease, or metabolic disorders.
1. Overview of Causes
| Category | Examples |
|---|---|
| Viral | HAV, HBV, HCV, HDV, HEV; also EBV, CMV, HSV |
| Alcoholic | Alcohol-induced steatohepatitis |
| Drug/Toxin | Isoniazid, acetaminophen, many others |
| Autoimmune | Autoimmune hepatitis (AIH) |
| Metabolic | NAFLD/NASH, Wilson disease, hemochromatosis |
2. General Clinical Features of Acute Hepatitis
All forms of acute hepatitis share a common presentation:
- Prodrome: low-grade fever, fatigue, anorexia, nausea/vomiting, RUQ pain, arthralgias/myalgias
- Icteric phase: dark urine, jaundice, clay-colored stools
- Labs: elevated bilirubin, ↑↑ transaminases (ALT > AST in viral; AST > ALT in alcoholic), elevated ALP
Alarm features (severe hepatic failure): mental status changes (hepatic encephalopathy), asterixis, ascites, prolonged PT/INR → require hospitalization and liver transplant evaluation.
Most cases of acute hepatitis resolve without complications and can be managed as outpatients, though symptomatic improvement precedes normalization of LFTs. — Textbook of Family Medicine 9e
3. Viral Hepatitis A–E
🅐 Hepatitis A (HAV)
| Feature | Details |
|---|---|
| Virus | Picornavirus (ssRNA, non-enveloped) |
| Transmission | Fecal-oral (contaminated food/water) |
| Incubation | 2–6 weeks |
| Chronicity | None — always self-limited, no carrier state |
| Immunity | Anti-HAV IgG confers lifelong immunity |
| Vaccine | Yes — formalin-inactivated, highly effective, licensed since 1995 |
Serology timeline:
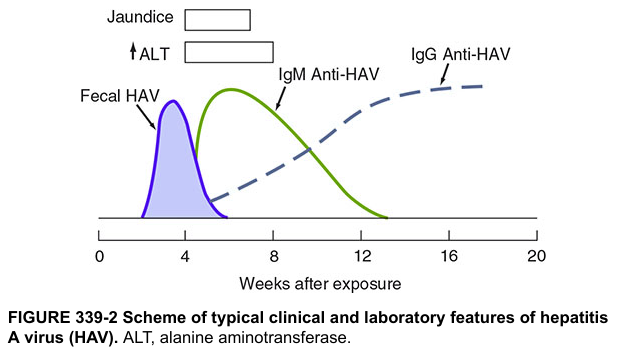
- Fecal HAV shedding peaks before symptoms
- IgM anti-HAV: acute infection marker (positive at symptom onset, resolves < 1 year)
- IgG anti-HAV: past infection / vaccine immunity (lifelong)
Post-exposure prophylaxis: Immune globulin (IG) within 1–2 weeks of exposure is ~90% effective. HAV vaccine is preferred for pre-exposure and provides more durable immunity.
🅑 Hepatitis B (HBV)
| Feature | Details |
|---|---|
| Virus | Hepadnavirus (dsDNA, enveloped) |
| Transmission | Parenteral, sexual, vertical (mother-to-child) |
| Incubation | 4–20 weeks |
| Chronicity | ~90% of neonates; ~5–10% of adults |
| Vaccine | Yes — recombinant HBsAg, 3-dose schedule |
Serology timeline:
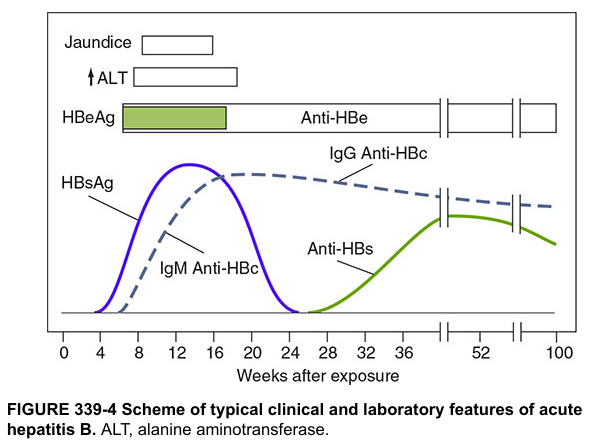
HBV Serology Interpretation Table (Jawetz Medical Microbiology)
| HBsAg | Anti-HBs | Anti-HBc | Interpretation |
|---|---|---|---|
| ✅ | ❌ | ❌ | Early acute HBV — confirm to exclude nonspecific reactivity |
| ✅ | ± | ✅ | Acute or chronic HBV — differentiate with IgM anti-HBc |
| ❌ | ✅ | ✅ | Past HBV infection — immune |
| ❌ | ❌ | ✅ | Past infection / low-level carrier / "window period" — check IgM anti-HBc + HBV DNA |
| ❌ | ❌ | ❌ | Never infected |
| ❌ | ✅ | ❌ | Successful vaccination |
Key antigens:
- HBsAg: first marker to appear; persists >6 months = chronic carrier
- HBeAg: marker of high replicative activity / high infectivity
- Anti-HBe: seroconversion = lower infectivity, sign of resolving infection
- IgM anti-HBc: best test for acute infection (short-lived, 3–6 weeks)
Vertical transmission risk:
- Mother HBsAg+ only: ~10–20% transmission
- Mother HBsAg+ and HBeAg+: ~90% transmission without prophylaxis
- Neonatal infection → 85–95% risk of chronic HBV
Treatment (chronic HBV): Indicated for chronic active hepatitis to prevent fibrosis progression and HCC.
- First-line: pegylated interferon alfa-2a, entecavir, tenofovir (preferred in pregnancy)
- Entecavir: guanosine analogue — 67% undetectable HBV DNA (HBeAg+), 90% (HBeAg–)
- Tenofovir: nucleotide analogue — 76% (HBeAg+), 93% (HBeAg–)
- Second-line: telbivudine; third-line: lamivudine, adefovir
🅒 Hepatitis C (HCV)
| Feature | Details |
|---|---|
| Virus | Flavivirus (ssRNA, enveloped), 6 genotypes |
| Transmission | Parenteral (IV drug use, needlestick); sexual (less efficient) |
| Incubation | ~6–12 weeks |
| Chronicity | ~70–85% become chronic |
| Vaccine | None available |
Natural history — chronic HCV:
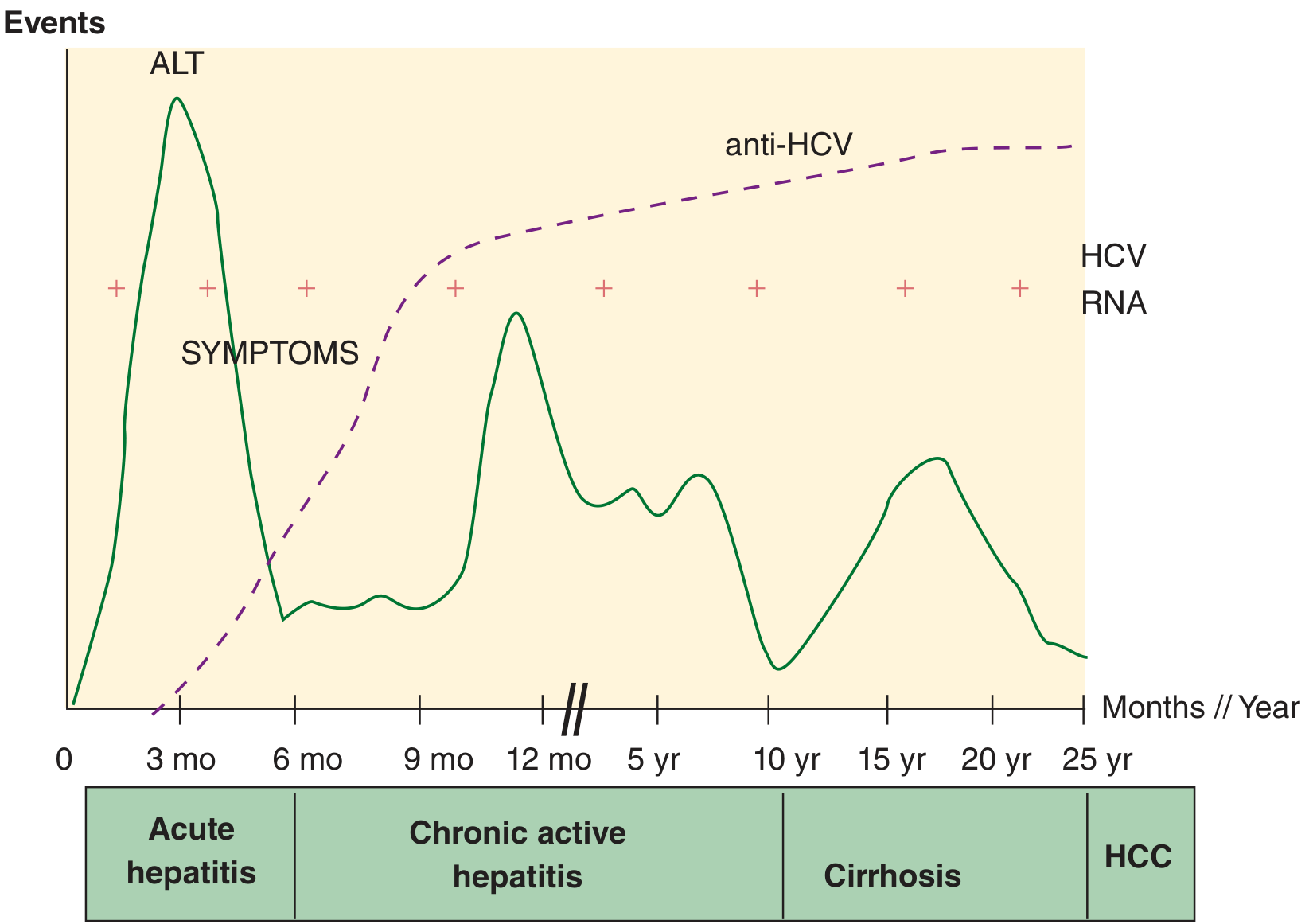
HCV RNA persists throughout (detectable from very early after infection). Anti-HCV rises ~3–12 months after exposure but does not confer immunity or indicate resolution. The characteristic "sawtooth" ALT pattern reflects episodic hepatic injury as disease progresses from acute → chronic active hepatitis → cirrhosis → HCC over decades.
Diagnosis:
- Anti-HCV: detects antibody (50–70% positive at symptom onset; lag of 3–6 weeks in others)
- HCV RNA by RT-PCR: confirms active infection; used for monitoring treatment
Treatment (modern era — direct-acting antivirals):
Direct-acting antiviral regimens using nucleoside inhibitors have revolutionized hepatitis treatment. — Rosen's Emergency Medicine
- Sofosbuvir (NS5B RNA polymerase inhibitor) + simeprevir (NS3/4A protease inhibitor): >90% sustained virological response (SVR)
- Interferon-free regimens now available with far less toxicity
- SVR = "functional cure" (undetectable HCV RNA 12 weeks after treatment end)
- Old standard (pegIFN + ribavirin): 30–35% SVR for genotype 1; 75–80% for genotypes 2/3
🅓 Hepatitis D (HDV) — "Delta Hepatitis"
| Feature | Details |
|---|---|
| Virus | Defective RNA virus — requires HBsAg to replicate |
| Transmission | Same as HBV (parenteral, sexual) |
| Forms | Coinfection (HAV + HBV simultaneous) vs. Superinfection (HDV in chronic HBV carrier) |
| Severity | Superinfection → more severe; ~70–80% progress to chronic disease |
| Prevention | HBV vaccination prevents HDV (HDV cannot exist without HBV) |
Coinfection (acute HBV + acute HDV): usually self-limited; low risk of chronic disease.
Superinfection (HDV in chronic HBV carrier): higher risk of fulminant hepatitis and cirrhosis.
🅔 Hepatitis E (HEV)
| Feature | Details |
|---|---|
| Virus | Hepevirus (ssRNA, non-enveloped), genotypes 1–4 |
| Transmission | Fecal-oral (genotypes 1 & 2 — developing world); zoonotic pork/game (genotypes 3 & 4 — developed world) |
| Incubation | ~2–8 weeks |
| Chronicity | Rare in immunocompetent; can be chronic in immunosuppressed (genotype 3) |
| Special danger | Pregnant women — mortality 5–25% (2nd/3rd trimester) — highest risk of acute liver failure |
| Vaccine | Available in China (not globally licensed) |
Clinical features resemble HAV. Most cases are self-limited. Neurologic manifestations (Guillain-Barré-like) are the most common extrahepatic feature with genotype 3.
4. Hepatitis Types at a Glance
| HAV | HBV | HCV | HDV | HEV | |
|---|---|---|---|---|---|
| Genome | ssRNA | dsDNA | ssRNA | ssRNA | ssRNA |
| Route | Fecal-oral | Parenteral/sexual/vertical | Parenteral | Parenteral/sexual | Fecal-oral |
| Incubation | 2–6 wk | 4–20 wk | 6–12 wk | 3–7 wk | 2–8 wk |
| Chronicity | None | ~5–10% (adults) | ~70–85% | ~70–80% (superinfection) | Rare (immunocompetent) |
| Fulminant | Rare | Rare | Very rare | Superinfection | Pregnant women |
| Vaccine | ✅ | ✅ | ❌ | (via HBV vaccine) | Limited |
5. Alcoholic Hepatitis
- Spectrum: steatosis → steatohepatitis → cirrhosis → HCC
- Labs: transaminases elevated but milder than viral hepatitis; AST:ALT ratio > 2:1 (classic)
- Hypoglycemia: common (depleted glycogen + suppressed gluconeogenesis)
- Severity scoring: Maddrey Discriminant Function (MDF) = 4.6 × (PT − control) + total bilirubin
- MDF > 32 = severe → prednisone 40 mg/day or methylprednisolone 32 mg IV/day
6. Other Non-Viral Causes
- Drug-induced: isoniazid, acetaminophen (acetaminophen overdose → treat immediately with N-acetylcysteine)
- Autoimmune hepatitis: positive ANA, anti-smooth muscle Ab (ASMA), elevated IgG; treat with prednisone ± azathioprine
- NAFLD/NASH: metabolic syndrome association; may progress to cirrhosis without viral etiology
7. Complications of Chronic Hepatitis
Any chronic hepatitis (B, C, alcoholic, autoimmune) can progress to:
- Cirrhosis → portal hypertension → ascites, varices, splenomegaly
- Hepatic encephalopathy (↑ ammonia)
- Hepatorenal syndrome (rising creatinine in liver failure)
- Hepatocellular carcinoma (HCC) — especially with HBV and HCV
8. Prevention Summary
| Agent | Vaccine | Post-Exposure Prophylaxis |
|---|---|---|
| HAV | ✅ Inactivated vaccine | Immune globulin (within 2 weeks) or HAV vaccine |
| HBV | ✅ Recombinant HBsAg (3 doses) | HBIG + HBV vaccine simultaneously |
| HCV | ❌ | None (no prophylaxis available) |
| HDV | (HBV vaccine protects) | — |
| HEV | Limited (China) | None globally available |
Sources
- Jawetz, Melnick & Adelberg's Medical Microbiology, 28th Ed.
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease
- Harrison's Principles of Internal Medicine, 21st Ed. (serology figures)
- Textbook of Family Medicine, 9th Ed.
- Rosen's Emergency Medicine
- Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.