Anti malarial drug
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of antimalarial drugs drawn from Katzung's Basic & Clinical Pharmacology, Goodman & Gilman's, and Lippincott Illustrated Reviews: Pharmacology.
Antimalarial Drugs
Life Cycle & Drug Target Sites
The diagram below shows exactly where each drug class acts in the parasite's life cycle:
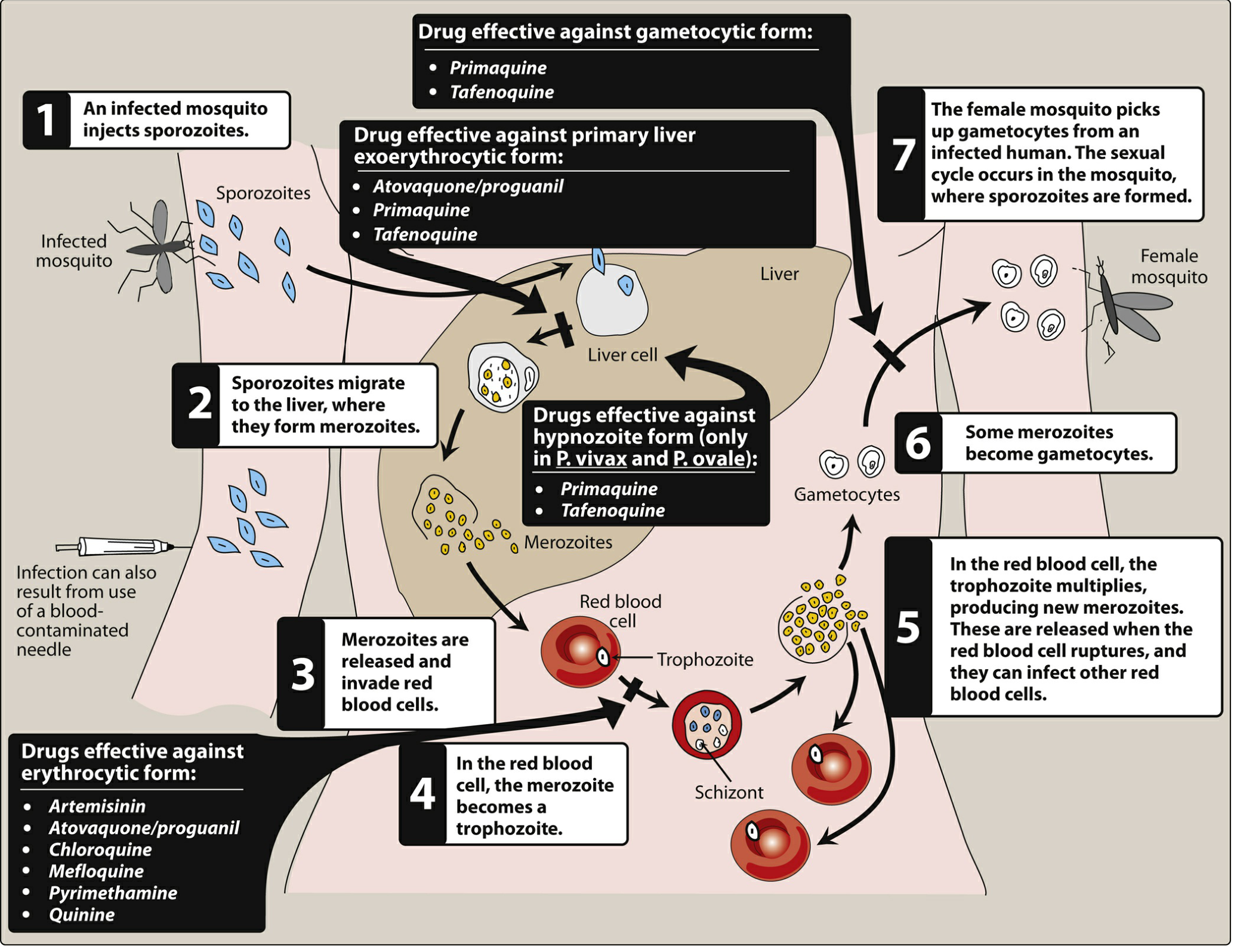
Life cycle of the malarial parasite showing sites of action of antimalarial drugs - Lippincott Illustrated Reviews: Pharmacology
Key Principle: No Single Drug Covers All Stages
As Goodman & Gilman explains:
- No antimalarial kills sporozoites - so true prevention of infection is impossible; drugs only prevent clinical disease.
- No single drug is effective against all hepatic and erythrocytic stages simultaneously - complete elimination may require combination therapy.
Classification & Major Drugs
Chemical structures of antimalarial drugs:
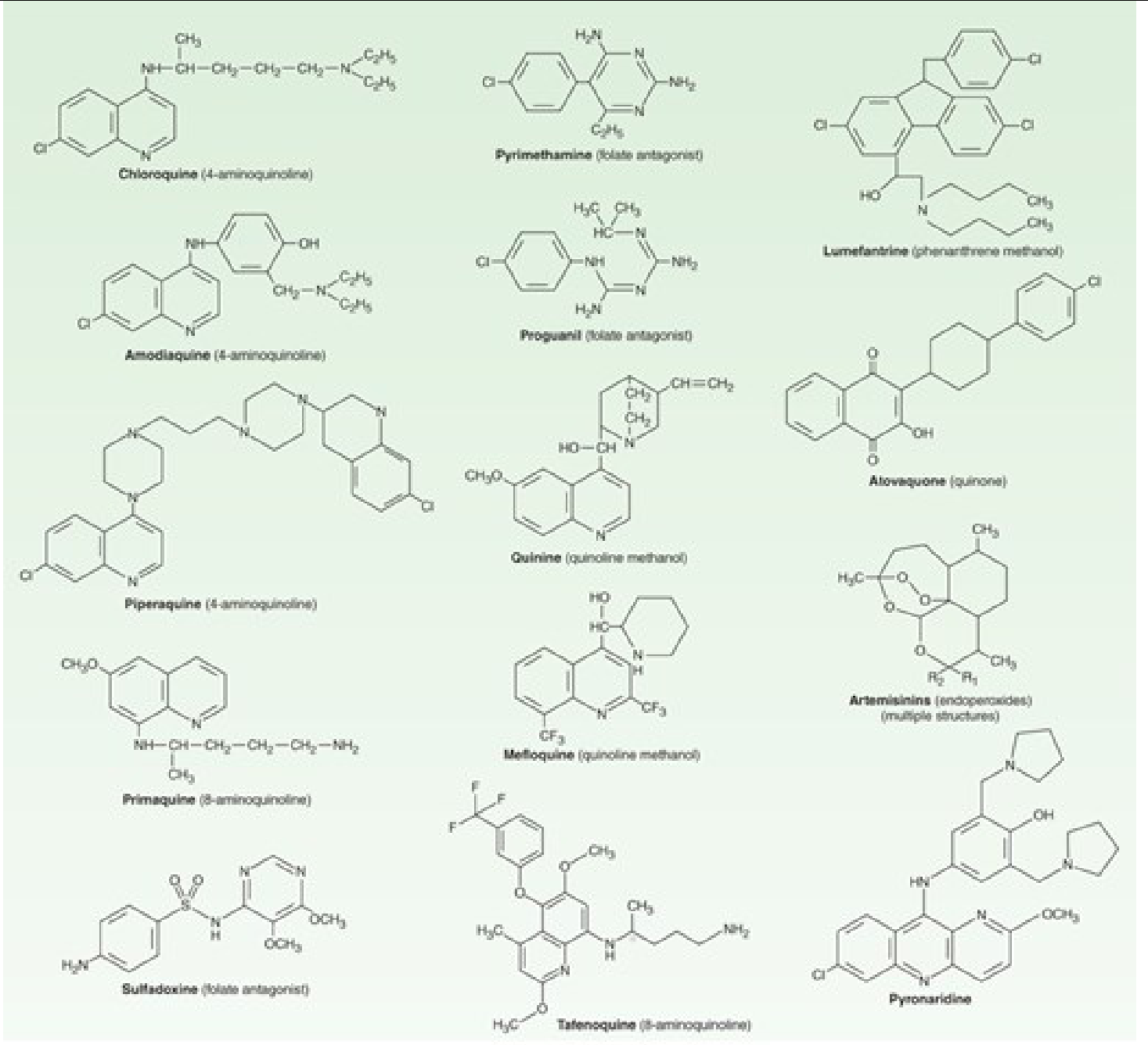
Katzung's Basic & Clinical Pharmacology
1. 4-Aminoquinolines
| Drug | Use |
|---|---|
| Chloroquine | Treatment & prophylaxis where parasites are still sensitive (now mainly Hispaniola, Central America west of Panama Canal) |
| Amodiaquine | Some chloroquine-resistant P. falciparum; used in fixed combination with artesunate |
| Piperaquine | P. falciparum in fixed combination with dihydroartemisinin |
Chloroquine mechanism: Accumulates in parasite food vacuole, inhibits heme polymerization - the parasite cannot detoxify heme (from hemoglobin digestion), so toxic heme accumulates and kills it.
Resistance: Widespread P. falciparum resistance via mutations in the chloroquine resistance transporter (CRT) that pumps the drug out of the food vacuole.
2. Quinoline Methanols
| Drug | Use |
|---|---|
| Quinine | Oral and IV treatment of P. falciparum (often combined with doxycycline or clindamycin) |
| Mefloquine | Prophylaxis and treatment of chloroquine-resistant P. falciparum |
Quinine - the original antimalarial from cinchona bark. Still used for severe malaria (IV) and multidrug-resistant cases. Adverse effects: cinchonism (tinnitus, headache, nausea), hypoglycemia, prolonged QT.
Mefloquine - weekly oral prophylactic. Neuropsychiatric side effects (vivid dreams, anxiety, psychosis) limit its use.
3. 8-Aminoquinolines
| Drug | Use |
|---|---|
| Primaquine | Radical cure and terminal prophylaxis of P. vivax and P. ovale (eradicates hypnozoites); kills gametocytes |
| Tafenoquine | Same indications as primaquine; longer half-life allows single-dose or weekly dosing |
Key facts about Primaquine:
- Acts on liver stages (exoerythrocytic) and gametocytes - NOT on erythrocytic stages (cannot be used as monotherapy)
- Mechanism: Oxidant metabolites disrupt plasmodial mitochondria
- Critical ADR: Hemolytic anemia in G6PD-deficient patients (must screen before use)
- Contraindicated in pregnancy, rheumatoid arthritis, SLE
Tafenoquine has a much longer half-life vs. primaquine - allowing single-dose treatment for relapse prevention; also requires G6PD screening.
4. Artemisinins (Sesquiterpene Lactone Endoperoxides)
| Drug | Notes |
|---|---|
| Artesunate (IV/oral) | First-line for severe malaria; oral in combination therapies |
| Artemether | Used in Coartem (artemether/lumefantrine) |
| Dihydroartemisinin | Active metabolite; combined with piperaquine |
- Fastest-acting antimalarials - 10-fold more potent than most other drugs
- Mechanism: Endoperoxide bridge reacts with heme iron to generate free radicals that damage parasite proteins and membranes
- Currently first-line agents for P. falciparum malaria worldwide (WHO recommends ACTs - Artemisinin-based Combination Therapies)
- Presently show no cross-resistance with other antimalarial drugs
5. Folate Antagonists
| Drug | Class | Use |
|---|---|---|
| Sulfadoxine-Pyrimethamine (Fansidar) | Sulfonamide + dihydrofolate reductase inhibitor | Some chloroquine-resistant P. falciparum; intermittent preventive therapy in pregnancy |
| Atovaquone-Proguanil (Malarone) | Quinone + biguanide | Treatment and prophylaxis of P. falciparum |
Atovaquone-Proguanil (Malarone):
- Atovaquone inhibits mitochondrial electron transport (cytochrome bc1 complex)
- Proguanil (converted to cycloguanil) inhibits dihydrofolate reductase
- Targets primary liver stages AND asexual blood stages - this means prophylaxis can be stopped sooner after travel (only 7 days vs. 4 weeks for mefloquine/chloroquine)
6. Tetracyclines
| Drug | Use |
|---|---|
| Doxycycline | Treatment with quinine for P. falciparum; chemoprophylaxis for multidrug-resistant areas (e.g., Thai border) |
- Daily oral dosing for prophylaxis
- Not safe in children <8 years or pregnant women
7. Lumefantrine & Pyronaridine (Combination Partners)
| Drug | Class | Use |
|---|---|---|
| Lumefantrine | Amyl alcohol | With artemether (Coartem) for uncomplicated P. falciparum |
| Pyronaridine | Mannich base acridine | With artesunate (Pyramax) for P. falciparum |
Chemoprophylaxis Summary (for Travelers)
| Drug | Area | Adult Dose |
|---|---|---|
| Chloroquine | Sensitive areas only (Hispaniola, C. America west of Panama Canal) | 500 mg weekly |
| Malarone | Chloroquine-resistant areas | 1 tablet daily |
| Mefloquine | Chloroquine-resistant areas | 250 mg weekly |
| Doxycycline | Multidrug-resistant areas (Thai border) | 100 mg daily |
| Primaquine | Terminal prophylaxis / alternative primary prevention | 52.6 mg daily |
| Tafenoquine | Terminal prophylaxis / alternative primary prevention | 200 mg once daily x3 days, then weekly |
Three Categories by Stage Coverage (Goodman & Gilman)
| Category | Drugs | What They Cover |
|---|---|---|
| 1 - Asexual blood stage only | Artemisinins, Chloroquine, Mefloquine, Quinine/Quinidine, Pyrimethamine, Sulfadoxine, Tetracyclines | Treat/prevent symptomatic malaria; do NOT reliably cover liver stages |
| 2 - Blood + primary liver stages | Atovaquone-Proguanil | Shorter post-exposure prophylaxis window |
| 3 - All liver stages + gametocytes | Primaquine, Tafenoquine | Radical cure (eradicates hypnozoites); needed for P. vivax / P. ovale relapse prevention; interrupts transmission |
Quick Memory Aid
- Chloroquine - classic drug, works where resistant strains haven't arrived
- Artemisinins - most potent, always used in combination (ACTs) to prevent resistance
- Primaquine/Tafenoquine - only drugs for hypnozoites (liver dormancy); need G6PD screen
- Malarone - convenient traveler's prophylaxis, short post-travel course
- Quinine + Doxycycline - backup for resistant or severe cases
Sources: Katzung's Basic & Clinical Pharmacology 16th Ed.; Goodman & Gilman's Pharmacological Basis of Therapeutics; Lippincott Illustrated Reviews: Pharmacology
This is a shared conversation. Sign in to Orris to start your own chat.