Stroke
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
"stroke"[MeSH Terms] AND "management"[MeSH Terms]
Searching the Web
stroke overview classification pathophysiology management 2024 2025 guidelines
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
I now have enough comprehensive information to write a thorough stroke overview. Here it is:
Stroke - Comprehensive Overview
A stroke is a cerebrovascular emergency defined as the sudden onset of a focal neurological deficit caused by either interruption of cerebral blood flow (ischemic stroke) or intracranial bleeding (hemorrhagic stroke). The core concept is "time is brain" - every minute of untreated stroke, approximately 1.9 million neurons are lost.
1. Classification
A. Ischemic Stroke (~85% of all strokes)
Caused by occlusion of a cerebral artery. Sub-classified by mechanism:
| Mechanism | Details |
|---|---|
| Large vessel atherosclerosis | Stenosis/thrombosis of major vessels (ICA, MCA, basilar) |
| Cardioembolism | Clot from the heart; most common cause is atrial fibrillation (5x increased risk) |
| Small vessel disease (lacunar) | Occlusion of small penetrating arteries; infarcts ≤1.5 cm in subcortical areas or brainstem |
| Cryptogenic | No identifiable cause despite full workup |
| Other determined cause | Hypercoagulability, dissection, vasculitis, etc. |
B. Hemorrhagic Stroke (~15%)
- Intracerebral hemorrhage (ICH): Bleeding directly into brain parenchyma. Causes 8-11% of all acute strokes; 7-day mortality ~30%, 1-year mortality even higher.
- Subarachnoid hemorrhage (SAH): Blood into the subarachnoid space, classically presenting as sudden severe ("thunderclap") headache. Often from ruptured aneurysm.
C. Transient Ischemic Attack (TIA)
A temporary, non-marching neurological deficit lasting <24 hours (most only a few minutes), attributed to focal ischemia, with full clinical recovery. About 1 in 10 patients with TIA have a stroke within 3 months - 50% within 48 hours. A "tissue-based" definition now recognizes TIA based on DWI-MRI lesions regardless of duration. - Bradley and Daroff's Neurology in Clinical Practice
2. Risk Factors
Non-modifiable: Age, sex, family history, race/ethnicity
Modifiable (the most important targets):
- Hypertension (the strongest single modifiable risk factor)
- Atrial fibrillation
- Smoking
- Diabetes mellitus
- Dyslipidemia
- Obesity, physical inactivity
- Excessive alcohol use
- Prior TIA or stroke
The 2024 AHA/ASA Primary Prevention of Stroke Guideline emphasizes "Life's Essential 8," updated BP targets, GLP-1 receptor agonists, lipid-lowering, antithrombotic therapy, colchicine, and social determinants of health.
3. Pathophysiology
Ischemic
The pathological features depend on the stroke mechanism, vessel size, and collateral blood flow availability:
- In hypotension-related ischemia: watershed (border zone) infarction is most common
- With main artery occlusion + good collaterals: wedge-shaped territory infarct
- With main artery occlusion + no collaterals: entire arterial territory infarcted
- Lacunar infarcts (≤1.5 cm) in subcortical areas may barely be visible macroscopically
- Hemorrhagic transformation can occur with reperfusion
Microscopically, the timeline of changes:
- 0-4 hours: Neuronal swelling, no overt changes
- 4-6 hours: Neutrophil infiltration begins
- 36 hours: Abundant neutrophils; astrocyte and endothelial swelling
- 48 hours: Microglial proliferation; foamy macrophages from myelin ingestion
- Later: Neovascularization, cavity formation with glial/fibrovascular elements
Three distinct zones in large infarction: (1) core coagulative necrosis, (2) middle zone of vacuolated neuropil and leucocytic infiltrates, (3) outer marginal zone of hyperplastic astrocytes. - Bradley and Daroff's Neurology in Clinical Practice
Hemorrhagic
ICH is clinically indistinguishable from ischemic stroke without imaging. Headache, nausea, and vomiting often precede the neurologic deficit. Unlike SAH, headache onset in ICH is more insidious. - Tintinalli's Emergency Medicine
4. Clinical Features
Depend on the vascular territory involved:
| Territory | Features |
|---|---|
| MCA (most common) | Contralateral hemiplegia/hemisensory loss (face + arm > leg), aphasia (dominant), neglect (non-dominant), gaze deviation toward lesion |
| ACA | Contralateral leg > arm weakness, abulia, incontinence |
| PCA | Contralateral homonymous hemianopia, alexia without agraphia, memory impairment |
| Vertebrobasilar | Diplopia, vertigo, dysarthria, dysphagia, ataxia, crossed sensorimotor deficits, "locked-in" syndrome with basilar occlusion |
| Lacunar | Pure motor, pure sensory, sensorimotor, ataxic hemiparesis, dysarthria-clumsy hand |
TIA warning features:
- Carotid territory: ipsilateral amaurosis fugax, contralateral motor/sensory deficit, aphasia, homonymous hemianopia
- Vertebrobasilar: bilateral/shifting motor or sensory deficits, visual loss in homonymous fields, perioral numbness; isolated diplopia or vertigo alone is NOT sufficient for TIA diagnosis
ABCD2 Score (TIA risk stratification): based on Age, Blood pressure ≥140/90, Clinical features, TIA Duration, and Diabetes. Score ≥4 = moderate-to-high stroke risk → hospital admission warranted. - Bradley and Daroff's Neurology in Clinical Practice
5. Investigations
Immediate (in all suspected strokes):
- Non-contrast CT head - first-line; rules out hemorrhage immediately; CT sensitivity for SAH is ~98% within 6-12 hours of onset
- CT angiography (CTA) - identifies large vessel occlusion (LVO) for thrombectomy decisions
- MRI DWI/ADC - most sensitive for acute ischemia; DWI shows restricted diffusion within minutes; also identifies TIA lesions that would be missed clinically
- Transcranial Doppler (TCD) - detects MCA/ICA occlusion; >85% sensitivity/specificity for M1 and supraclinoid ICA; also monitors recanalization after tPA
Below are DWI-MRI examples: Left image (A) shows small acute infarct; right image (B) shows a large territory infarct.
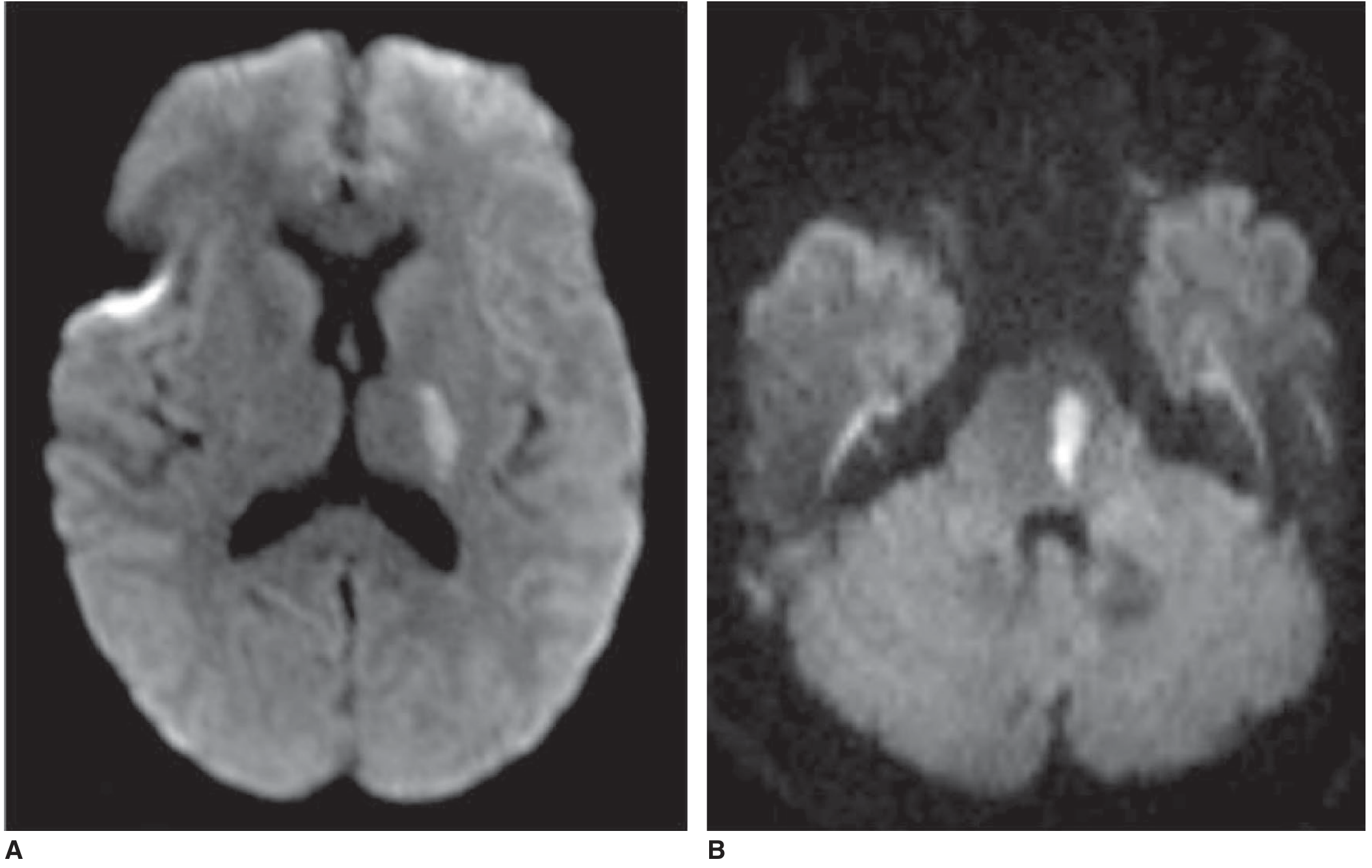
Images from Adams and Victor's Principles of Neurology, 12th Edition
Other investigations:
- ECG (detect atrial fibrillation)
- Echocardiography (cardiac source of embolism)
- Lipid profile, HbA1c, CBC, coagulation studies
- Holter monitoring for paroxysmal AF
- Carotid ultrasound
6. Acute Management
Treatment of acute ischemic stroke has four approaches: (1) general supportive measures, (2) reperfusion/recanalization, (3) cytoprotective strategies, (4) anti-inflammatory strategies. - Bradley and Daroff's Neurology
Reperfusion
IV Thrombolysis (IV tPA / alteplase):
- Window: within 4.5 hours of symptom onset (some systems extend this with imaging guidance)
- "Wake-up strokes" without known onset time can be treated based on DWI-FLAIR mismatch
- tPA is less effective for large vessel occlusions (only ~20% recanalization) - Schwartz's Surgery
Mechanical Thrombectomy (endovascular):
- Indicated for large vessel occlusion (LVO) of the distal ICA or proximal MCA
- Window: within 6 hours of onset; can extend to 18-24 hours with appropriate imaging (perfusion-diffusion mismatch on CT/MRI)
- Landmark trials: MR CLEAN, ESCAPE, EXTEND-IA, SWIFT-PRIME, REVASCAT all confirmed benefit
- Can be done with or without preceding IV tPA
- Significantly superior to tPA alone for LVO
Heparin/LMWH: No proven benefit for reducing stroke morbidity, mortality, or early recurrence (International Stroke Trial, 20,000 patients). May be useful in specific situations (cerebral venous thrombosis, small cardioembolic infarcts with intracardiac thrombus on echo). - Bradley and Daroff's Neurology
General Supportive Measures
- Airway protection, oxygen if SpO2 <94%
- Blood pressure management (permissive hypertension up to 220/120 before tPA; strict control after thrombolysis)
- Glycemic control
- Fever management
- DVT prophylaxis
7. Hemorrhagic Stroke Management
ICH management is fundamentally different from ischemic stroke:
- Reverse anticoagulation urgently
- Blood pressure control (target SBP <140 mmHg)
- Neurosurgical consultation for cerebellar hemorrhage >3 cm or hydrocephalus
- ICP management
SAH management:
- Secure the aneurysm (surgical clipping or endovascular coiling)
- Nimodipine to prevent vasospasm
- Avoid hypotension; treat hydrocephalus with EVD if needed
8. Secondary Prevention
| Stroke Mechanism | Prevention Strategy |
|---|---|
| Small vessel disease | Antiplatelet (aspirin ± dipyridamole, or clopidogrel); aggressive BP control |
| Large vessel atherosclerosis | Antiplatelet; high-intensity statin; carotid endarterectomy/stenting if ≥70% stenosis |
| Cardioembolism (AF) | Oral anticoagulation - DOACs preferred over warfarin (except in rheumatic AF) |
| Hypercoagulable states | Anticoagulation as indicated |
| Cryptogenic stroke | Antiplatelet; extended cardiac monitoring to find occult AF |
Primary prevention targets: hypertension control, smoking cessation, glycemic control, lipid-lowering (statins), treating AF. The 2024 AHA guideline also highlights GLP-1 receptor agonists (for diabetes/obesity) and colchicine as newer additions. - Adams and Victor's Principles of Neurology, 12th Ed
9. Complications & Rehabilitation
Early complications:
- Cerebral edema (peaks 2-5 days; malignant MCA syndrome may require hemicraniectomy)
- Hemorrhagic transformation of ischemic infarct
- Aspiration pneumonia (most common cause of early death)
- DVT/pulmonary embolism
- Post-stroke seizures
- Hydrocephalus (especially with cerebellar or SAH)
Long-term complications:
- Post-stroke depression (~30%)
- Vascular dementia
- Spasticity, contractures
- Dysphagia
- Recurrent stroke
Rehabilitation begins as early as possible (within 24-48 hours if stable): physiotherapy, occupational therapy, speech-language therapy. The degree of recovery depends heavily on stroke location, size, patient age, and time to treatment.
Key "Time is Brain" Summary
| Time Window | Action |
|---|---|
| 0-4.5 hours | IV tPA eligible (if no contraindications) |
| 0-6 hours | Mechanical thrombectomy for LVO |
| 6-24 hours | Thrombectomy still possible with imaging mismatch (DEFUSE 3, DAWN trial criteria) |
| >24 hours | No reperfusion; supportive care + secondary prevention |
Sources:
- Bradley and Daroff's Neurology in Clinical Practice
- Adams and Victor's Principles of Neurology, 12th Edition
- Tintinalli's Emergency Medicine: A Comprehensive Study
- Fuster and Hurst's The Heart, 15th Edition
- 2024 AHA/ASA Primary Prevention of Stroke Guideline
This is a shared conversation. Sign in to Orris to start your own chat.