ABG analysis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Now I have comprehensive information from authoritative textbooks. Let me compile a thorough ABG analysis guide.
Arterial Blood Gas (ABG) Analysis
Normal Values
| Parameter | Normal Range |
|---|---|
| pH | 7.35 - 7.45 |
| PaCO2 | 35 - 45 mm Hg |
| PaO2 | 70 - 95 mm Hg (age-dependent) |
| HCO3- | 22 - 26 mEq/L |
| SaO2 | 95 - 100% |
| Base Excess | -2 to +2 mEq/L |
PaO2 (sitting) = 104.2 - (0.27 × age in years) - Goldman-Cecil Medicine
Step-by-Step ABG Interpretation
Step 1 - Assess pH
- < 7.35 = Acidemia
- 7.35 - 7.45 = Normal (but a mixed disorder may still be present)
- > 7.45 = Alkalemia
Step 2 - Determine the Primary Disorder
Look at PaCO2 and HCO3- to identify what's driving the pH change:
| Disorder | pH | PaCO2 | HCO3- |
|---|---|---|---|
| Respiratory Acidosis | ↓ | ↑ (primary) | ↑ (compensation) |
| Respiratory Alkalosis | ↑ | ↓ (primary) | ↓ (compensation) |
| Metabolic Acidosis | ↓ | ↓ (compensation) | ↓ (primary) |
| Metabolic Alkalosis | ↑ | ↑ (compensation) | ↑ (primary) |
Key rule: If PaCO2 and pH move in opposite directions, it's respiratory. If they move in the same direction, it's metabolic.
Step 3 - Check for Compensation (Are "Renal Rules" Met?)
If the measured compensatory value matches the predicted value, it's a simple disorder. If it doesn't match, a mixed disorder is present.
Compensation Formulas (Costanzo Physiology, 7th ed., Table 7.3):
| Disorder | Predicted Compensation |
|---|---|
| Metabolic Acidosis | ↓ PaCO2 = 1.3 × (24 - HCO3-) [Winter's Formula: PaCO2 = 1.5(HCO3-) + 8 ± 2] |
| Metabolic Alkalosis | ↑ PaCO2 = 0.7 × (HCO3- - 24) |
| Acute Respiratory Acidosis | ↑ HCO3- = 0.1 × (PaCO2 - 40) |
| Chronic Respiratory Acidosis | ↑ HCO3- = 0.4 × (PaCO2 - 40) |
| Acute Respiratory Alkalosis | ↓ HCO3- = 0.2 × (40 - PaCO2) |
| Chronic Respiratory Alkalosis | ↓ HCO3- = 0.4 × (40 - PaCO2) |
"The compensatory response is always in the same direction as the original disturbance." - Costanzo Physiology, 7th ed.
Step 4 - Calculate Anion Gap (if metabolic acidosis present)
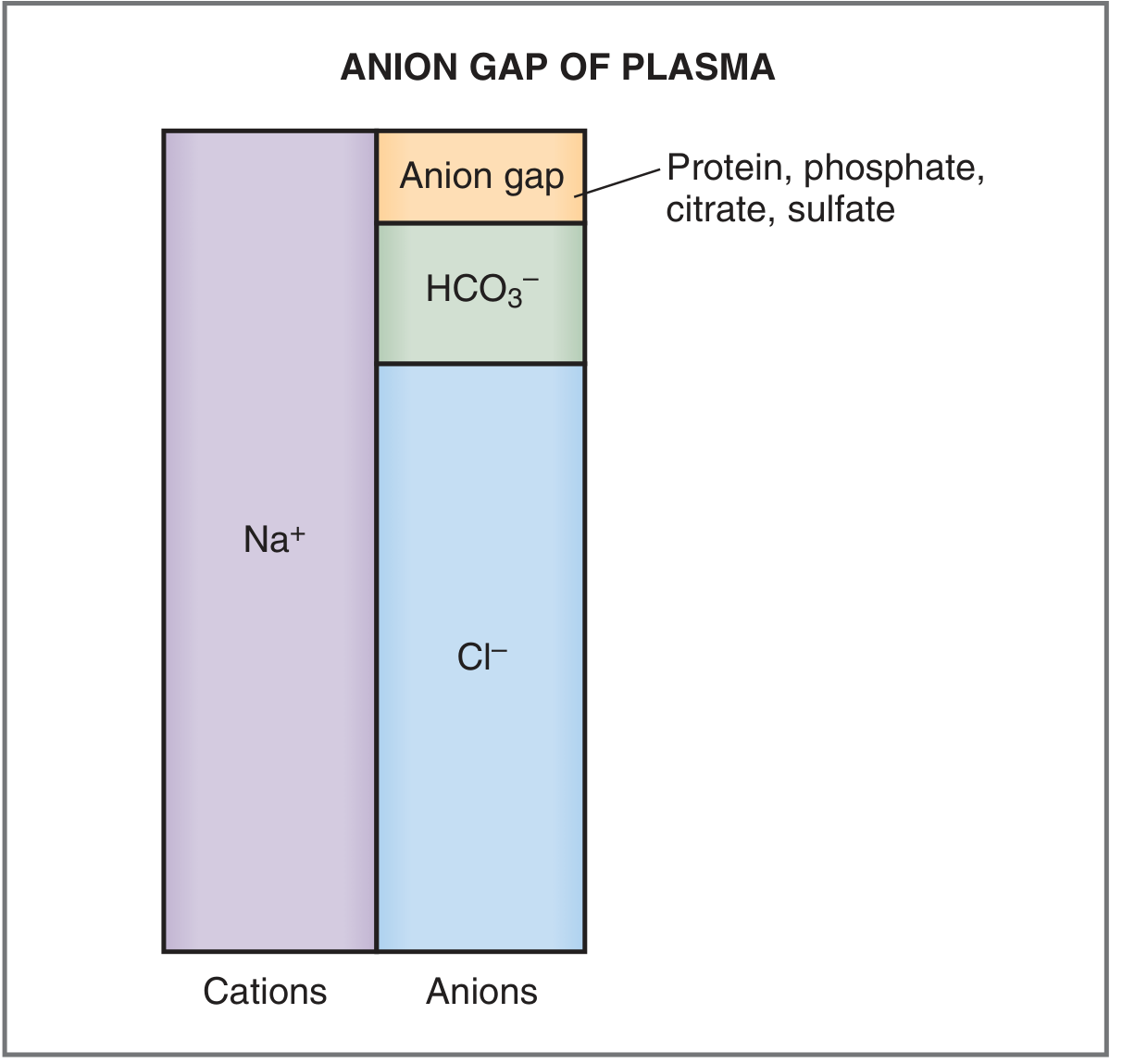
Anion Gap (AG) = [Na+] - ([HCO3-] + [Cl-])
- Normal AG = 8-16 mEq/L (often cited as ~12 ± 4)
- The gap represents unmeasured anions: plasma proteins, phosphate, citrate, sulfate
High Anion Gap Metabolic Acidosis (HAGMA)
Mnemonic: MUDPILES
- Methanol
- Uremia (chronic renal failure)
- Diabetic ketoacidosis
- Propylene glycol / Paraldehyde
- Isoniazid / Iron
- Lactic acidosis
- Ethylene glycol
- Salicylates
Normal Anion Gap Metabolic Acidosis (NAGMA) - Hyperchloremic
Mnemonic: HARDUP
- Diarrhea, RTA (renal tubular acidosis), Addison's disease, pancreatic fistula, ureteral diversions
Step 5 - Assess Oxygenation
A-a Gradient
P(A-a)O2 = FiO2(PB - PH2O) - (PaO2 + PaCO2/0.8)
Simplified at room air (sea level):
P(A-a)O2 = 150 - PaO2 - (PaCO2/0.8)
Normal P(A-a)O2 = Age/4 + 4
| Mechanism of Hypoxemia | A-a Gradient |
|---|---|
| V/Q mismatch (pneumonia, PE) | Increased |
| Diffusion impairment (ILD) | Increased |
| R-to-L shunt | Increased |
| Hypoventilation | Normal |
| High altitude / low FiO2 | Normal |
- Goldman-Cecil Medicine, Table 89-1
Acid-Base Map
This map plots PCO2 (y-axis) vs. [HCO3-] (x-axis) with pH isopleths. Each shaded band represents a simple disorder:
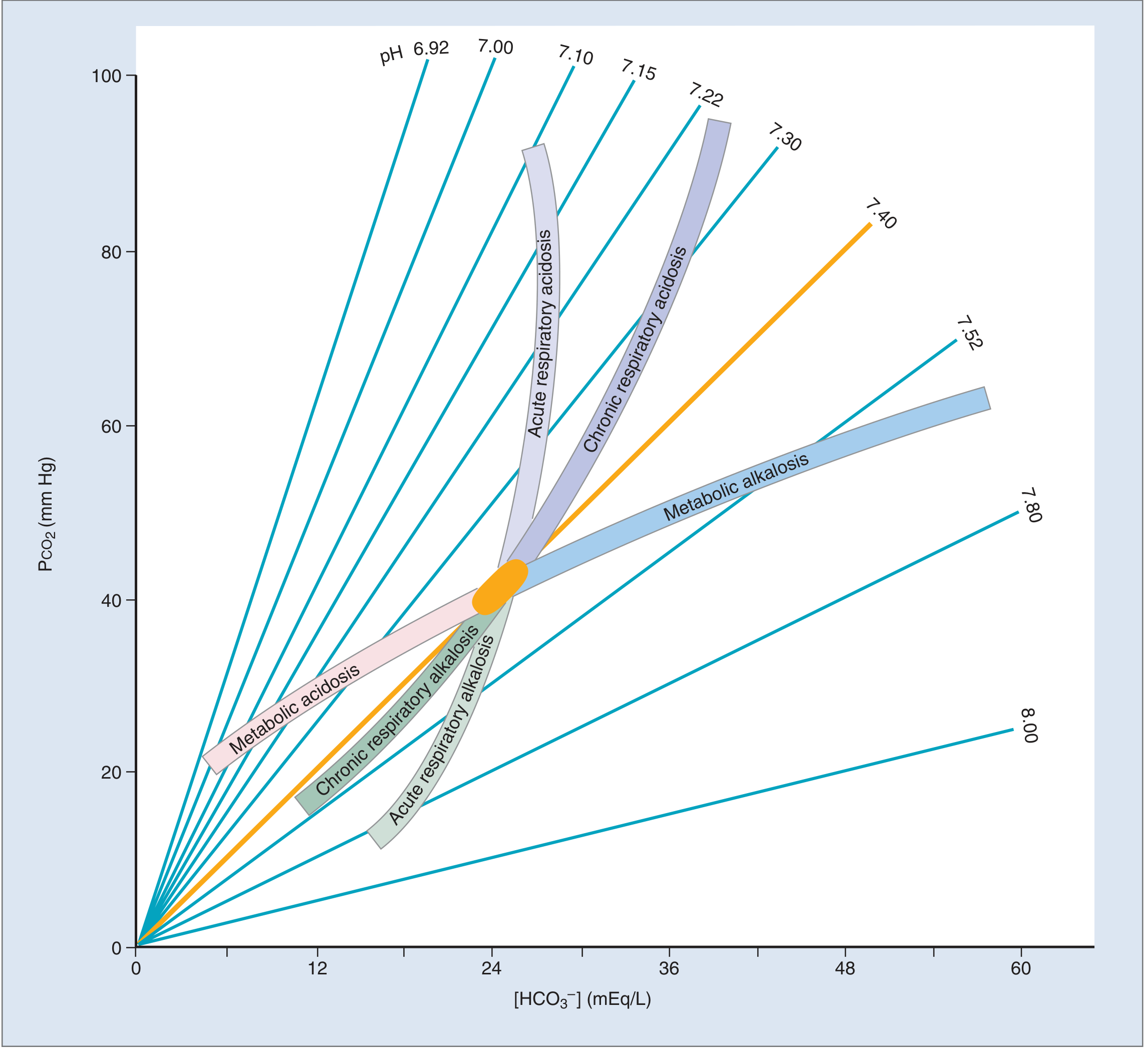
- If the patient's values fall within a shaded band: single simple disorder
- If values fall between bands: mixed acid-base disorder
- Costanzo Physiology, 7th ed., Fig. 7.10
Summary Table of the 4 Simple Disorders
| Disorder | pH | PaCO2 | HCO3- | Resp. Compensation | Renal Compensation |
|---|---|---|---|---|---|
| Metabolic Acidosis | ↓ | ↓ | ↓ (1°) | Hyperventilation | ↑ HCO3- reabsorption |
| Metabolic Alkalosis | ↑ | ↑ | ↑ (1°) | Hypoventilation | ↑ HCO3- excretion |
| Respiratory Acidosis | ↓ | ↑ (1°) | ↑ | None | ↑ HCO3- reabsorption |
| Respiratory Alkalosis | ↑ | ↓ (1°) | ↓ | None | ↓ HCO3- reabsorption |
Quick Clinical Approach at the Bedside
- pH acidemia or alkalemia?
- Which parameter is most abnormal and consistent with the pH change? (That's the primary disorder)
- Is compensation appropriate? (Use the formulas above)
- If metabolic acidosis: calculate AG
- If high AG: calculate delta-delta ratio = (AG - 12) / (24 - HCO3-): ratio 1-2 = pure HAGMA; <1 = NAGMA coexisting; >2 = concurrent metabolic alkalosis
- Assess oxygenation: PaO2, SaO2, A-a gradient
Sources:
- Goldman-Cecil Medicine, Systemic ABG Analysis section
- Costanzo Physiology, 7th Edition, Acid-Base Disorders, pp. 330-335
- Tintinalli's Emergency Medicine, ABG Analysis chapter
This is a shared conversation. Sign in to Orris to start your own chat.