Jaundice - cause, types, and symptoms
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a thorough, well-cited answer. Here it is:
Jaundice: Causes, Types, and Symptoms
What Is Jaundice?
Jaundice (also called icterus) is the yellowish discoloration of the skin, sclera (whites of the eyes), and mucous membranes caused by excess bilirubin in the extracellular fluids. It becomes clinically visible when the serum bilirubin rises above approximately 2.5-3 mg/dL (normal is ~0.5 mg/dL). - Schwartz's Principles of Surgery, 11th Ed., p. 1381
Hyperbilirubinemia technically begins above 1 mg/dL, but visible jaundice requires tissue saturation at roughly 2-2.5 mg/dL. - Harper's Illustrated Biochemistry, 32nd Ed.
Bilirubin Metabolism (Background)
Understanding jaundice requires understanding how bilirubin is produced and cleared:
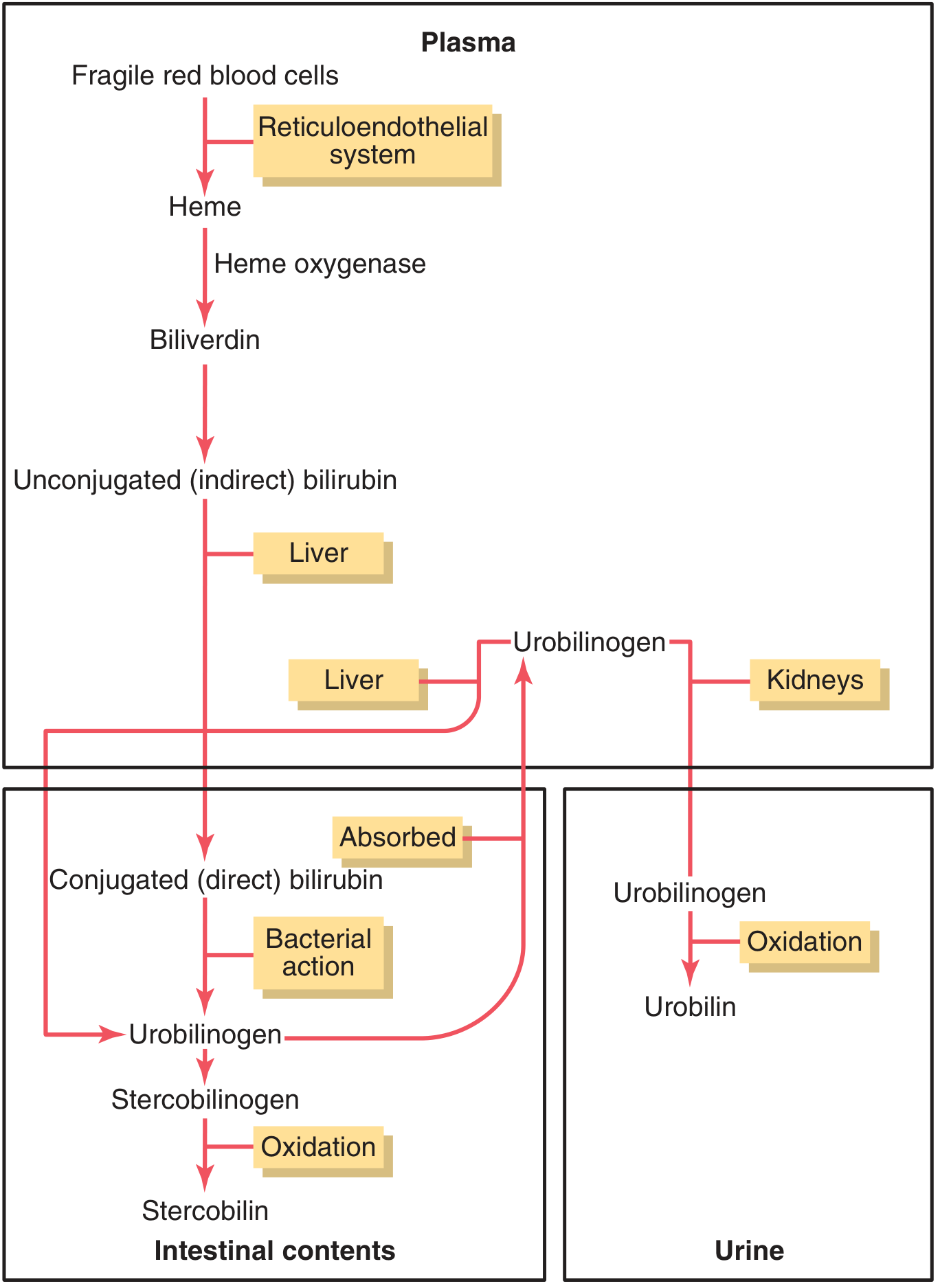
Figure: Bilirubin formation and excretion (Guyton & Hall Textbook of Medical Physiology)
- Aged red blood cells (lifespan ~120 days) are broken down by the reticuloendothelial system (macrophages). Hemoglobin splits into globin + heme. Heme opens to form biliverdin, then unconjugated (indirect) bilirubin.
- Unconjugated bilirubin is fat-soluble and insoluble in water - it binds albumin in plasma and travels to the liver.
- In the liver, it is conjugated (mostly with glucuronic acid) to form conjugated (direct) bilirubin, which is water-soluble.
- Conjugated bilirubin is excreted into bile and passes into the intestines, where bacteria convert it to urobilinogen - some is reabsorbed, some is excreted in urine, and the remainder becomes stercobilin (which gives stool its brown color). - Guyton & Hall Textbook of Medical Physiology
Types of Jaundice (by Location)
Jaundice is classified by where the metabolic defect occurs: prehepatic, hepatic (intrahepatic), and posthepatic. - Schwartz's Principles of Surgery, 11th Ed.
1. Prehepatic (Hemolytic) Jaundice
Cause: Excessive destruction of red blood cells - more bilirubin is produced than the liver can conjugate and excrete. The liver function itself is intact.
- Predominantly unconjugated (indirect) hyperbilirubinemia
- Urobilinogen in urine and stool is increased
- No bilirubin in urine (unconjugated bilirubin is albumin-bound and cannot be filtered by kidneys)
Specific causes:
- Inherited hemolytic anemias: sickle cell disease, hereditary spherocytosis, G6PD deficiency, thalassemia
- Acquired immune-mediated: autoimmune hemolytic anemia (positive direct Coombs test), drug-induced
- Acquired non-immune: mechanical trauma (prosthetic heart valves), microangiopathic hemolytic anemia, infections (malaria), toxins
- Gilbert's syndrome: Mild, benign reduction in UDP-glucuronosyltransferase activity; affects ~4-7% of the population; unconjugated bilirubin rises during fasting or stress - self-limited
- Crigler-Najjar syndrome: Rare, severe neonatal deficiency of conjugating enzyme; can cause bilirubin encephalopathy (kernicterus)
- Neonatal physiologic jaundice: Accelerated hemolysis plus immature hepatic conjugation machinery in newborns - Schwartz's, Harper's
2. Hepatic (Intrahepatic) Jaundice
Cause: The liver itself is damaged, impairing both conjugation and/or excretion of bilirubin. Can produce mixed (unconjugated + conjugated) hyperbilirubinemia.
Specific causes:
- Viral hepatitis (Hepatitis A, B, C, D, E) - the most common cause of hepatocellular jaundice
- Alcoholic liver disease
- Drug/toxin-induced hepatitis: acetaminophen overdose, oral contraceptives, anabolic steroids, rifampicin
- Autoimmune hepatitis
- Cirrhosis: end-stage chronic liver disease; jaundice marks transition to decompensated cirrhosis - Goldman-Cecil Medicine
- Sepsis: systemic infection impairs hepatocyte bilirubin transport
- Ischemic/hypoxic hepatitis: any condition impairing hepatic blood flow
- Primary biliary cholangitis (PBC) / Primary sclerosing cholangitis (PSC): cholestatic diseases causing progressive biliary destruction
- Inherited excretion disorders:
- Dubin-Johnson syndrome: defective secretion of conjugated bilirubin from hepatocytes into bile - conjugated hyperbilirubinemia (benign)
- Rotor syndrome: similar defect, also benign - Schwartz's, Harper's
3. Posthepatic (Obstructive / Cholestatic) Jaundice
Cause: Obstruction of the biliary duct system preventing bile (containing conjugated bilirubin) from reaching the duodenum. Predominantly conjugated (direct) hyperbilirubinemia.
- Bilirubin cannot reach intestines - stool becomes clay/pale colored (no stercobilin)
- No urobilinogen reabsorption - urobilinogen absent from urine
- Conjugated bilirubin accumulates in blood, spills into urine - dark ("tea-colored") urine
- Urine foam turns yellow on shaking
Specific causes:
- Choledocholithiasis (gallstone in common bile duct) - most common cause
- Pancreatic cancer (cancer of the head of pancreas) - classic cause of painless obstructive jaundice
- Cholangiocarcinoma (bile duct cancer)
- Benign biliary strictures
- Pancreatitis / pancreatic pseudocyst (extrinsic compression)
- Primary sclerosing cholangitis
- Cholangitis (infection of bile ducts)
- Post-surgical complications: clips, retained stones, ischemic bile duct injury - Schwartz's Principles of Surgery
Summary Table
| Feature | Prehepatic | Hepatic | Posthepatic |
|---|---|---|---|
| Bilirubin type | Unconjugated (indirect) | Mixed | Conjugated (direct) |
| Urine color | Normal | Dark (if conjugated) | Dark ("tea-colored") |
| Stool color | Dark (more stercobilin) | Variable | Pale/clay-colored |
| Urine urobilinogen | Increased | Variable | Absent |
| Urine bilirubin | Absent | Present (if conjugated) | Present |
| Example causes | Hemolysis, Gilbert's | Hepatitis, cirrhosis | Gallstones, pancreatic cancer |
Clinical Symptoms
Jaundice itself is a sign, but it comes with a constellation of symptoms depending on the underlying cause:
Universal symptoms:
- Yellow skin and sclera - the hallmark. Scleral icterus appears first (fat-rich sclera takes up bilirubin early)
- Pruritus (itching) - especially prominent in cholestatic/obstructive jaundice; caused by bile salt deposition in skin. Can be severe and debilitating - Sleisenger & Fordtran's GI and Liver Disease
- Dark urine - in conjugated hyperbilirubinemia (conjugated bilirubin is water-soluble and filtered by kidneys)
- Pale/clay-colored stools - in obstructive jaundice (absent stercobilin)
- Fatigue and malaise
In hemolytic jaundice:
- Anemia symptoms: pallor, fatigue, dyspnea
- Splenomegaly (from increased RBC destruction)
- Dark urine not typical (bilirubin not conjugated - cannot appear in urine)
In hepatic jaundice:
- Nausea, vomiting, anorexia
- Right upper quadrant (RUQ) pain or discomfort
- Hepatomegaly, tender liver
- Features of liver failure in severe cases: encephalopathy, spider angiomata, ascites, coagulopathy
In obstructive jaundice:
- Progressively deepening jaundice
- Clay-colored stools
- Dark urine (conjugated bilirubin in urine)
- Severe pruritus
- Charcot's triad (in cholangitis): fever/chills + RUQ pain + jaundice
- Weight loss if due to malignancy (painless progressive jaundice = pancreatic cancer until proven otherwise)
Special Note: Neonatal Jaundice
Physiologic jaundice of the newborn results from immature hepatic conjugation + accelerated hemolysis at birth. It is usually unconjugated and benign. However, severe unconjugated hyperbilirubinemia can cross the blood-brain barrier (conjugated bilirubin cannot), causing kernicterus - bilirubin encephalopathy with permanent brain damage. - Guyton & Hall; Harper's Illustrated Biochemistry
Treatment: phototherapy (converts unconjugated bilirubin to a water-soluble form for excretion).
Sources:
- Guyton and Hall Textbook of Medical Physiology
- Harper's Illustrated Biochemistry, 32nd Ed.
- Schwartz's Principles of Surgery, 11th Ed.
- Goldman-Cecil Medicine (International Edition)
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.