Cranial nerves from zero to master
Reading File
Finding Sources
Finding Sources
Searching the Web
cranial nerves complete guide anatomy function clinical testing
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Searching Images
cranial nerves overview diagram all 12 brain
Loading Image
Loading Image
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
I now have comprehensive material from multiple authoritative sources. Let me compile the complete master-level guide:
The Cranial Nerves: Zero to Master
The Big Picture
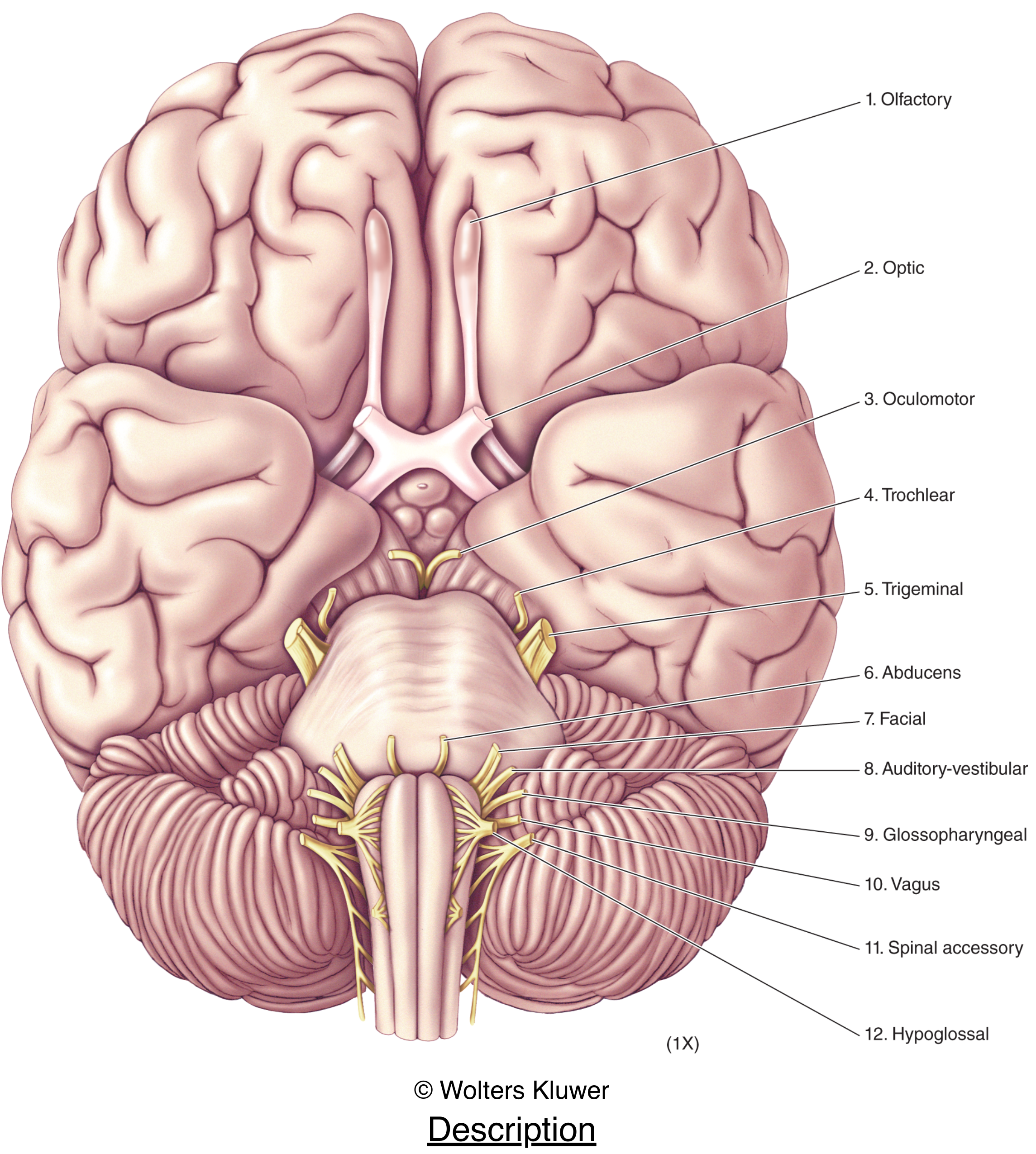
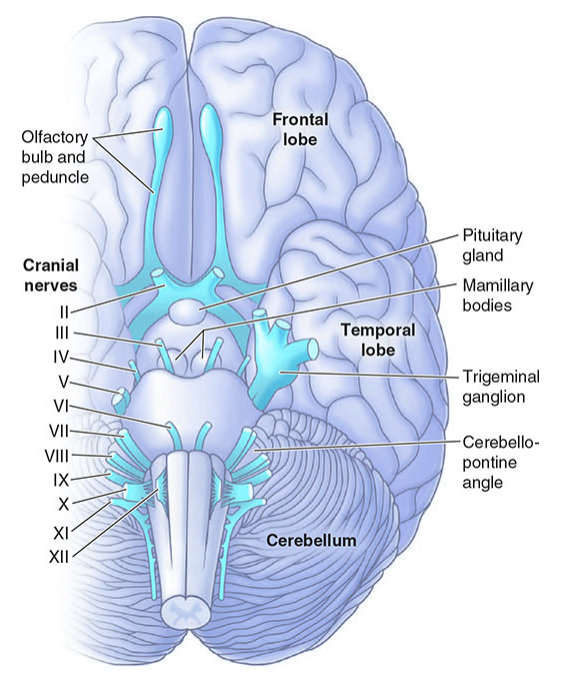
Twelve pairs of cranial nerves emerge from the base of the brain and exit the cranial cavity through foramina or fissures in the skull. CN I and II are technically CNS tracts (not true peripheral nerves), while CN III–XII are true peripheral nerves analogous to spinal nerves. All innervate head and neck structures; the vagus (X) descends far into thorax and abdomen. Four carry parasympathetic fibers: III, VII, IX, X.
Mnemonic: Names
Oh Oh Oh To Touch And Feel Very Good Velvet, Ah Heavens! (Olfactory, Optic, Oculomotor, Trochlear, Trigeminal, Abducens, Facial, Vestibulocochlear, Glossopharyngeal, Vagus, Accessory, Hypoglossal)
Mnemonic: Fiber Types (Sensory/Motor/Both)
Some Say Marry Money But My Brother Says Big Brains Matter More (S, S, M, M, B, M, B, S, B, B, M, M)
CN 0 — Nervus Terminalis (Terminal Nerve)
Often omitted from standard lists, CN 0 runs alongside CN I in the nasal septum. It is present in the human fetal brain but its role in adults is debated (possibly pheromone-related or vascular control). It has no established clinical testing. Textbooks occasionally note it in developmental and evolutionary neuroscience contexts.
CN I — Olfactory Nerve
- Fiber type: Special sensory (SVA)
- Origin: Olfactory receptor neurons (bipolar) in the olfactory epithelium (roof of nasal cavity)
- Pathway: Axons form the olfactory fila → pass through the cribriform plate of the ethmoid → synapse in the olfactory bulb → olfactory tract → primary olfactory cortex (piriform cortex, amygdala)
- Key fact: Only cranial nerve that does NOT relay through the thalamus before reaching cortex
- Foramen: Cribriform plate (numerous small foramina)
- Clinical test: Each nostril tested separately with familiar non-pungent odors (coffee, peppermint); avoid ammonia (CN V stimulation)
- Lesions: Anosmia (fracture of cribriform plate, meningioma of olfactory groove, head trauma, COVID-19); parosmia or phantosmia with partial lesions; Foster Kennedy syndrome = ipsilateral optic atrophy + anosmia + contralateral papilledema (frontal lobe/olfactory groove meningioma)
CN II — Optic Nerve
- Fiber type: Special sensory (SSA) — actually a CNS white matter tract
- Origin: Retinal ganglion cells → optic nerve → optic chiasm (nasal fibers decussate) → optic tract → lateral geniculate nucleus (thalamus) → optic radiations → primary visual cortex (V1, calcarine sulcus)
- Foramen: Optic canal (with ophthalmic artery)
- Clinical test: Visual acuity (Snellen chart), visual fields (confrontation testing), color vision, fundoscopy (disc, vessels, macula)
- Pupillary pathway: CN II afferent → pretectal nucleus → bilateral Edinger-Westphal nuclei → CN III efferent → sphincter pupillae (consensual + direct reflex)
- Key lesions by location:
| Location | Defect |
|---|---|
| Optic nerve (prechiasm) | Monocular blindness; RAPD (Marcus Gunn pupil) |
| Optic chiasm (midline compression — pituitary adenoma) | Bitemporal hemianopia |
| Optic tract | Contralateral homonymous hemianopia |
| Meyer's loop (temporal lobe) | "Pie in the sky" — contralateral superior quadrantanopia |
| Parietal lobe (dorsal optic radiation) | Contralateral inferior quadrantanopia |
| Occipital cortex | Contralateral homonymous hemianopia with macular sparing |
CN III — Oculomotor Nerve
- Fiber types: Somatic motor (GSE) + parasympathetic (GVE)
- Nucleus: Oculomotor nucleus (midbrain, at level of superior colliculus); Edinger-Westphal nucleus (parasympathetic)
- Muscles supplied: Superior rectus, inferior rectus, medial rectus, inferior oblique, levator palpebrae superioris
- Parasympathetic: Pre-ganglionic → ciliary ganglion → post-ganglionic → sphincter pupillae (miosis) + ciliary muscle (accommodation)
- Foramen: Superior orbital fissure (with IV, V1, VI)
- Course: Exits midbrain between PCA and SCA → travels in the lateral wall of the cavernous sinus → enters orbit through SOF
- Clinical test: Inspect ptosis, eye position; test H-pattern of gaze; pupil reaction
- Lesions:
- Complete CN III palsy: Eye is "down and out," ptosis, dilated non-reactive pupil (mydriasis — because parasympathetic fibers travel on the OUTSIDE of the nerve)
- Surgical CN III = posterior communicating artery (PCoA) aneurysm — pupil INVOLVED (compressed parasympathetics)
- Medical CN III = diabetes/hypertension (ischemic) — pupil SPARED (internal fibers spared by ischemia)
CN IV — Trochlear Nerve
- Fiber type: Somatic motor (GSE)
- Unique features: Only CN to exit the dorsal brainstem; longest intracranial course; thinnest CN; fully decussates before emerging
- Nucleus: Trochlear nucleus (midbrain, at level of inferior colliculus)
- Muscle supplied: Superior oblique (intorts, depresses, abducts the eye)
- Action: Depresses the eye when adducted ("looking at your nose tip")
- Foramen: Superior orbital fissure
- Clinical test: Head tilt test (Bielschowsky) — patient tilts head away from affected side to compensate
- Lesions: Vertical diplopia worse on looking down and in (e.g., reading, walking downstairs); head tilt toward opposite shoulder. Most common cause of isolated vertical diplopia. Often from closed head trauma (dorsal midbrain vulnerable).
CN V — Trigeminal Nerve
- Fiber types: Somatic sensory (GSA) + branchial motor (SVE) — the largest CN
- Nuclei:
- Main (principal) sensory nucleus (pons): fine touch, pressure
- Nucleus of spinal tract (extends from pons → cervical C2–4): pain and temperature
- Mesencephalic nucleus (midbrain): proprioception from jaw muscles
- Motor nucleus (pons): mastication muscles
- Gasserian (semilunar) ganglion: Sensory ganglion at apex of petrous bone in Meckel's cave
- Three divisions:
| Division | Foramen | Sensory Supply | Motor |
|---|---|---|---|
| V1 (Ophthalmic) | Superior orbital fissure | Forehead, scalp, cornea, upper eyelid, nose bridge, meninges | None |
| V2 (Maxillary) | Foramen rotundum | Cheek, lower eyelid, upper lip, upper teeth, palate | None |
| V3 (Mandibular) | Foramen ovale | Chin, lower lip, lower teeth, tongue, TMJ, EAC | Masseter, temporalis, pterygoids, tensor tympani, tensor veli palatini, mylohyoid, ant. digastric |
- Parasympathetics: CN III, VII, IX all hitch-hike on V branches (ciliary, pterygopalatine, submandibular, otic ganglia)
- Reflexes: Corneal reflex (V1 afferent, VII efferent), jaw-jerk reflex (V3 afferent + efferent)
- Clinical test: Facial sensation (V1/V2/V3 zones with cotton and pinprick), corneal reflex, jaw deviation (toward side of lesion if motor affected)
- Key lesions: Trigeminal neuralgia (tic douloureux — lancinating pain V2/V3, usually vascular compression), herpes zoster (ophthalmic division → rash on forehead + keratitis), acoustic neuroma (compresses at CPA), Meckel's cave tumors
CN VI — Abducens Nerve
- Fiber type: Somatic motor (GSE)
- Nucleus: Abducens nucleus (pons, floor of 4th ventricle) — also contains interneurons crossing to contralateral CN III for conjugate gaze
- Muscle supplied: Lateral rectus (abducts the eye)
- Foramen: Superior orbital fissure
- Course: Longest intracranial course running along the clivus → enters Dorello's canal → cavernous sinus → SOF. Most vulnerable CN to raised intracranial pressure (false localizing sign).
- Clinical test: Lateral gaze; horizontal diplopia (worse on ipsilateral gaze)
- Lesions: Esotropia, inability to abduct eye. Foville syndrome (pontine lesion = ipsilateral CN VI + VII + ipsilateral gaze palsy). Gradenigo syndrome (petrous apex infection = CN VI palsy + ipsilateral facial pain + otitis media).
CN VII — Facial Nerve
-
Fiber types: Branchial motor (SVE), somatic sensory (GSA), special sensory taste (SVA), parasympathetic (GVE) — "tears, snots, tastes, salivates, moves the face, and dampens sounds" (Localization in Clinical Neurology, 8e)
-
Nucleus: Facial motor nucleus (caudal pons, ventrolateral tegmentum)
-
Segments: (1) nucleus & fascicles, (2) cisternal, (3) intratemporal (fallopian canal), (4) peripheral
-
Motor branches (peripheral): Temporal, Zygomatic, Buccal, Marginal mandibular, Cervical (To Zanzibar By Motor Car)
-
Nervus intermedius (Wrisberg): Carries taste (anterior 2/3 tongue via chorda tympani → submandibular ganglion → sublingual & submandibular glands), lacrimation (via greater petrosal nerve → pterygopalatine ganglion → lacrimal gland), and sensation to external auditory canal
-
Foramen: Internal auditory meatus → facial canal in petrous bone → stylomastoid foramen
-
Critical anatomy: Facial nerve wraps around the abducens nucleus (genu) in the pons → lesion there = combined VI + VII palsy
-
LMN vs UMN facial palsy (HIGH-YIELD):
| Feature | LMN (e.g., Bell's palsy) | UMN (e.g., stroke) |
|---|---|---|
| Forehead spared? | No — entire face paralyzed | Yes — forehead spared (bilateral cortical supply) |
| Hyperacusis? | Yes (stapedius branch) | No |
| Taste affected? | Yes (if lesion proximal to chorda tympani) | No |
| Lacrimation affected? | Yes (if proximal) | No |
- Key lesions: Bell's palsy (idiopathic LMN, HSV-1 reactivation), Ramsay Hunt syndrome (herpes zoster, VZV, ear pain + vesicles + facial palsy), acoustic neuroma (CPA), parotid tumor (peripheral), Lyme disease, sarcoidosis, Guillain-Barré
CN VIII — Vestibulocochlear Nerve
- Fiber type: Special sensory (SSA) — two distinct components
- Foramen: Internal auditory meatus (with CN VII)
Cochlear Division (Hearing)
- Pathway: Hair cells of organ of Corti → spiral ganglion → cochlear nuclei (medullopontine junction) → dorsal/ventral acoustic striae → bilateral projections via lateral lemniscus → inferior colliculus → medial geniculate nucleus (thalamus) → auditory cortex (Heschl's gyri, superior temporal gyrus)
- Tonotopy: Low frequency = cochlear apex; high frequency = base
- Clinical test: Whisper test, Weber (tuning fork to vertex), Rinne (AC vs BC)
| Conductive loss | Sensorineural loss | |
|---|---|---|
| Weber | Lateralizes to affected ear | Lateralizes to unaffected ear |
| Rinne | BC > AC (negative Rinne) | AC > BC (positive Rinne, reduced) |
Vestibular Division (Balance)
- Receptors: Utricle & saccule (linear acceleration), cristae of semicircular canals (angular acceleration)
- Pathway: Scarpa's ganglion → vestibular nuclei (medulla/pons) → cerebellum, spinal cord (VST), MLF (conjugate eye movements), thalamus → cortex
- Clinical test: Head impulse test (HIT), Dix-Hallpike (BPPV), Romberg, gait
- Key lesions: Acoustic neuroma (vestibular schwannoma), Ménière's disease (episodic vertigo + tinnitus + fluctuating hearing loss + aural fullness), BPPV, labyrinthitis, presbycusis
CN IX — Glossopharyngeal Nerve
- Fiber types: Branchial motor (SVE), visceral motor parasympathetic (GVE), visceral sensory (GVA), general sensory (GSA), special sensory taste (SVA) — truly mixed
- Nuclei: Nucleus ambiguus (rostral, motor), inferior salivatory nucleus (parasympathetic), nucleus solitarius (taste/visceral sensory), spinal nucleus V (exteroception)
- Foramen: Jugular foramen (with X and XI)
- Ganglia: Superior and petrous (inferior) ganglia
- Key functions:
- Motor: stylopharyngeus muscle (pharyngeal elevator)
- Parasympathetic: inferior salivatory nucleus → tympanic nerve (Jacobson's nerve) → lesser petrosal nerve → otic ganglion → auriculotemporal nerve → parotid gland
- Sensory: posterior 1/3 tongue (taste + sensation), oropharynx, tonsils, tympanic membrane (Eustachian tube, mastoid via Jacobson's nerve)
- Carotid sinus nerve (nerve of Hering): Carries chemoreceptors from carotid body and baroreceptors from carotid sinus → nucleus solitarius → cardiovascular regulation
- Reflexes: Gag reflex (IX afferent, X efferent)
- Clinical test: Gag reflex, soft palate sensation, taste posterior tongue
- Key lesions: Glossopharyngeal neuralgia (lancinating throat/ear pain triggered by swallowing), jugular foramen syndrome (IX+X+XI), parotid gland surgery complications
CN X — Vagus Nerve
- Fiber types: Visceral motor parasympathetic (GVE), visceral sensory (GVA), branchial motor (SVE), somatic sensory (GSA)
- Nuclei:
- Dorsal motor nucleus of vagus (floor of 4th ventricle): preganglionic parasympathetics to thoracic/abdominal viscera (heart, lungs, gut to splenic flexure)
- Nucleus ambiguus: Motor to striated muscles of pharynx/larynx/soft palate
- Nucleus solitarius: Taste (epiglottis), visceral afferents
- Spinal nucleus V: Somatic sensation (external ear — nerve of Arnold)
- Foramen: Jugular foramen (in same dural sheath as CN XI)
- Ganglia: Jugular (somatic afferent) and nodose (visceral afferent)
- Key branches:
- Auricular branch (Arnold's nerve): skin of external ear + EAC → explains Arnold's reflex cough
- Pharyngeal ramus → pharyngeal plexus (motor to pharynx + soft palate except tensor veli palatini)
- Superior laryngeal nerve: external branch (cricothyroid motor) + internal branch (laryngeal sensory above vocal cords)
- Recurrent laryngeal nerve (RLN): All intrinsic laryngeal muscles except cricothyroid; left RLN loops under aortic arch (vulnerable to mediastinal pathology); right RLN loops under subclavian artery
- Clinical test: Palate elevation symmetry ("say aah" — uvula deviates away from lesion), hoarseness, gag reflex, voice quality
- Key lesions: Hoarseness (RLN palsy — thyroid surgery, lung cancer, aortic aneurysm), dysphagia, nasal regurgitation; autonomic dysfunction (cardiac, GI); vagal syncope
CN XI — Spinal Accessory Nerve
- Fiber type: Branchial motor (SVE) — purely motor
- Unique anatomy: Has spinal and cranial roots:
- Cranial root: nucleus ambiguus in medulla → exits skull via jugular foramen → joins vagus (contributes to pharyngeal/laryngeal muscles)
- Spinal root: anterior horn cells C1–C5/6 → ascends through foramen magnum → exits through jugular foramen → descends in neck
- Foramen: Jugular foramen
- Muscles supplied:
- Sternocleidomastoid (SCM): head rotation toward opposite side, ipsilateral flexion
- Trapezius (upper): shoulder shrug, scapular elevation
- Clinical test: Resist shoulder shrug (trapezius), resist head turning against resistance (SCM); note asymmetric trapezius bulk
- Lesions: Shoulder droop, winging of scapula, inability to shrug, weakness turning head to contralateral side; common cause = iatrogenic (posterior triangle lymph node biopsy, carotid endarterectomy)
CN XII — Hypoglossal Nerve
- Fiber type: Somatic motor (GSE) — purely motor
- Nucleus: Hypoglossal nucleus (paramedian medulla, beneath hypoglossal trigone, 4th ventricle floor); extends from caudal medulla to pontomedullary junction
- Course: Fibers emerge as 10–12 rootlets in the preolivary sulcus → hypoglossal canal (anterior condylar foramen) → descends in neck near internal carotid/IJ → turns medially toward tongue
- Ansa hypoglossi (ansa cervicalis): Descending ramus (C1 hitchhiking on CN XII) + descending cervical ramus (C2–C3) → supplies infrahyoid (strap) muscles
- Supranuclear control: Crossed corticobulbar fibers (mainly from contralateral cortex); genioglossus has crossed control (tongue deviates toward lesion in UMN injury)
- Muscles: All intrinsic tongue muscles + hyoglossus, styloglossus, genioglossus, geniohyoid
- Clinical test: Tongue at rest (fasciculations = LMN), tongue protrusion (deviates toward side of LMN lesion; deviates away from side of UMN lesion), tongue strength
- Lesions: LMN = ipsilateral atrophy + fasciculations + deviation toward lesion (e.g., skull base tumor, carotid dissection); UMN = deviation away from lesion (contralateral hemisphere lesion)
Master Summary Table
| CN | Name | Foramen | Fiber Types | Key Function | Clinical Test |
|---|---|---|---|---|---|
| 0 | Nervus terminalis | Cribriform plate | — | Unknown/pheromonal | None established |
| I | Olfactory | Cribriform plate | SVA | Smell | Coffee/peppermint test |
| II | Optic | Optic canal | SSA (CNS tract) | Vision | VA, fields, fundoscopy |
| III | Oculomotor | SOF | GSE, GVE | Most eye movements, lid, pupil | H-pattern, pupil light reflex |
| IV | Trochlear | SOF | GSE | Superior oblique (depression in adduction) | Vertical diplopia, Bielschowsky |
| V | Trigeminal | SOF (V1), FR (V2), FO (V3) | GSA, SVE | Face sensation, mastication | Cotton/pin face, jaw, corneal reflex |
| VI | Abducens | SOF | GSE | Lateral rectus (abduction) | Lateral gaze |
| VII | Facial | IAM → stylomastoid F | SVE, GVE, SVA, GSA | Facial expression, taste ant 2/3, lacrimation, salivation | Facial symmetry, taste |
| VIII | Vestibulocochlear | IAM | SSA | Hearing, balance | Weber, Rinne, HIT, Dix-Hallpike |
| IX | Glossopharyngeal | Jugular F | SVE, GVE, GVA, GSA, SVA | Taste post 1/3, gag, parotid, carotid sinus | Gag reflex |
| X | Vagus | Jugular F | GVE, GVA, SVE, GSA | Palate/larynx motor, visceral parasymp. | Palate elevation, voice |
| XI | Spinal accessory | Jugular F | SVE | SCM, trapezius | Shrug, head turn |
| XII | Hypoglossal | Hypoglossal canal | GSE | Tongue motor | Tongue protrusion |
SOF = superior orbital fissure; FR = foramen rotundum; FO = foramen ovale; IAM = internal auditory meatus
Parasympathetic Ganglia (High-Yield)
| CN | Pre-ganglionic nucleus | Ganglion | Target |
|---|---|---|---|
| III | Edinger-Westphal | Ciliary | Sphincter pupillae (miosis), ciliary muscle (accommodation) |
| VII | Superior salivatory | Pterygopalatine | Lacrimal gland, nasal/palatine glands |
| VII | Superior salivatory | Submandibular | Sublingual + submandibular salivary glands |
| IX | Inferior salivatory | Otic | Parotid gland |
| X | Dorsal motor nucleus | Terminal ganglia (in/near organs) | Heart, lungs, esophagus → transverse colon |
Key Brainstem Syndromes Involving Cranial Nerves
| Syndrome | Location | CNs Affected | Other Features |
|---|---|---|---|
| Weber | Midbrain (cerebral peduncle) | III (ipsilateral) | Contralateral hemiplegia |
| Claude | Midbrain (tegmentum) | III (ipsilateral) | Contralateral ataxia (red nucleus) |
| Benedikt | Midbrain | III (ipsilateral) | Contralateral ataxia + tremor |
| Millard-Gubler | Pons (ventral) | VI, VII (ipsilateral) | Contralateral hemiplegia |
| Foville | Pons (tegmentum) | VI, VII + gaze palsy (ipsilateral) | Contralateral hemiplegia |
| Gradenigo | Petrous apex | VI | Ipsilateral V1/V2 pain, otitis media |
| Lateral medullary (Wallenberg) | Medulla (PICA) | V, IX, X, XI (ipsilateral) | Ipsilateral Horner, contralateral spinothalamic loss, ataxia |
| Medial medullary (Dejerine) | Medulla (ASA) | XII (ipsilateral) | Contralateral hemiplegia + proprioceptive loss |
| Jugular foramen (Vernet) | Jugular foramen | IX, X, XI | Dysphagia, hoarseness, shoulder weakness |
| Collet-Sicard | Jugular + hypoglossal | IX, X, XI, XII | Above + tongue palsy |
Cavernous Sinus
The cavernous sinus contains CN III, IV, V1, V2, VI and the internal carotid artery. A cavernous sinus lesion (thrombosis, fistula, meningioma, pituitary apoplexy) can produce multiple ophthalmoplegia + V1/V2 sensory loss + Horner syndrome (sympathetics on ICA). CN VI is most vulnerable within the sinus (free-floating in venous blood, not embedded in wall).
Clinical Approach to Cranial Nerve Examination (Sequential)
- CN I — Smell each nostril; note anosmia
- CN II — VA (Snellen), color vision (Ishihara), fields (confrontation), pupils (direct/consensual, RAPD), fundoscopy
- CN II + III — Pupillary light reflex
- CN III, IV, VI — Eye position at rest, H-pattern pursuits (look for diplopia, ptosis, nystagmus)
- CN V — Face sensation (V1/V2/V3), corneal reflex, jaw open/clench/deviation
- CN VII — Raise eyebrows, close eyes tight, show teeth, puff cheeks, taste (anterior tongue)
- CN VIII — Whisper test, Weber/Rinne; vestibular: HIT, Dix-Hallpike, Romberg
- CN IX, X — Gag reflex, palate symmetry on phonation, voice quality (nasal, hoarse, breathy)
- CN XI — Shoulder shrug (trapezius), head rotation against resistance (SCM)
- CN XII — Tongue rest (fasciculations?), protrusion (deviation?), rapid side-to-side
Sources: Neuroscience: Exploring the Brain, 5th Ed. · Gray's Anatomy for Students · Localization in Clinical Neurology, 8e · Neuroanatomy through Clinical Cases, 3rd Ed. · Harrison's Principles of Internal Medicine, 21st Ed.
Create on summary image for fmge exam
Generating Image
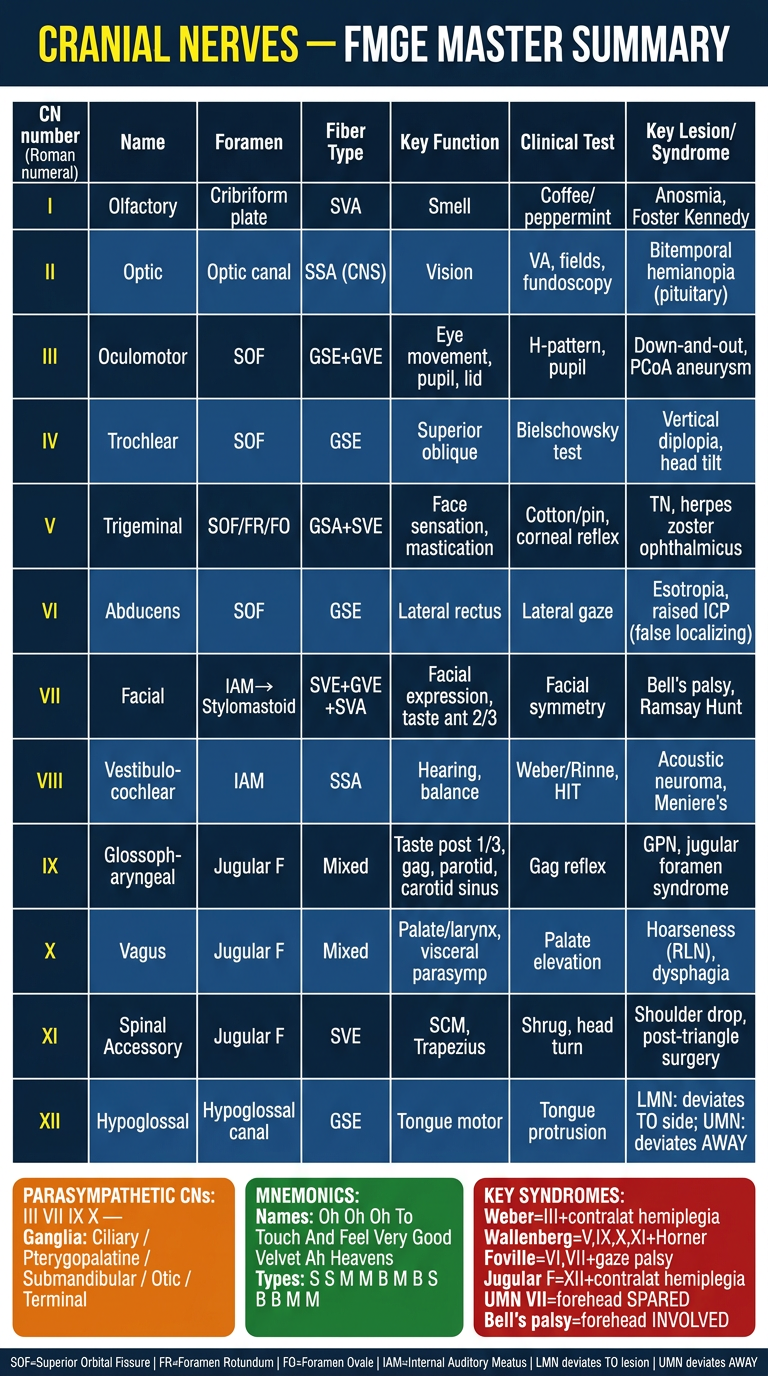
Here's your FMGE exam summary poster covering all 12 cranial nerves in one glance. It includes:
- Full table — CN number, name, foramen, fiber type, function, clinical test, and key lesion for every nerve
- Parasympathetic 4 — III, VII, IX, X with their ganglia
- Mnemonics — names and sensory/motor types
- High-yield syndromes — Weber, Wallenberg, Foville, Bell's palsy vs UMN facial, tongue deviation rules
- Foramen quick-reference footer
The most tested FMGE points are highlighted: pupil involvement in CN III palsy (surgical vs medical), forehead sparing in UMN VII, tongue deviation rules (LMN → TO lesion; UMN → AWAY), and false localizing sign for CN VI.
Create summary image with diagrams and everything in detail
Generating Image
Generating Image
Generating Image
Generating Image
Generating Image
Generating Image
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.