Explain me cubital fossa
Reading File
Finding Sources
Searching the Web
cubital fossa anatomy boundaries contents clinical significance
Reading File
Reading File
Loading Image
Reading File
Loading Image
Excellent - I now have comprehensive textbook content and diagrams. Here is the full explanation:
Cubital Fossa
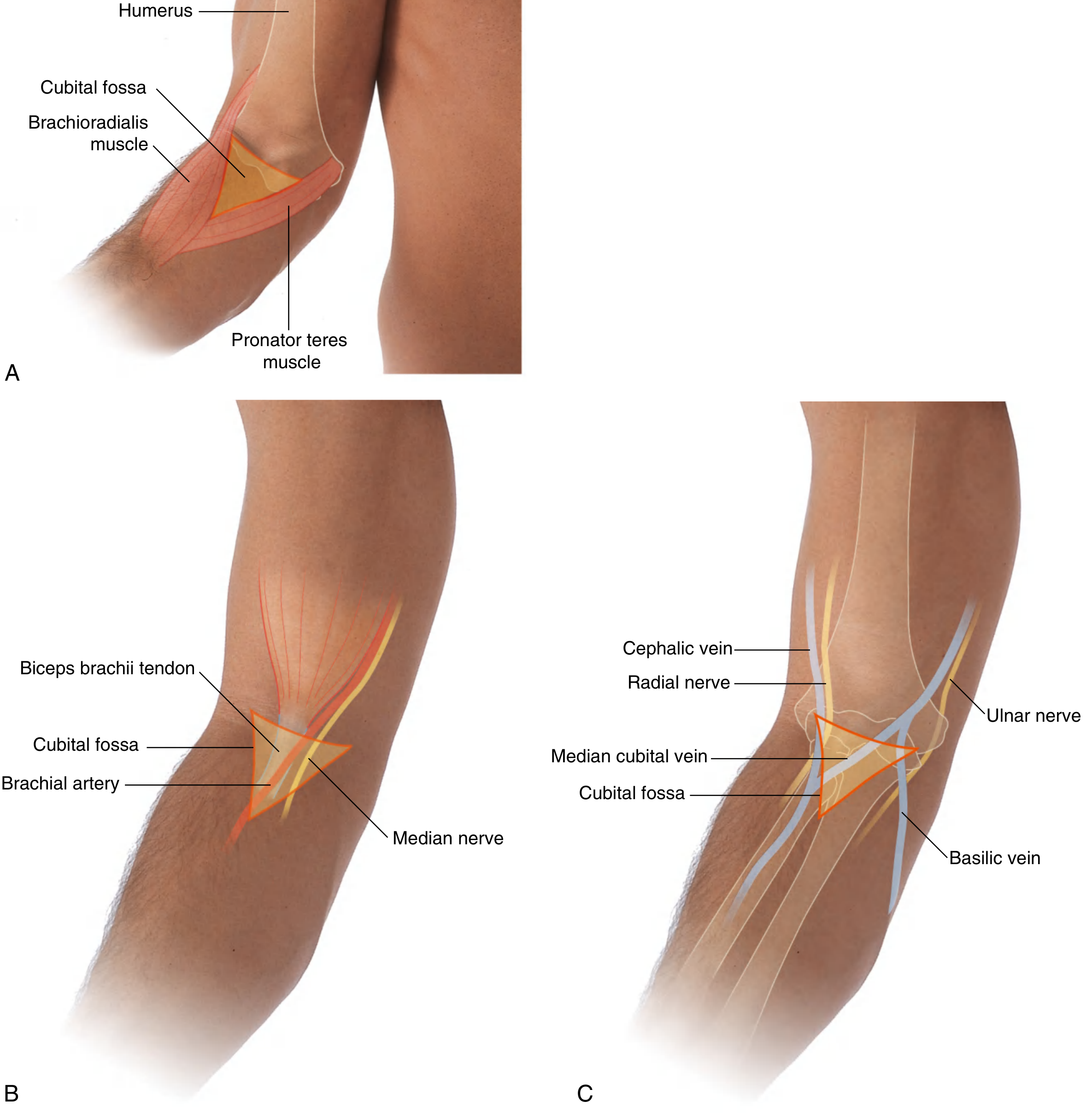
The cubital fossa (also called the antecubital fossa) is a triangular depression on the anterior aspect of the elbow joint. It is an important transition area between the arm and the forearm - most major neurovascular structures pass through it as they travel from the upper arm into the forearm.
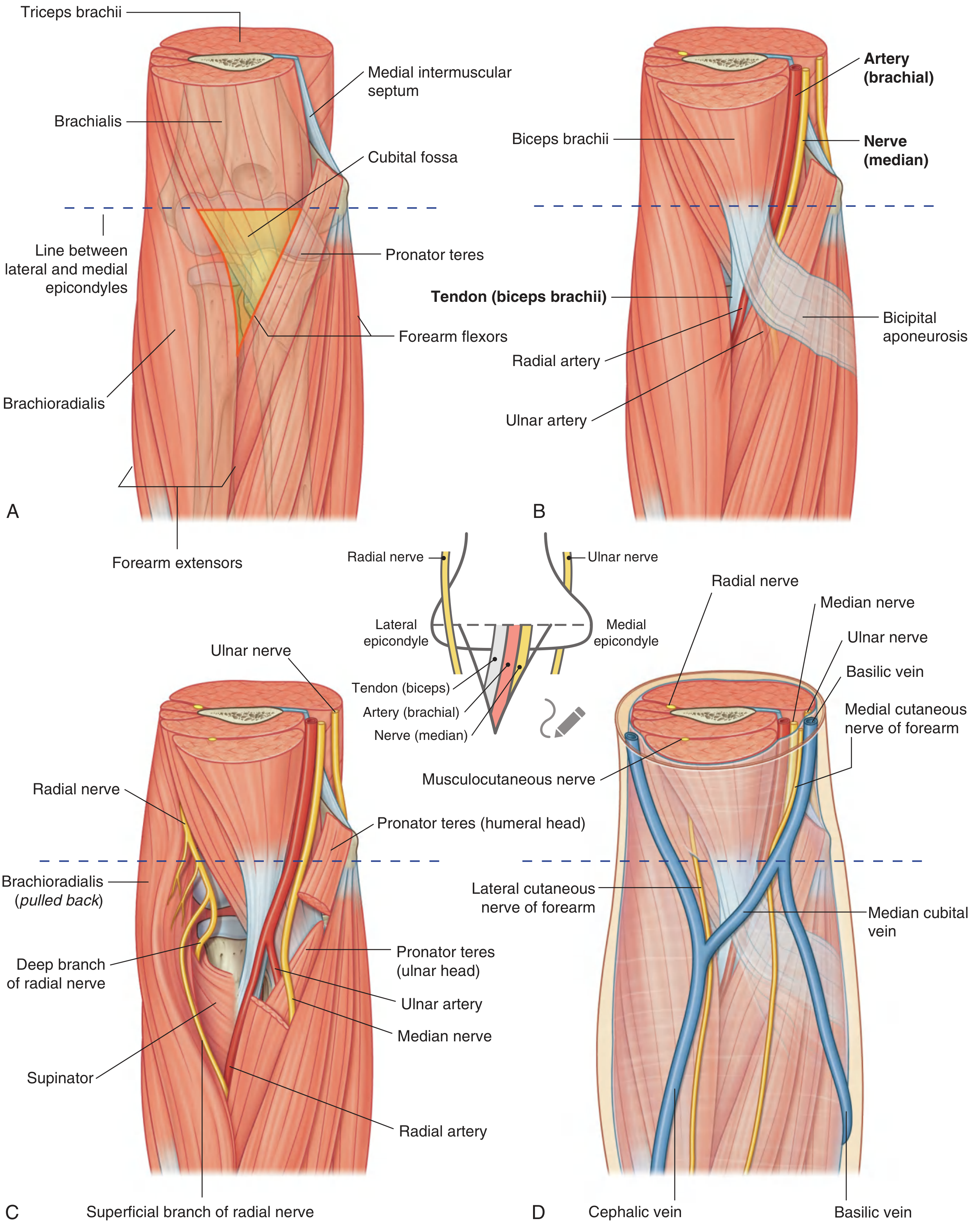
Boundaries
The fossa is triangular, so it has three borders + a roof and floor:
| Structure | Role |
|---|---|
| Imaginary line between medial and lateral epicondyles | Base (superior border) |
| Brachioradialis (from lateral supraepicondylar ridge) | Lateral border |
| Pronator teres (from medial epicondyle) | Medial border |
| The apex is where the two muscles meet distally | Apex (inferior) |
Practical tip: You can locate the lateral border (brachioradialis) by asking the patient to flex the semipronated forearm against resistance. The medial border (pronator teres) lies along an oblique line between the medial epicondyle and the midpoint of the lateral forearm surface.
Roof and Floor
- Roof (superficial to deep): Skin → superficial fascia (containing median cubital vein, lateral and medial cutaneous nerves of the forearm) → deep fascia → bicipital aponeurosis medially
- Floor: Mainly the brachialis muscle, with the supinator completing the floor laterally
The bicipital aponeurosis is a flat connective tissue membrane that sweeps from the medial side of the biceps tendon into the deep fascia of the forearm. It covers and protects the brachial artery and median nerve in the distal part of the fossa. Its sharp medial margin can often be felt on palpation.
Contents (Lateral to Medial)
The classic mnemonic is "TAN" - Tendon, Artery, Nerve:
| Structure | Notes |
|---|---|
| Biceps brachii tendon | Most lateral content; easily palpable; gives off the bicipital aponeurosis medially |
| Brachial artery | Medial to the tendon; bifurcates into the radial and ulnar arteries typically at the apex of the fossa |
| Median nerve | Most medial content; lies immediately medial to brachial artery; exits by passing between the two heads of pronator teres |
Additionally:
- Radial nerve - lies just under the lip of the brachioradialis at the lateral margin. It divides here into:
- Superficial branch - continues into the forearm deep to brachioradialis
- Deep branch - passes between the two heads of the supinator to enter the posterior compartment of the forearm
- Ulnar nerve - does NOT pass through the cubital fossa. It passes posterior to the medial epicondyle (where it can be rolled against the bone - the "funny bone").
Superficial Veins (in the Roof)
The subcutaneous fascia over the cubital fossa contains important superficial veins:
- Median cubital vein - connects the cephalic and basilic veins; crosses superficial to the bicipital aponeurosis (which protects the brachial artery beneath)
- Cephalic vein - lateral side
- Basilic vein - medial side
Clinical Significance
-
Blood pressure measurement - The stethoscope diaphragm is placed over the cubital fossa to auscultate the brachial artery while inflating the cuff above. The brachial pulse is also palpable here, medial to the biceps tendon.
-
Venipuncture / IV cannulation - The median cubital vein in the roof is the most commonly used site for drawing blood. The bicipital aponeurosis protects the brachial artery and median nerve from accidental puncture.
-
Dialysis fistula - The brachial artery can be surgically anastomosed to the cephalic vein at the elbow to create an arteriovenous fistula for hemodialysis (allowing flow rates of 250-500 mL/min required for dialysis).
-
Nerve injury risk - The radial nerve divides at the lateral border of the fossa. Lacerations or injections in this area can injure it. The median nerve is at risk from deep lacerations.
-
Elbow joint access - The brachial artery pulse can guide arterial line placement or confirm vascular integrity after elbow dislocations/fractures.
Source: Gray's Anatomy for Students, pp. 889-891 & 944-945
This is a shared conversation. Sign in to Orris to start your own chat.