
c44dd55b-32b7-44fa-982c-b9659fe7fec1.jpeg
Elaborate and explain
analyse_media
Reading File
Finding Sources
Searching the Web
genetic toxicity testing assays genotoxicity pharmacology drug development explained
Here is a thorough breakdown of everything covered in the image on Genetic Toxicity Testing:
Genetic Toxicity Testing (Genotoxicity Testing)
What Is It?
Genetic toxicity testing (genotoxicity testing) is a branch of preclinical safety pharmacology that evaluates whether a drug, chemical, or compound can damage genetic material - DNA, chromosomes, or the genome as a whole. Such damage can cause:
- Gene mutations - permanent changes in the DNA base sequence of a single gene
- Chromosomal aberrations - structural damage to chromosomes (deletions, inversions, translocations)
- DNA sequence alterations - broader changes in the arrangement or integrity of DNA
Genotoxic damage is concerning because it can lead to cancer (carcinogenesis), heritable genetic defects in offspring, or teratogenicity (birth defects).
Why It Is Done
- Regulatory requirement - All new drugs must pass genotoxicity tests before human clinical trials (with the notable exception for anticancer drugs explained below).
- Safety prediction - A genotoxic signal can predict carcinogenic potential long before expensive, time-consuming long-term carcinogenicity studies.
- Dose guidance - Helps set safe exposure limits in early human trials.
Test Systems Used
Genotoxicity is tested across multiple biological systems to catch different types of genetic damage:
| System | Examples |
|---|---|
| Microorganisms | Bacteria (e.g., Salmonella in the Ames test) |
| Plants | Tradescantia micronucleus assay |
| Mammalian cells (in vitro) | CHO cells, lymphocytes in culture |
| Whole animals (in vivo) | Rodents - mice and rats (preferred) |
Rodents are the preferred whole-animal model because their genetics are well understood, they are inexpensive to maintain, and decades of comparative data exist.
Specific Assays Described in the Text
1. Rodent Chromosome Assay (Chromosomal Aberration Test)
- Cells from rodents (typically bone marrow or peripheral blood) are examined under a microscope after drug exposure.
- Looks for broken or rearranged chromosomes.
- Detects clastogenic agents (those that break chromosomes).
2. Dominant Lethal Assay
This is the most nuanced assay mentioned. Here is the key concept broken down:
- A dominant lethal mutation is a genetic change that occurs inside a germ cell (sperm or egg).
- Crucially, the mutation does NOT kill the germ cell itself - the sperm/egg still functions and can fertilize.
- However, after fertilization, the resulting embryo inherits the mutated DNA and dies early (pre-implantation or post-implantation death).
- How it works in practice: Male rodents are exposed to the test drug, then mated with unexposed females. The females are later examined for the number of dead implants, early fetal deaths, and reduced litter sizes - all indicators of dominant lethal mutations in the male's sperm.
- What it detects: DNA strand breaks, chromosomal damage in germ cells - especially relevant for assessing risk of heritable mutations.
3. Mouse Specific Locus Test
- Exposes mice to the test compound and then looks for mutations at specific, easily visible gene loci (e.g., coat color genes).
- If mutations arise, the offspring show observable phenotypic changes (like a different coat color).
- A direct, in vivo measure of gene mutation frequency in germ cells.
4. Micronucleus Test
- One of the most widely used and internationally recognized genotoxicity tests.
- After cell division, chromosomal fragments or whole chromosomes that were not incorporated into the main nucleus form small separate nuclei called micronuclei.
- Increased micronuclei in bone marrow erythrocytes (immature red blood cells) of rodents = evidence of chromosomal damage or spindle disruption.
- Simple, fast, and highly reliable.
5. Heritable Translocation Assay
- Checks whether a drug causes chromosomal translocations (pieces of chromosomes swapping places) that are passed on to offspring.
- Male mice are exposed to the drug, mated, and the resulting offspring (F1 generation) are examined for reduced fertility, which signals a balanced translocation inherited from the father.
- Detects transmissible chromosomal structural damage.
6. Sister Chromatid Exchange (SCE) Assay
- During DNA replication, the two identical copies of a chromosome (sister chromatids) normally do not exchange segments.
- Genotoxic agents cause abnormal swapping of DNA segments between sister chromatids.
- Detected using special staining techniques (differential staining after BrdU incorporation).
- A very sensitive indicator of DNA strand breakage and repair activity - even low-level genotoxic exposure can elevate SCE frequency.
Special Rule for Anticancer Drugs
The text makes an important regulatory note:
"Genotoxic data of an anticancer drug is not required until it passes Phase 2 trial."
This exception exists because:
- Many anticancer drugs are intentionally genotoxic - they work by damaging the DNA of rapidly dividing cancer cells (e.g., alkylating agents, topoisomerase inhibitors).
- Requiring full genotoxicity data before Phase 1/2 would prevent potentially life-saving drugs from being tested in terminal patients.
- The risk-benefit calculation shifts significantly when the patient has cancer vs. a healthy volunteer or a patient with a minor condition.
- Once Phase 2 demonstrates efficacy, full genotoxicity profiling is then required before broader Phase 3 trials.
Summary Table of Assays
| Assay | What It Detects | In vivo / In vitro |
|---|---|---|
| Rodent Chromosome Assay | Chromosomal breaks/rearrangements | In vivo |
| Dominant Lethal Assay | Germ cell DNA damage causing embryo death | In vivo |
| Mouse Specific Locus Test | Gene point mutations in germ cells | In vivo |
| Micronucleus Test | Chromosomal breakage / spindle damage | In vivo (bone marrow) |
| Heritable Translocation Assay | Transmissible chromosomal translocations | In vivo |
| Sister Chromatid Exchange (SCE) | DNA strand breaks / repair | In vitro or In vivo |
This topic sits within preclinical toxicology and is directly relevant to pharmacology, drug development regulations (ICH S2 guidelines), and understanding how candidate drugs are screened for cancer-causing potential before they ever reach humans.
How do these assays differ from in vitro vs in vivo testing?

1000646462.jpg
Provisional diagnosis
Finding Sources
Finding Sources
analyse_media
Finding Sources
Finding Sources
Searching the Web
in vitro vs in vivo genotoxicity assays differences advantages limitations ICH S2
Searching the Web
leukocytosis neutrophilia 74 year old male differential diagnosis bacterial infection
I'll address both questions together - the in vitro vs in vivo comparison, and the CBC interpretation with a provisional diagnosis.
Part 1: In Vitro vs In Vivo Genotoxicity Assays
The Core Distinction
| Feature | In Vitro | In Vivo |
|---|---|---|
| Setting | Test tube / cell culture / bacterial plate | Living animal (usually rodent) |
| System | Isolated cells, bacteria, or cell lines | Whole organism with intact physiology |
| Metabolism | Often absent or artificially added (S9 mix) | Full metabolic processing by liver, gut, etc. |
| Cost | Low | High |
| Speed | Days | Weeks to months |
| Regulatory weight | Screening level | Confirmatory / definitive |
In Vitro Assays - Explained
These tests expose isolated cells or bacteria to the drug outside of a living organism.
Ames Test (Bacterial Reverse Mutation Assay)
- Uses specially engineered strains of Salmonella typhimurium and E. coli that cannot grow without histidine.
- If the drug causes a gene mutation that "reverses" this defect, the bacteria grow - counted as colonies.
- Fast, cheap, and the gold standard first-line screen for point mutations.
- Limitation: Bacteria lack human metabolism. A "pro-mutagen" (a drug that becomes toxic only after liver metabolism) may be missed. To address this, a rat liver extract called S9 mix is added to mimic hepatic metabolism.
In Vitro Chromosomal Aberration Test
- Human or Chinese hamster ovary (CHO) cells are grown in culture and exposed to the drug.
- Cells are arrested in metaphase and chromosomes are examined under microscope for breaks, deletions, or rearrangements.
- Detects clastogens (chromosome-breaking agents).
In Vitro Micronucleus Test
- Cells are exposed to the drug and examined after division.
- Micronuclei (tiny fragments of broken chromosomes or entire lagging chromosomes) are counted.
- Detects both clastogens (chromosome breakers) and aneugens (agents that disrupt the spindle, causing whole chromosomes to be lost).
Mouse Lymphoma tk Assay
- Uses mouse lymphoma cells with one functional copy of the thymidine kinase (tk) gene.
- Mutations in this gene allow cells to survive in a selective medium - colonies indicate mutagenic activity.
- Sensitive to a wide range of mutation types.
Key limitation of ALL in vitro tests: High false-positive rate, especially in mammalian cell assays. Cytotoxic concentrations can cause chromosomal damage that is not relevant to real human exposure - hence the ICH S2(R1) guideline caps the top test concentration at 1 mM or 0.5 mg/mL.
In Vivo Assays - Explained
These are conducted in living animals (rodents), where the drug is metabolized, distributed, and excreted just as it would be in humans.
Why In Vivo Matters
- Metabolism is real - the liver converts the drug into active or inactive metabolites naturally.
- DNA repair mechanisms are intact and functional.
- Pharmacokinetics (absorption, distribution) affect how much drug actually reaches target cells.
- A drug that looks genotoxic in vitro may be harmless in vivo because it is rapidly detoxified, cannot penetrate cells, or is repaired efficiently.
Rodent Bone Marrow Micronucleus Test (In Vivo)
- Rodents are given the drug, and bone marrow cells (erythrocytes) are examined for micronuclei.
- The bone marrow is used because it divides rapidly, and immature red blood cells (polychromatic erythrocytes) lack a nucleus - making micronuclei easy to spot.
- The most widely accepted in vivo confirmatory test.
Comet Assay (Single Cell Gel Electrophoresis)
- Individual cells from any tissue are embedded in gel and subjected to electrophoresis.
- Damaged (broken) DNA strands migrate away from the nucleus, forming a "comet tail."
- The longer the tail, the more DNA strand breakage.
- Can be performed on any tissue (liver, stomach, lung) - useful when testing a drug that concentrates in a specific organ.
- Often paired with the micronucleus test in vivo to satisfy ICH S2(R1) requirements.
Dominant Lethal, Heritable Translocation, Specific Locus Test
- As described in your textbook - these target germ cells specifically, assessing whether mutations can be passed to future generations.
- Critical for reproductive toxicology.
ICH S2(R1) Standard Battery (Regulatory Requirement)
The global regulatory standard defines two testing options:
Option 1:
- Ames test (bacterial mutation, in vitro)
- In vitro chromosomal aberration OR micronucleus test (mammalian cells)
- One in vivo test (usually bone marrow micronucleus)
Option 2:
- Ames test (in vitro)
- Two in vivo tests in two different tissues (e.g., micronucleus + comet in liver)
If in vitro results are positive, in vivo testing must follow to determine if the finding is a true risk or a false positive.
Summary: Why Both Are Needed
In Vitro → Fast, cheap, sensitive screening
BUT: high false positives, no real metabolism, no repair
In Vivo → Slower, costly, but reflects true biological reality
Confirms or refutes in vitro signals
Considers metabolism, repair, pharmacokinetics
A drug is considered genotoxic only when both in vitro AND in vivo evidence align. A positive in vitro result alone is not sufficient to condemn a drug - it triggers further in vivo investigation.
Part 2: CBC Report - Provisional Diagnosis
Patient: Mr. Ashwani Kumar Singla, 74-year-old male | Reported 12 July 2026
Abnormal Findings at a Glance
| Parameter | Result | Reference | Status |
|---|---|---|---|
| Total WBC | 11,800 /cumm | 4000-11000 | HIGH |
| Neutrophils % | 86% | 50-70% | HIGH |
| Lymphocytes % | 10% | 25-50% | LOW |
| Absolute Neutrophil Count | 10,148 /cumm | 2000-7000 | HIGH |
| Haemoglobin | 12.2 g/dL | 12-17 | Low-normal |
| Platelets | 1.58 lakh/cumm | 1.50-4.10 | Low-normal |
| RBC indices (MCV, MCH, MCHC, RDW) | All normal | - | Normal |
Interpretation of the Pattern
1. Leukocytosis with Marked Neutrophilia
- WBC of 11,800 with 86% neutrophils = absolute neutrophil count of 10,148 - nearly 1.5x the upper limit of normal.
- This pattern - elevated total WBC driven almost entirely by neutrophils - is the classic response to acute bacterial infection or significant tissue inflammation/stress.
- The neutrophilia is not extreme enough to suggest a primary haematological malignancy (e.g., CML typically causes WBC >50,000 with a "left shift" showing immature forms like bands, metamyelocytes).
2. Relative Lymphopenia (10%)
- Lymphocytes are suppressed to 10% (absolute count 1,180, which is actually low-normal).
- Relative lymphopenia in the setting of neutrophilia is expected - it does NOT indicate a primary lymphocyte problem. The neutrophils are "crowding out" the percentage.
- This pattern is typical of: acute stress response, bacterial sepsis, corticosteroid use, or acute severe illness.
3. Haemoglobin 12.2 g/dL (Low-Normal for a 74-year-old Male)
- While technically within the male reference range (12-17), a Hb of 12.2 in a 74-year-old man is concerning.
- WHO defines anaemia in adult males as Hb <13 g/dL. By this standard, this patient has mild anaemia.
- The RBC indices are normocytic normochromic (MCV 82.7, MCH 27, MCHC 32.6, RDW 13.9) - pointing toward anaemia of chronic disease or early iron deficiency rather than B12/folate deficiency.
4. Platelets 1.58 lakh/cumm (Low-Normal)
- Within range but at the lower end. Should be monitored. Not thrombocytopenic.
Provisional Differential Diagnosis
Most Likely:
- Acute Bacterial Infection - pneumonia, urinary tract infection, cholangitis, or bacteraemia - is the most probable cause of leukocytosis + neutrophilia in a 74-year-old. Elderly patients often have atypical presentations (no fever, minimal symptoms).
- Systemic Inflammatory Response - post-procedure, post-fall injury, or tissue necrosis (e.g., myocardial infarction, bowel ischemia).
Must Rule Out:
3. Early Chronic Myeloid Leukaemia (CML) or Myeloproliferative disorder - though the WBC is only mildly elevated at 11,800. Peripheral smear should be examined for left shift, blast cells, or basophilia.
4. Medication effect - corticosteroids, beta-agonists, lithium, or colony-stimulating factors all cause neutrophilia.
5. Reactive neutrophilia from stress - acute physiological or emotional stress in the elderly.
Recommended Next Steps
- Clinical correlation is essential - what symptoms does the patient have? (Fever, cough, dysuria, abdominal pain, chest pain?)
- Peripheral blood smear - to look for toxic granulation, Dohle bodies (infection), or immature myeloid cells (leukaemia).
- CRP / Procalcitonin - elevated in bacterial infection; helps differentiate from non-infectious causes.
- Blood cultures if bacteraemia is suspected.
- Urine routine and culture - UTI is the most common infection in elderly males causing these findings.
- Chest X-ray - to rule out pneumonia.
- LFTs, serum ferritin, iron studies - to characterize the mild anaemia.
Important note: This analysis is for educational purposes only. Clinical correlation, full history, examination findings, and further investigations are required before any diagnosis or treatment decision.

8a18f5bf-6751-4bd1-9572-54a397767b15.jpeg
Explain it
Finding Sources
Searching the Web
Cre loxP tissue specific knockout mice mechanism explained floxed gene
Reading File
Reading File
Loading Image
Here is a thorough explanation of Tissue-Specific Knockout Mice using the Cre/loxP system.
Tissue-Specific Knockout Mice: The Cre/loxP System
The Problem It Solves
Traditional knockout mice have a gene deleted in every single cell from conception. This creates two problems:
- If the gene is essential for early development, the mouse dies as an embryo - you never get to study the gene's role in adults.
- You cannot determine which tissue the gene's effects come from. For example, if you knock out an insulin receptor gene everywhere, you cannot tell whether the effects are from muscle, liver, or brain.
The Cre/loxP system solves both problems by deleting a gene only in the target tissue, leaving it intact everywhere else.
The Two Components: Cre and loxP
loxP Sites
- loxP stands for "locus of X-over of P1" - named after bacteriophage P1, where this system was first discovered.
- A loxP site is a short, specific 34 base-pair DNA sequence that does NOT naturally exist in mouse or human genomes - it must be artificially inserted.
- Two loxP sites are inserted flanking (one on each side of) the gene exon you want to delete. A gene sandwiched between two loxP sites is called a "floxed" gene (flanked by loxP).
- The floxed gene is fully functional - the loxP sites do not disrupt its expression on their own.
Cre Recombinase
- Cre (Cyclization Recombinase) is an enzyme originally produced by bacteriophage P1 (a virus that infects E. coli).
- Cre is a site-specific recombinase - it recognizes loxP sequences specifically and cuts the DNA at those sites.
- When Cre encounters two loxP sites on the same DNA molecule, it cuts both sites and loops out and excises the DNA between them - permanently deleting the gene sandwiched in between.
- The result: the target exon is precisely and irreversibly removed, silencing that gene.
Before Cre acts:
——[loxP]——[TARGET GENE EXON]——[loxP]——
↓ Cre cuts both loxP sites
After Cre acts:
——[loxP]—— (gene is gone, only one loxP remains)
How Tissue Specificity Is Achieved
The key insight: Cre is placed under the control of a tissue-specific promoter.
- A promoter is the "switch" region of DNA that controls when and where a gene is turned on.
- If you attach Cre to a promoter that only activates in, say, liver cells, then Cre will only be produced in liver cells.
- Cre only acts where it is expressed - so the floxed gene is only deleted in that one tissue.
Example: Attach Cre to the albumin promoter (which is active only in liver cells) → Cre is only made in liver → only liver cells delete the floxed gene → every other tissue in the body retains normal gene function. This is called a conditional knockout.
The Two-Mouse Breeding Strategy
Two separate mouse lines must be created and then bred together:
Mouse Line 1: The "Floxed Mouse" (Cre-Deletor Mouse)
- A mouse engineered to carry the target gene flanked by loxP sites on both chromosomes.
- This mouse looks and behaves completely normally because loxP sites do not affect gene function.
- Written as: Exon^fl/fl (homozygous floxed)
Mouse Line 2: The "Cre Mouse" (Cre-Deleter Mouse)
- A mouse that expresses Cre recombinase from a tissue-specific promoter.
- The Cre gene is present and active only in the desired tissue (e.g., neurons, cartilage, heart muscle, etc.).
- This mouse also looks normal because it does not have any floxed gene to delete.
The Breeding Cross
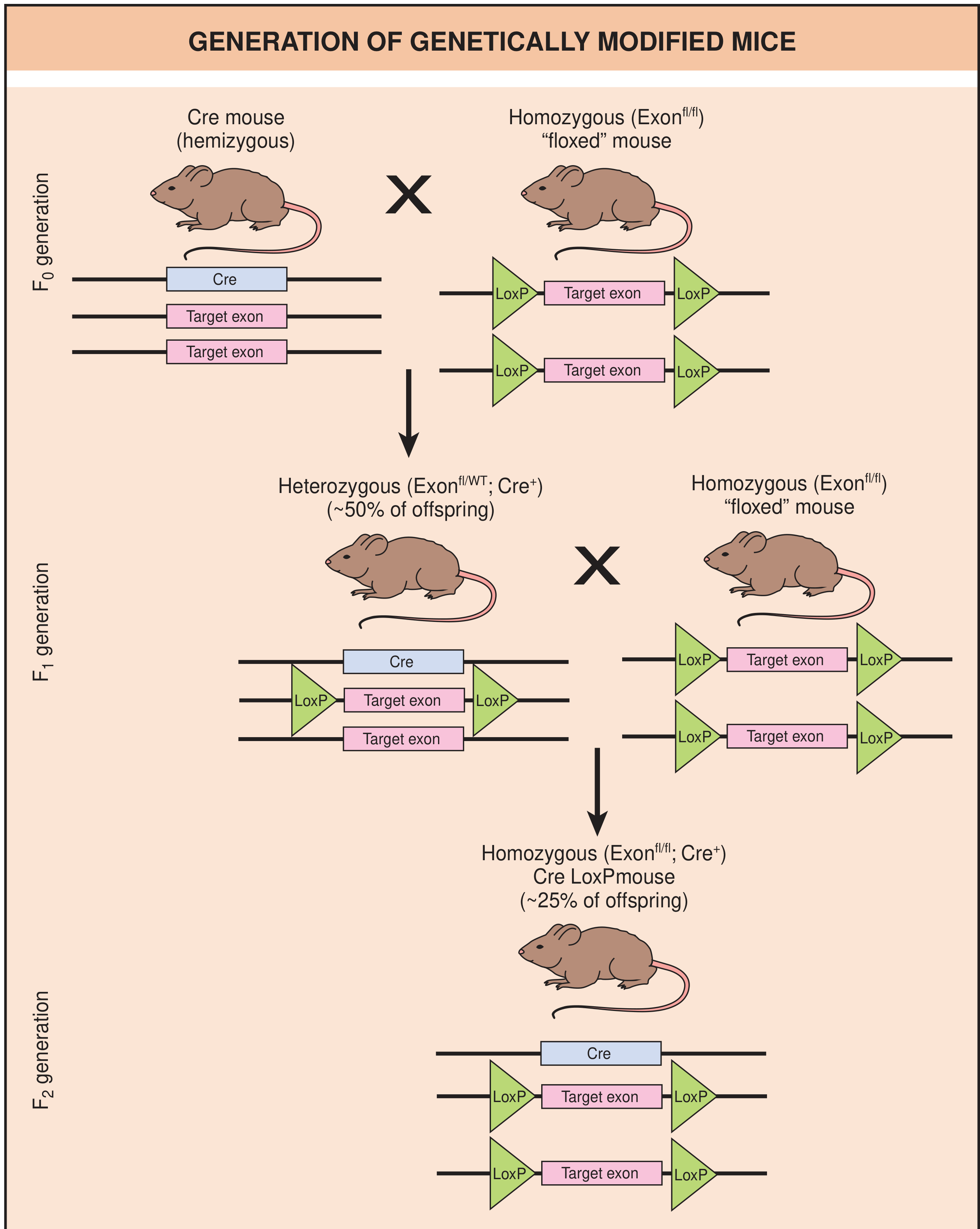
The diagram above (from Rheumatology textbook, Elsevier 2022) shows the three-generation breeding scheme:
F0 Generation:
- Cre mouse (hemizygous) × Floxed mouse (homozygous, Exon^fl/fl)
- All offspring carry one floxed allele and ~50% also carry the Cre gene.
F1 Generation:
- F1 mice that are Exon^fl/WT; Cre+ are bred back to homozygous floxed mice (Exon^fl/fl)
- This produces mixed litters.
F2 Generation - The Target Mouse:
- ~25% of F2 offspring are homozygous floxed AND carry Cre (Exon^fl/fl; Cre+)
- In these mice: wherever the tissue-specific promoter activates Cre → Cre enzyme cuts the loxP sites → target exon is looped out and deleted → that tissue has no functional copy of the gene.
- Every other tissue: gene intact and working normally.
The "Knock-in" Technology Mention
The text mentions these mice are also produced by "knock-in" technology. This refers to a related approach where instead of just deleting a gene, you insert (knock in) a new or modified gene sequence at a precise chromosomal location - often used to introduce human disease mutations into mice to model genetic diseases.
Why This Matters: Applications
| Application | Example |
|---|---|
| Study gene function in one organ | Delete insulin receptor only in brain to study diabetes and cognition separately |
| Avoid embryonic lethality | Many genes essential for development can be studied in adult tissue if deleted only later |
| Disease modeling | Delete cartilage-specific genes in joints to study osteoarthritis |
| Cancer research | Delete tumor suppressor genes only in specific tissues to generate organ-specific cancer models |
| Neuroscience | Delete synaptic genes in specific brain regions (e.g., hippocampus) to study memory |
Summary in Simple Steps
- Identify the gene you want to knock out in a specific tissue.
- Flank it with loxP sites using embryonic stem cell engineering → create the "floxed mouse."
- Generate a Cre mouse that expresses Cre only in your target tissue using a tissue-specific promoter.
- Breed the two lines together.
- Offspring that carry both the floxed gene AND the Cre gene will have their target gene silenced only in that specific tissue - a conditional tissue-specific knockout.
This system earned Mario Capecchi, Martin Evans, and Oliver Smithies the Nobel Prize in Physiology or Medicine in 2007, recognizing it as one of the most powerful tools in biomedical research. - Rheumatology, 2-Volume Set (Elsevier 2022), Principles of Neural Science, 6th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.