Excellent content gathered. Now I have everything needed for a comprehensive answer. Let me compile it.
Giant Cells in Pathology
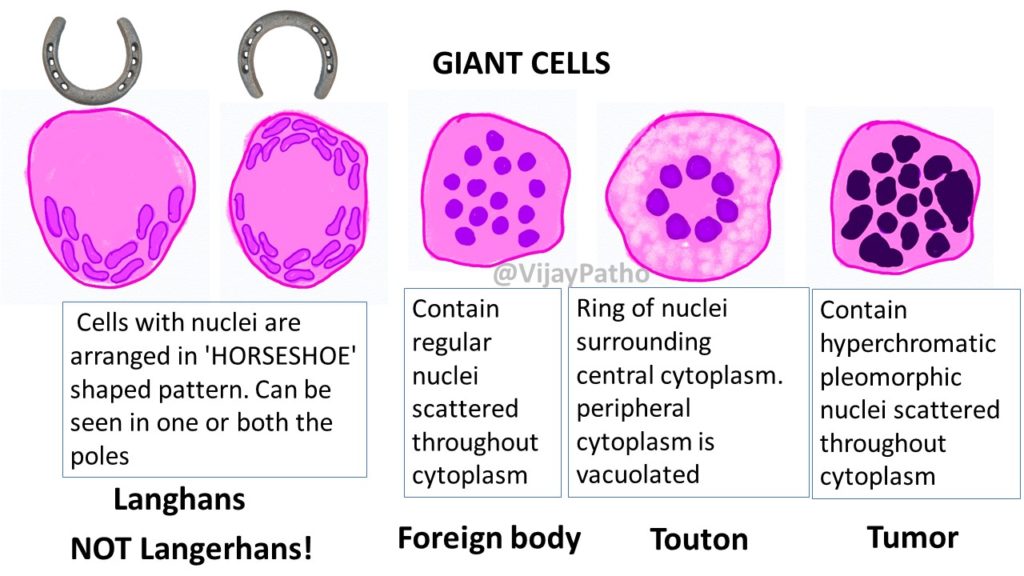
Giant cells form by fusion of macrophages/histiocytes (or occasionally other cells) and are large, multinucleated cells. They are a hallmark of granulomatous inflammation and several specific diseases.
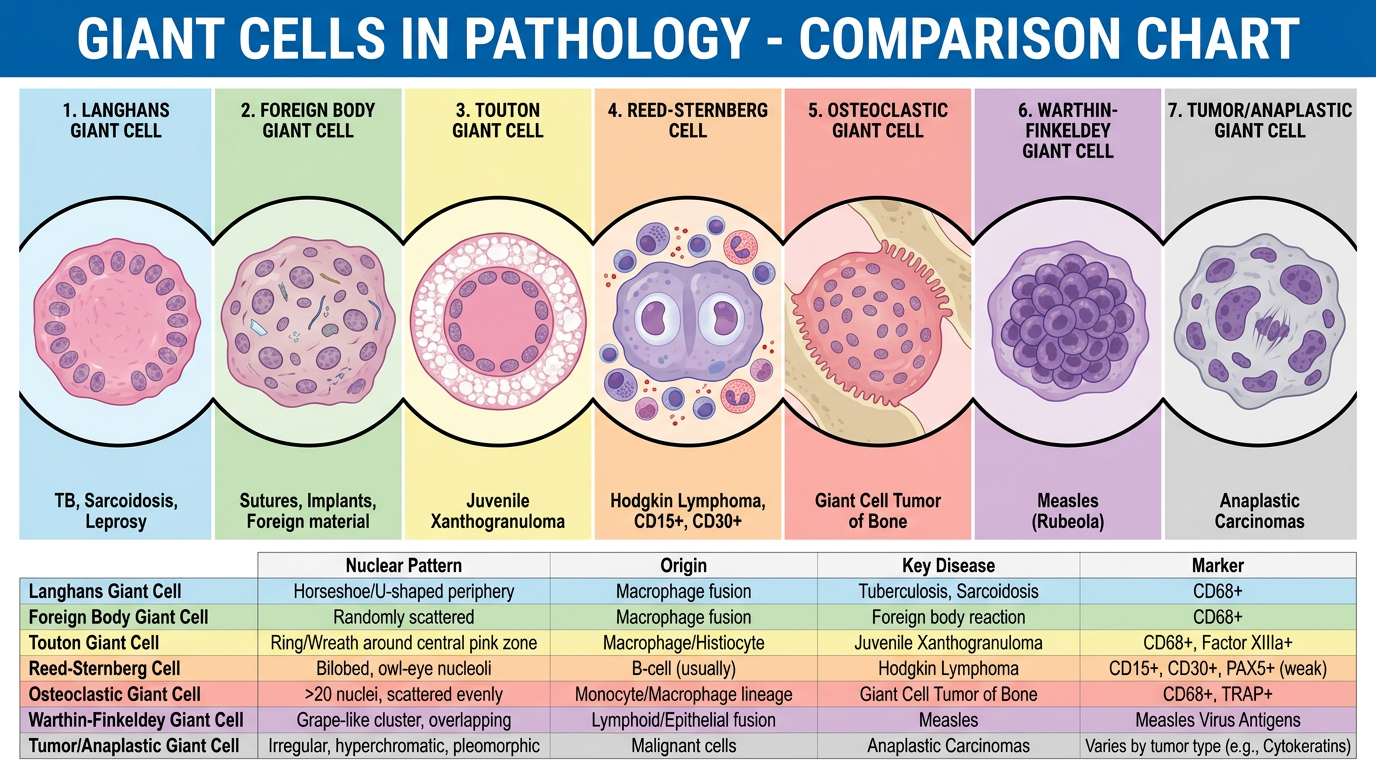
Diagram - Types of Giant Cells
Key memory aid: Langhans = horseshoe nuclei; Foreign body = scattered nuclei; Touton = ring of nuclei with peripheral foam; Tumor = hyperchromatic pleomorphic scattered nuclei
1. Langhans Giant Cell
NOT to be confused with Langerhans cell (of skin/immune system)
| Feature | Detail |
|---|
| Origin | Fusion of epithelioid macrophages |
| Nucleus arrangement | Horseshoe- or U-shaped arrangement at the periphery / one or both poles |
| Cytoplasm | Abundant eosinophilic |
| Size | Large, 40-50 µm |
Where they occur:
- Tuberculosis (most classic)
- Leprosy (tuberculoid/borderline)
- Sarcoidosis
- Crohn disease
- Berylliosis
- Syphilis
- Fungal infections (histoplasmosis, coccidioidomycosis)
- Wegener granulomatosis
Special points:
- Associated with T-cell mediated (type IV hypersensitivity) granulomas
- Found in "tuberculoid granulomas" - compact aggregates of epithelioid histiocytes rimmed by lymphocytes
- NOT exclusive to TB - any caseating or non-caseating granuloma can have them
Clinical significance: Seeing Langhans cells on biopsy triggers workup for TB, sarcoidosis, and other granulomatous diseases
2. Foreign Body Giant Cell
| Feature | Detail |
|---|
| Origin | Fusion of macrophages around non-immunogenic material |
| Nucleus arrangement | Randomly scattered throughout cytoplasm (haphazardly distributed) |
| Cytoplasm | May contain the engulfed foreign material |
| Size | Very large |
Where they occur:
- Around exogenous materials: sutures, splinters, talc, silica, silicone, tattoo pigment, aesthetic fillers
- Around endogenous materials: urate crystals (gout), calcium oxalate, cholesterol crystals (cholesteatoma), keratin (ruptured cysts)
- Surgical wounds
- Berylliosis
Special points:
- Surrounded by histiocytes, lymphocytes, fibroblasts = foreign body granuloma
- Polarization microscopy essential to identify birefringent foreign material within them
- More "reactive" than immunological - appear faster (days to weeks) and with less T-cell involvement
- Can have 50-100+ nuclei
Clinical significance: Indicates an inert foreign material reaction. Important after surgery, dermal fillers, tattoos
3. Touton Giant Cell
| Feature | Detail |
|---|
| Origin | Fusion of lipid-laden macrophages (foam cells) |
| Nucleus arrangement | Ring/wreath of nuclei around central homogeneous eosinophilic cytoplasm, with outer rim of foamy/vacuolated cytoplasm |
| Cytoplasm | Three zones: central homogeneous pink → ring of nuclei → peripheral foamy (lipid-laden) |
| Hallmark | "Wreath-like" ring of nuclei + peripheral foam |
Where they occur:
- Juvenile xanthogranuloma (JXG) - most characteristic
- Xanthoma
- Necrobiotic xanthogranuloma
- Dermatofibroma (occasionally)
- Reticulohistiocytosis
- Xanthomatous conditions generally
Special points:
- Touton cells are characteristic of JXG but NOT pathognomonic (not specific)
- The peripheral foamy cytoplasm distinguishes them from Langhans or foreign body types
- Reflect lipid engulfment by macrophages
Clinical significance: Presence in a skin biopsy strongly suggests a xanthogranulomatous process; in JXG, ocular involvement can threaten vision
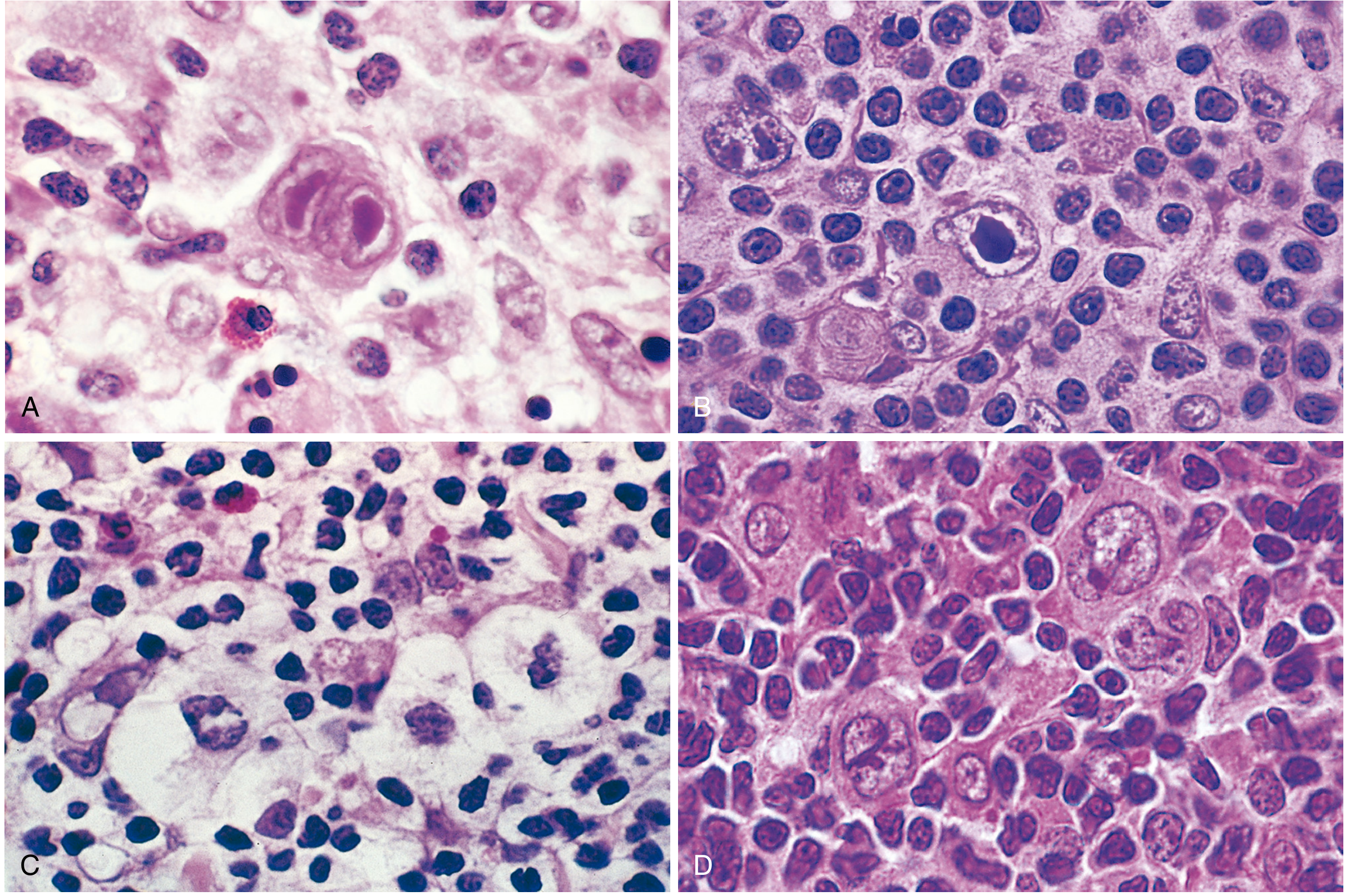
4. Reed-Sternberg Cell
| Feature | Detail |
|---|
| Origin | Neoplastic B-cell (germinal center origin proven by IGH gene rearrangements) |
| Appearance | Bi- or multinucleated giant cell with large, prominent inclusion-like "owl-eye" nucleoli with a clear halo |
| Background | Lymphocytes, eosinophils, plasma cells, macrophages |
| IHC | CD15+, CD30+ (classic); EBV+ in 30-70% |
A: Classic diagnostic RS cell - bilobed, owl-eye nucleoli. B: Mononuclear variant. C: Lacunar variant (nodular sclerosis). D: Lymphohistiocytic "popcorn" variant.
Where they occur:
- Hodgkin lymphoma (classic type: nodular sclerosis, mixed cellularity, lymphocyte-rich, lymphocyte-depleted)
- Infectious mononucleosis (EBV-infected B cells can mimic RS cells)
Special points:
- Diagnostic RS cell: bilobed/multinucleated, each lobe has a large inclusion-like nucleolus ("owl eye")
- Lacunar variant: folded multilobated nucleus, sits in an open space (artifact of formalin) - seen in nodular sclerosis
- L&H "popcorn" cell: multiple infolded nuclear membranes, small nucleoli - seen in nodular lymphocyte predominant HL; CD20+, CD15-, CD30-
- RS cells are necessary but not sufficient to diagnose HL (must be in appropriate cellular background)
- CD30 is the therapeutic target (brentuximab vedotin)
Clinical significance: Hallmark of Hodgkin lymphoma; determines subtype; CD30 targeted by brentuximab
5. Osteoclast-type Giant Cell
| Feature | Detail |
|---|
| Origin | Fusion of monocyte/macrophage lineage (RANKL-driven osteoclast differentiation) |
| Nucleus arrangement | Numerous nuclei (can be 100+) distributed throughout large cytoplasm |
| Location | Typically in or near bone, in fibrovascular stroma |
Where they occur:
- Giant cell tumor of bone (GCT) - epiphyses of long bones, 3rd-5th decade
- Aneurysmal bone cyst
- Giant cell reparative granuloma (jaw bones)
- Brown tumor of hyperparathyroidism
- Clear-cell chondrosarcoma (mixed)
- Tenosynovial giant cell tumor (PVNS)
- Paget disease (osteoclastic activity)
Special points:
- In GCT: monotonous mononuclear stromal cells + macrophages + osteoclast-type giant cells
- GCT is benign but locally aggressive; ~1-2% can metastasize to lung
- RANKL pathway drives formation - denosumab (anti-RANKL) is treatment option for unresectable GCT
- Brown tumors of hyperparathyroidism are histologically indistinguishable from GCT - always check serum calcium and PTH
Clinical significance: GCT - lytic epiphyseal lesion on X-ray ("soap bubble" appearance); treatment is surgical + denosumab for unresectable cases
6. Warthin-Finkeldey Giant Cell
| Feature | Detail |
|---|
| Origin | Lymphoid/viral (EBV-like mechanism in measles) |
| Appearance | Large multinucleated syncytial giant cell with amphophilic cytoplasm; nuclei form bizarre clusters; "grape-like" nuclear inclusions |
Where they occur:
- Measles (rubeola) - lymph nodes, tonsils, appendix, respiratory mucosa
- Also in HIV lymphadenopathy
Special points:
- Pathognomonic for measles when seen in lymphoid tissue
- Appear during prodromal/early phase of measles
- Koplik spots (on buccal mucosa) correspond to same virus - Warthin-Finkeldey cells are the histologic counterpart
Clinical significance: Seen in lymph node biopsy done for unexplained lymphadenopathy - should prompt measles serology
7. Tumor Giant Cells (Anaplastic)
| Feature | Detail |
|---|
| Origin | Neoplastic cells |
| Appearance | Hyperchromatic, pleomorphic, irregularly shaped nuclei scattered throughout cytoplasm; atypical mitoses common |
Where they occur:
- Giant cell carcinoma (e.g., lung, thyroid, pancreas)
- Pleomorphic undifferentiated sarcoma
- Anaplastic large cell lymphoma
- Osteosarcoma
Special points:
- Not a result of macrophage fusion - these are malignant cells
- Indicate high-grade malignancy with worse prognosis
8. Syncytiotrophoblast / Placental Giant Cell
- Multinucleated syncytial cells lining chorionic villi
- Physiologic, not pathological
- Can be confused with tumor giant cells if seen in ectopic locations (choriocarcinoma)
Summary Table
| Giant Cell | Nuclear Pattern | Origin | Hallmark Disease | Key Marker |
|---|
| Langhans | Horseshoe / peripheral | Macrophage fusion | TB, Sarcoidosis, Leprosy | Caseating/non-caseating granuloma |
| Foreign Body | Randomly scattered | Macrophage fusion | Suture/implant reactions | Polarized foreign material |
| Touton | Wreath ring + peripheral foam | Lipid macrophage fusion | Juvenile xanthogranuloma | "Wreath" nuclei + foamy rim |
| Reed-Sternberg | Owl-eye bilobed, prominent nucleoli | Neoplastic B-cell | Hodgkin lymphoma | CD15+, CD30+ |
| Osteoclastic | Numerous, scattered (100+) | Monocyte/macrophage | Giant cell tumor of bone | RANKL pathway |
| Warthin-Finkeldey | Grape-like clusters | Lymphoid/viral | Measles (rubeola) | Pathognomonic for measles |
| Tumor/Anaplastic | Hyperchromatic, pleomorphic | Malignant cells | Anaplastic carcinomas | Atypical mitoses |
Key Clinical Pearls
- Langhans ≠ Langerhans - Langhans = granuloma giant cell; Langerhans = dendritic cell of skin (Birbeck granules, CD1a+, S100+)
- None of the three main giant cells (Langhans, Foreign Body, Touton) are disease-specific - context and associated findings determine diagnosis
- Owl-eye nucleolus = Reed-Sternberg cell = Hodgkin lymphoma until proven otherwise
- Touton cells in the eye (juvenile xanthogranuloma) can cause spontaneous hyphema in infants
- Brown tumor and Giant Cell Tumor of bone are histologically identical - always check calcium/PTH to exclude hyperparathyroidism before labeling as GCT
- Denosumab (anti-RANKL monoclonal antibody) targets osteoclastic giant cells in GCT of bone
- Granulomatous inflammation requires special stains (ZN for TB, PAS/GMS for fungi, polarization for foreign material) before labeling as idiopathic
Sources: Dermatology 2-Volume Set 5e (Dermatology); Robbins, Cotran & Kumar Pathologic Basis of Disease; Dermatology 2-Volume Set 5e (granuloma classification); Reed-Sternberg cell data from Robbins.