Infective endocarditis
Reading File
Finding Sources
Searching PubMed
"infective endocarditis"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I have extensive material now. Let me compile the comprehensive answer.
Infective Endocarditis (IE)
Definition
Infective endocarditis is a microbial infection of the endocardial surface of the heart - primarily the cardiac valves - leading to the formation of vegetations composed of thrombotic debris, fibrin, inflammatory cells, and organisms, often with destruction of the underlying tissue. The aorta, aneurysmal sacs, other vessels, prosthetic devices, and cardiovascular implantable electronic devices (CIEDs) can also be affected. The vast majority of cases are bacterial.
- Robbins & Kumar Basic Pathology, p. 368
- Goldman-Cecil Medicine, p. 700
Classification
| Type | Tempo | Organism | Valve |
|---|---|---|---|
| Acute | Days; fulminant, destructive | S. aureus (virulent) | Can attack normal valves |
| Subacute | Weeks to months; insidious | Viridans streptococci (less virulent) | Usually pre-damaged valves |
Note: the acute/subacute distinction is not always clear-cut; many cases fall on a spectrum.
Epidemiology
-
Incidence in Western countries: approximately 3-14 cases per 100,000 persons/year
-
The US sees roughly 10,000-20,000 new cases per year
-
Shifting epidemiology: in developed countries, S. aureus (driven by healthcare exposure and IV drug use) has surpassed viridans streptococci as the most common causative agent
-
In developing countries, rheumatic heart disease still predominates, with subacute disease caused by VGS in younger adults
-
The opioid epidemic has contributed to rising IE rates, especially in rural US settings
-
Braunwald's Heart Disease, p. 838
Predisposing Conditions / Risk Factors
More common:
- Mitral valve prolapse (especially with regurgitation) - the leading structural risk factor in developed countries
- Degenerative valvular disease
- Injection drug use (IV drug use - favors tricuspid involvement)
- Congenital heart disease (VSD, unrepaired cyanotic CHD)
- Previous IE
- Prosthetic heart valves (10-20% of all IE cases)
- Pacemaker/CIED lines and indwelling vascular catheters
Less common:
- Rheumatic heart disease (still important in developing countries)
- Bicuspid aortic valve
- Hypertrophic obstructive cardiomyopathy
- Hemodialysis access
Host factors: neutropenia, immunodeficiency, malignancy, diabetes, alcohol abuse.
- Robbins & Kumar, p. 368; Goldman-Cecil Medicine, p. 700
Pathogenesis
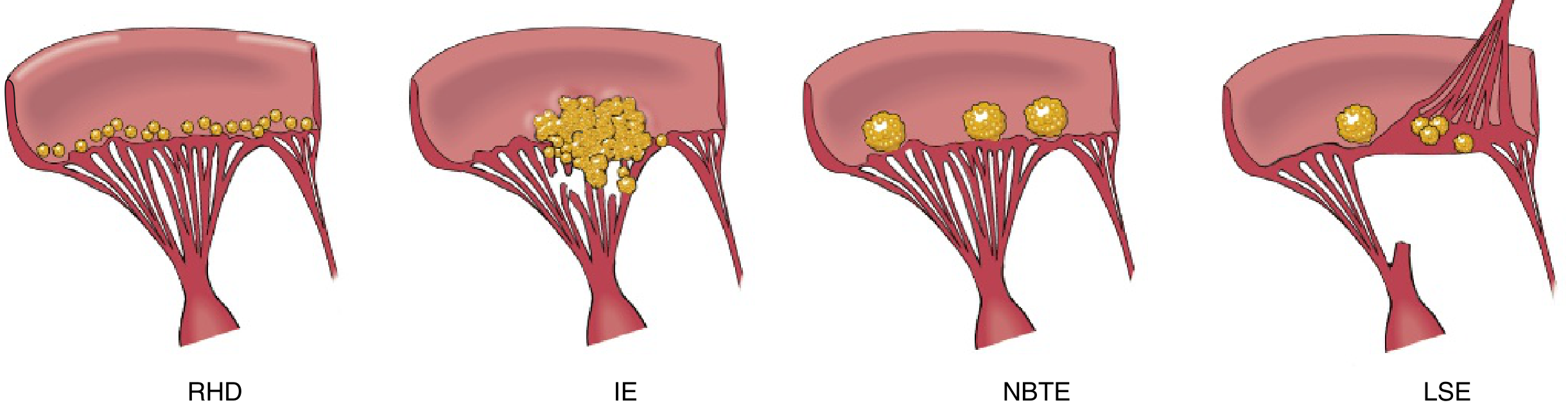
- Endothelial damage (from turbulent flow, jets, indwelling hardware) creates sterile platelet-fibrin deposits (non-bacterial thrombotic endocarditis - NBTE)
- Transient bacteremia seeds these deposits
- Organisms adhere, proliferate, and become embedded in a protective fibrin-platelet matrix forming vegetations
- Portal of entry: dental/surgical procedures, IV drug injection, gut/oral flora, infected catheters, trivial skin injuries
Key organisms:
- Staphylococci, streptococci, enterococci are the three most common worldwide
- S. viridans: 50-60% of community-acquired IE; damaged valves; subacute course
- S. aureus: most common in healthcare settings and IVDU; can infect normal valves; acute course
- HACEK group: Haemophilus, Aggregatibacter (Actinobacillus), Cardiobacterium, Eikenella, Kingella - oral commensals, slow-growing gram-negative bacilli
- Enterococci: genitourinary/GI portal of entry
- Culture-negative endocarditis (~10%): prior antibiotics, fastidious organisms (Coxiella burnetii/Q fever, Bartonella, Brucella, HACEK)
Morphology (Pathology)
Vegetations in IE are friable, bulky, and destructive, containing fibrin, inflammatory cells, and large numbers of microorganisms. Contrast with other endocardial lesions:
- Sites: Aortic and mitral valves most common (left-sided); tricuspid valve in IVDU (right-sided)
- Vegetations may be single or multiple, on one or more valves
- Can erode into myocardium producing ring abscesses (especially aortic valve IE - can disrupt the conduction system causing heart block)
- Friable nature leads to septic emboli → abscesses, septic infarcts, mycotic aneurysms at embolic sites
Clinical Features
Symptoms
- Fever (most consistent sign - >90% of patients)
- Chills, night sweats, malaise, fatigue, weight loss, myalgias, arthralgias
- Subacute: vague flu-like illness; splenomegaly common
- Acute: rapidly developing fever, rigors, sepsis
Signs - "FROM JANE" (mnemonic)
| Sign | Description | Mechanism |
|---|---|---|
| Fever | >38°C | Infection |
| Roth spots | Oval retinal hemorrhages with pale center | Immune complex vasculitis / emboli |
| Osler nodes | Painful, tender nodules on fingertips/toes | Immune complex deposition |
| Murmur | New/changing regurgitant murmur | Valve destruction (~90% of left-sided IE) |
| Janeway lesions | Painless erythematous macules on palm/sole | Septic emboli |
| Anemia | Normocytic anemia of chronic disease | Chronic inflammation |
| Nail-bed hemorrhages | Splinter (linear) hemorrhages | Microemboli |
| Emboli | Stroke, peripheral embolism, septic pulmonary infarcts | Vegetation fragments |
Key mnemonic: Osler nodes are Ouch (painful) - immune complex; Janeway lesions are Just there (painless) - septic emboli.
Diagnosis: Modified Duke Criteria
A definite diagnosis requires:
- Pathologic criteria (culture/histology from vegetation or abscess), OR
- Clinical criteria: 2 major, OR 1 major + 3 minor, OR 5 minor criteria
Possible IE: 1 major + 1 minor, OR 3 minor criteria
Major Criteria
-
Blood culture positive for IE
- Typical organisms (S. viridans, S. gallolyticus, S. aureus, HACEK, community-acquired enterococci) from ≥2 separate cultures
- Persistently positive cultures (≥2 from samples >12 hr apart, or ≥3 of ≥4 samples)
- Single positive culture for Coxiella burnetii OR anti-phase I IgG titer ≥1:800
-
Evidence of endocardial involvement (Echo/imaging)
- Oscillating intracardiac mass on valve or supporting structures
- Abscess / ring abscess
- New partial dehiscence of prosthetic valve
- New valvular regurgitation (worsening of pre-existing murmur NOT sufficient)
- 18F-FDG PET/CT: abnormal metabolic activity at valve/prosthetic material (≥3 months after implantation) - added in 2023 updated criteria
Minor Criteria
- Predisposing heart condition or IV drug use
- Fever >38°C
- Vascular phenomena: major arterial emboli, septic pulmonary infarcts, mycotic aneurysm, intracranial hemorrhage, conjunctival hemorrhages, Janeway lesions
- Immunologic phenomena: glomerulonephritis, Osler nodes, Roth spots, rheumatoid factor
- Microbiologic evidence: positive blood culture not meeting major criteria (excludes single coagulase-negative staphylococci)
- Braunwald's Heart Disease; Clinical Echocardiography (2023 Duke Criteria)
Investigations
| Investigation | Purpose/Findings |
|---|---|
| Blood cultures | 3 sets from different sites before antibiotics; most important test |
| CBC | Leukocytosis (acute), normocytic anemia, elevated ESR/CRP |
| Urinalysis | Hematuria, proteinuria (immune complex GN) |
| TTE (transthoracic echo) | First-line; sensitivity ~60-70% for vegetations |
| TEE (transesophageal echo) | Superior sensitivity (~90%); indicated when TTE negative but suspicion high, prosthetic valves, poor TTE window, complications suspected |
| 18F-FDG PET/CT | Useful for prosthetic valve endocarditis (PVE) when TEE non-diagnostic |
| CT/MRI brain | Detect embolic stroke, cerebral abscess, mycotic aneurysm |
Per AHA guidelines: TEE is especially urged when:
- TTE is of poor quality or negative despite high clinical suspicion
- Prosthetic valve is involved
- S. aureus bacteremia
- Complications (paravalvular abscess) suspected
Complications
| Complication | Notes |
|---|---|
| Heart failure | Most common indication for surgery; valve destruction, especially acute aortic IE |
| Perivalvular extension | Ring abscess, fistula formation; complicates aortic IE most often; causes heart block |
| Systemic emboli | Stroke (most feared), splenic/renal/mesenteric infarcts |
| Septic pulmonary emboli | Right-sided IE (IVDU) |
| Mycotic aneurysm | Bacterial infection of arterial wall; can rupture → catastrophic hemorrhage |
| Glomerulonephritis | Immune complex deposition; hematuria, renal failure |
| Metastatic abscess | Brain, spleen, kidney |
| Arrhythmias/heart block | Extension to conduction system (aortic root abscess) |
| Relapse | 2-20% of cases |
Management
Principles
- Every patient with IE should be managed inpatient at a center with an experienced multidisciplinary "IE team" (infectious disease, cardiology, cardiac surgery)
- Blood cultures must be drawn before antibiotics
- Prolonged parenteral antibiotics are the cornerstone
- Surgical consultation in all complicated cases
Antibiotic Therapy (General Principles)
Parenteral bactericidal antibiotics for 4-6 weeks; regimens tailored to organism and susceptibility:
| Organism | Preferred Regimen |
|---|---|
| Penicillin-sensitive S. viridans / S. gallolyticus | Penicillin G or ceftriaxone × 4 weeks; or + gentamicin × 2 weeks (shortened course) |
| Penicillin-resistant streptococci | Penicillin G + gentamicin × 4 weeks, or vancomycin × 4 weeks |
| MSSA S. aureus | Nafcillin/oxacillin × 6 weeks (native valve); ± gentamicin first 3-5 days |
| MRSA S. aureus | Vancomycin × 6 weeks |
| Enterococcus | Ampicillin + gentamicin × 4-6 weeks, OR ampicillin + ceftriaxone (for high-level aminoglycoside resistance) |
| HACEK organisms | Ceftriaxone × 4 weeks |
| Prosthetic valve MRSA | Vancomycin + rifampin × ≥6 weeks + gentamicin × 2 weeks |
Indications for Surgery
Surgery (valve repair or replacement) is indicated urgently/emergently for:
- Heart failure or cardiogenic shock due to valvular dysfunction - most common surgical indication (Class I)
- Locally uncontrolled infection - paravalvular abscess, fistula, enlarging vegetation despite appropriate antibiotics, persistent bacteremia
- Prevention of embolism - large vegetation (>10 mm) especially with prior embolic event, or very large (>15 mm) vegetation
- Prosthetic valve endocarditis - especially early PVE (<1 year after implantation), PVE with dehiscence, or S. aureus PVE
- Fungal IE - almost always requires surgery
The AHA, ACC/AHA, and ESC guidelines all support early surgery for life-threatening heart failure in active IE.
Antibiotic Prophylaxis (2021 AHA Update)
The 2021 AHA Scientific Statement narrowed prophylaxis indications to high-risk cardiac conditions only:
-
Indications (AP suggested):
- Prosthetic cardiac valve or prosthetic material used for valve repair
- Transcatheter-implanted prosthetic valves
- Previous IE
- Unrepaired cyanotic CHD (including palliative shunts/conduits)
- Repaired CHD with prosthetic material within the first 6 months post-procedure, or with residual defect
- Cardiac transplant recipients with valvulopathy
- New: Ventricular assist devices and implantable hearts
- New: Melody valve and Contegra conduit
-
Prophylaxis NOT suggested: Pacemakers/ICDs, septal defect closure (with complete closure), coronary stents, peripheral vascular grafts, vena cava filters
-
Preferred agent: Amoxicillin 2 g PO 30-60 min before dental procedure (90% of "penicillin-allergic" patients will have negative skin testing and can use amoxicillin)
-
Clindamycin removed as an alternative (risk of C. difficile)
-
Doxycycline added as an alternative for truly penicillin-allergic patients
Prognosis
- Left untreated, IE is universally fatal
- With appropriate therapy, overall in-hospital mortality: 15-25%
- Worse prognosis: S. aureus, prosthetic valve IE, aortic IE, perivalvular extension, heart failure, large vegetations, elderly, immunocompromised
- Better prognosis: streptococcal IE, early surgery when indicated
Special Populations
Right-sided IE (IVDU):
- Tricuspid valve most common
- S. aureus predominates
- Septic pulmonary emboli (presenting as multiple nodular opacities/cavities on CXR/CT)
- Better prognosis than left-sided IE; some cases can be treated with shorter (2-4 week) antibiotic courses
Prosthetic Valve IE (PVE):
- Early PVE (<60 days post-op): coagulase-negative staphylococci, S. aureus, gram-negatives, fungi
- Late PVE (>12 months): similar to native valve IE
- Higher morbidity/mortality; surgery often required
- TEE and PET/CT are especially valuable
Culture-negative IE: workup for fastidious organisms - Coxiella burnetii (Q fever; most common cause of culture-negative IE in some series), Bartonella, Tropheryma whipplei, Brucella
Key Sources:
- Braunwald's Heart Disease, 12th Ed. - Chapters 80, 80G
- Robbins & Kumar Basic Pathology - Chapter 9, p. 368
- Goldman-Cecil Medicine - Chapter 61, p. 700
- Textbook of Clinical Echocardiography (2023 Duke Criteria), Chapter 14
- Tintinalli's Emergency Medicine, Chapter 129
This is a shared conversation. Sign in to Orris to start your own chat.