Treatment for migraine
Reading File
Finding Sources
Searching PubMed
"migraine"[MeSH Terms] AND "treatment"[MeSH Terms]
Reading File
Reading File
Reading File
Searching PubMed
"migraine" AND "gepant OR triptan OR CGRP"
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive information to provide a thorough answer. Here is a complete, well-structured overview of migraine treatment:
Migraine Treatment
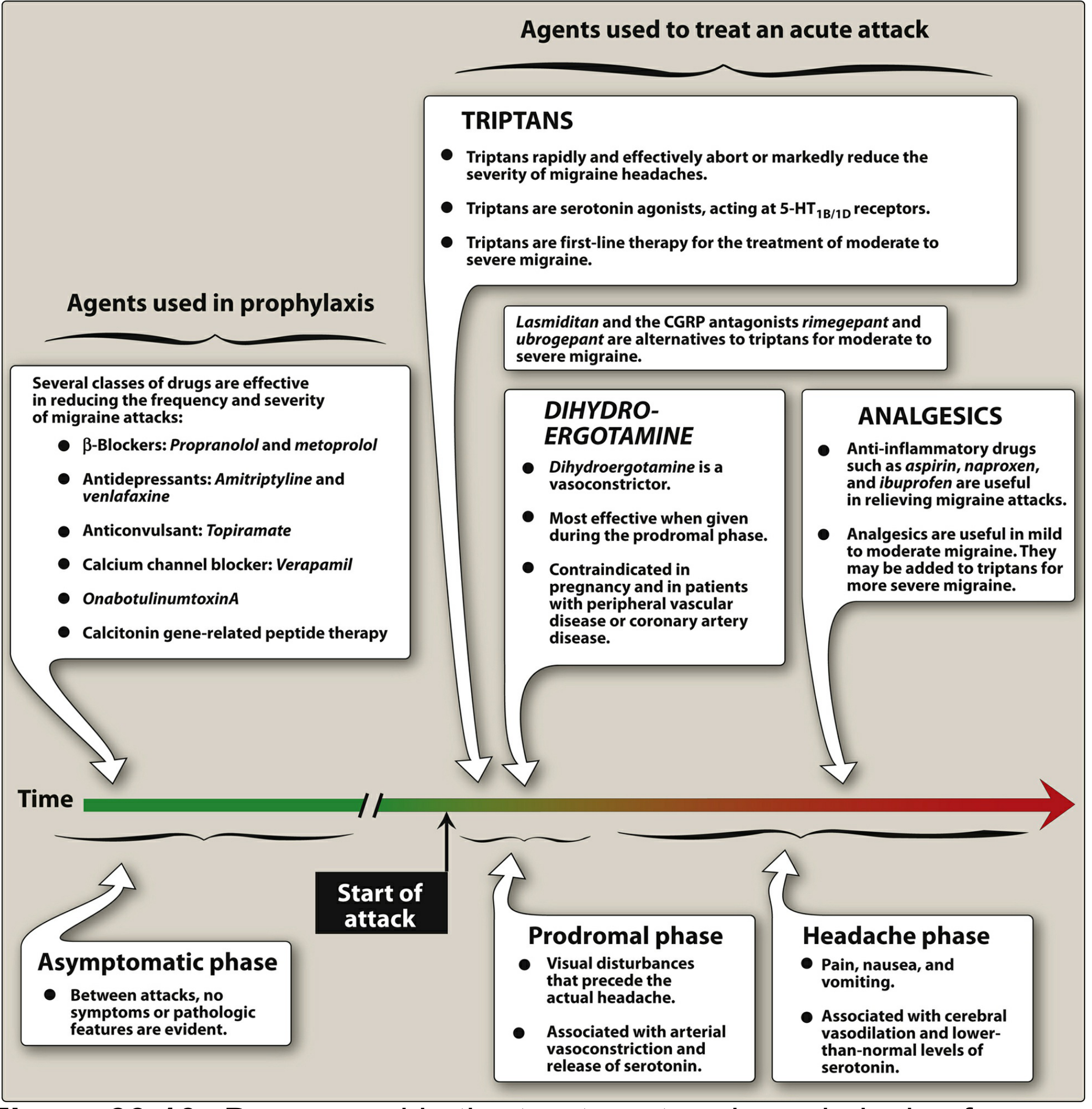
Figure: Treatment and prophylaxis of migraine across attack phases. — Lippincott Illustrated Reviews: Pharmacology
Overview
Migraine management divides into two strategies:
- Acute (abortive) — stopping an attack in progress
- Preventive (prophylactic) — reducing frequency/severity
Treatment should be started as early as possible — ideally during the visual prodrome or at headache onset.
A. Acute Treatment
Step 1 — Mild to Moderate Attacks
NSAIDs / Analgesics are first-line for mild attacks:
- Aspirin, ibuprofen, naproxen, or acetaminophen
- Ketorolac 10–30 mg IV/IM is used in the ED setting
- Caution: overuse (>10–15 days/month) can trigger medication-overuse headache
Antiemetics address nausea/vomiting and have independent analgesic effects:
| Drug | Dose | Notes |
|---|---|---|
| Prochlorperazine | 5–10 mg IV/PR | Give diphenhydramine concurrently to prevent dystonia |
| Metoclopramide | 10 mg IV | Also prokinetic; give diphenhydramine |
| Droperidol | 2.5 mg IV/IM | Monitor QTc |
| Chlorpromazine | 7.5 mg IV | Pretreat with NS bolus for hypotension |
Step 2 — Moderate to Severe Attacks: Triptans (First-Line)
Triptans are 5-HT₁B/1D receptor agonists — they cause cranial vasoconstriction and inhibit release of proinflammatory neuropeptides from trigeminal nerve endings. Effective in ~70% of patients.
Available triptans and oral dosing:
| Drug | Optimum dose | Max daily dose |
|---|---|---|
| Sumatriptan | 50 mg PO / 6 mg SC / 20 mg nasal | 200 mg |
| Rizatriptan | 10 mg | 30 mg |
| Zolmitriptan | 2.5 mg PO or nasal | 10 mg |
| Eletriptan | 20–40 mg | 80 mg |
| Almotriptan | 12.5 mg | 25 mg |
| Naratriptan | 2.5 mg | 5 mg |
| Frovatriptan | 2.5 mg (longest t½ >24 h) | 7.5 mg |
Route matters: Subcutaneous onset ~20 min; oral onset ~1–2 hours. Use SC or nasal formulations when nausea limits oral intake, or when oral preparations have been ineffective if given late.
Contraindications: Ischemic heart disease, uncontrolled hypertension, history of stroke/TIA, hemiplegic or basilar migraine, peripheral vascular disease.
Step 3 — Alternatives When Triptans Are Contraindicated or Ineffective
CGRP Receptor Antagonists ("Gepants") — Acute Use
- Ubrogepant and rimegepant — oral CGRP antagonists; no vasoconstriction, so safe in patients with cardiovascular contraindications to triptans
- Rimegepant also has a dual acute + preventive role (see below)
Ditans
- Lasmiditan — selective 5-HT₁F receptor agonist; no vasoconstriction; approved for acute migraine but causes CNS sedation/dizziness
Ergot Alkaloids
- Ergotamine (sublingual/oral + caffeine): potent alpha-adrenergic + 5-HT₁ agonist with vasoconstricting action. Effective if used early; strict dosage limits due to dependence and rebound headache risk.
- Dihydroergotamine (DHE) 1 mg IV (over 3 min) or 1 mg intranasal: reserved for severe/refractory migraine. Pretreat with an antiemetic. Contraindicated in pregnancy (Category X), CAD, uncontrolled hypertension, basilar/hemiplegic migraine. Do not combine with triptans within 24 hours.
IV/Hospital Options
- Magnesium sulfate 2 g IV over 30 min — especially useful in migraine with aura; consider in pregnancy
- Valproate 500 mg IV — nonvalidated but used
- Dexamethasone 6–10 mg IV — adjunctive, reduces recurrence
- Ketamine 0.1–0.3 mg/kg IV — refractory cases; safe with head trauma (does not raise ICP)
B. Preventive (Prophylactic) Treatment
Indications: ≥2 attacks/month, severe or prolonged attacks, attacks with serious neurologic signs, poor response to acute treatment, or medication overuse.
First-Line Preventives
| Class | Drugs | Notes |
|---|---|---|
| β-Blockers (drugs of choice) | Propranolol, metoprolol | Avoid in asthma, bradycardia, depression |
| Anticonvulsants | Topiramate, valproate (divalproex) | Topiramate: weight loss side effect; valproate: teratogenic |
| TCAs | Amitriptyline | Also treats comorbid depression/insomnia |
| SNRIs | Venlafaxine | Second-line antidepressant option |
| Calcium channel blockers | Verapamil | Also used for cluster headache prevention |
OnabotulinumtoxinA (Botox)
Approved for chronic migraine (≥15 headache days/month). Injected into 31 sites across head/neck every 12 weeks.
CGRP-Targeted Preventive Therapies (Newer)
Monoclonal antibodies (anti-CGRP or anti-CGRP receptor) — monthly or quarterly injections:
| Drug | Target | Dosing |
|---|---|---|
| Erenumab | CGRP receptor | 70–140 mg SC monthly |
| Galcanezumab | CGRP ligand | 120 mg SC monthly |
| Fremanezumab | CGRP ligand | 225 mg SC monthly or 675 mg quarterly |
| Eptinezumab | CGRP ligand | 100–300 mg IV quarterly |
Oral CGRP antagonists with dual acute + preventive use:
- Atogepant (daily oral) — preventive
- Rimegepant (as-needed or every-other-day oral) — both acute and preventive
These represent a major advance, particularly for patients who have failed or cannot tolerate traditional preventives.
C. Non-Pharmacological Measures
- Identify and avoid triggers (sleep disruption, skipped meals, alcohol, stress, hormonal fluctuations)
- Regular sleep schedule, hydration, stress management
- Biofeedback, cognitive-behavioral therapy, acupuncture — evidence-supported adjuncts
- Lifestyle modification should accompany any pharmacological regimen
Recent Evidence Update
A 2024 network meta-analysis (BMJ, PMID 39293828) compared drug interventions for acute migraine across 53 trials and found gepants and lasmiditan are effective alternatives to triptans with better cardiovascular safety profiles.
A 2025 evidence-based guideline (Cephalalgia, PMID 40277319) — the most current available — provides updated pharmacological treatment recommendations including CGRP therapies as both first- and second-line options depending on clinical context.
Sources: Adams and Victor's Principles of Neurology 12th Ed.; Lippincott Illustrated Reviews: Pharmacology; Tintinalli's Emergency Medicine; Goodman & Gilman's Pharmacological Basis of Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.