Describe Arterial supply of Heart. Summarize Autopsy diagnosis of Myocardial Infarction.
Arterial Supply of the Heart
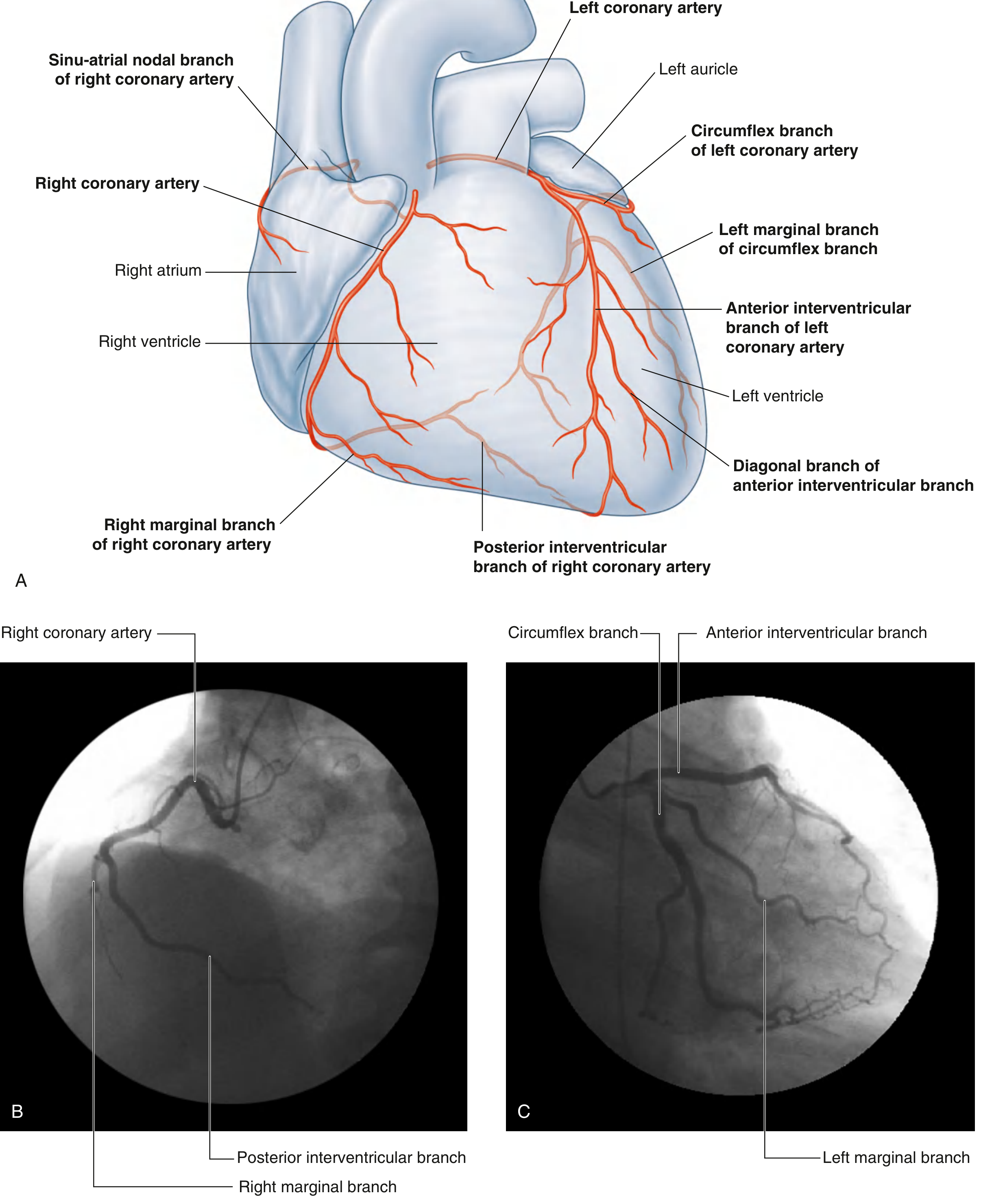
Right Coronary Artery (RCA)
| Branch | Course & Supply |
|---|---|
| Sinu-atrial nodal branch | Arises from an early atrial branch, passes around the superior vena cava to supply the SA node |
| Right marginal branch | Runs along the inferior (acute) margin toward the apex |
| AV nodal branch | Small branch to the atrioventricular node |
| Posterior interventricular branch (PDA) | Terminal branch in the posterior interventricular sulcus |
- Right atrium and right ventricle
- SA node and AV node (in most people)
- Interatrial septum
- Posteroinferior one-third of the interventricular septum
- Posterior part of the left ventricle (in right dominant hearts)
Left Coronary Artery (LCA)
1. Anterior Interventricular Branch (Left Anterior Descending - LAD)
2. Circumflex Branch (LCX)
- Most of the left atrium and left ventricle
- Most of the interventricular septum (anterior two-thirds)
- AV bundle and its branches
- Lateral wall of the left ventricle (LCX)
Coronary Dominance
In clinical practice: the short LCA is called the left main stem; the anterior interventricular artery is the LAD; the posterior interventricular artery is the posterior descending artery (PDA).
Autopsy Diagnosis of Myocardial Infarction
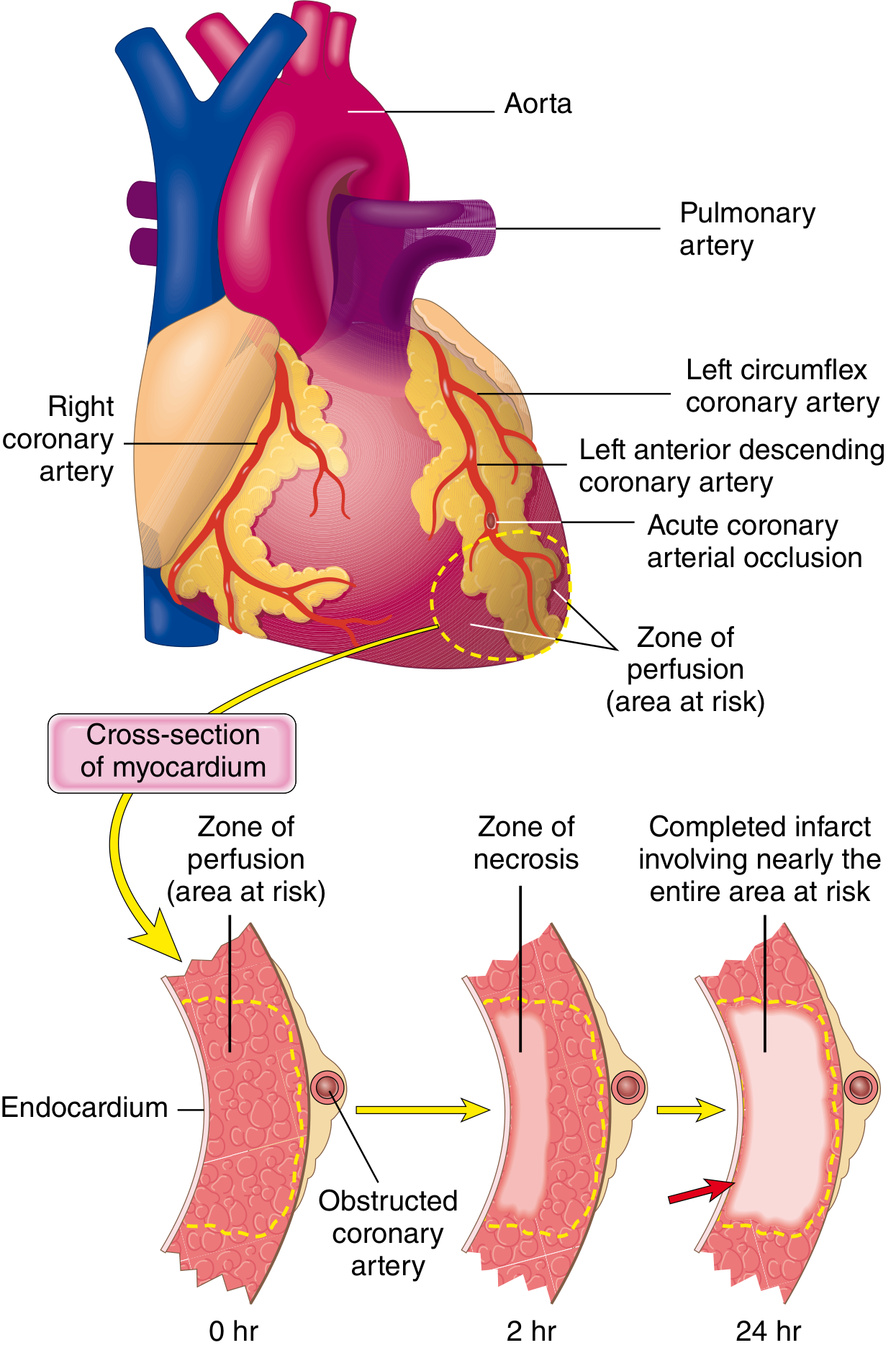
Patterns of Infarction at Autopsy

| Artery Occluded | Frequency | Infarct Location |
|---|---|---|
| LAD | 40-50% | Anterior LV wall near apex; anterior two-thirds of ventricular septum; apex circumferentially |
| RCA | 30-40% | Inferior/posterior LV wall; posterior ventricular septum; posterior RV free wall (some cases) |
| LCX | 15-20% | Lateral LV wall (except apex) |
- Transmural infarct: Full wall thickness necrosis. Caused by permanent occlusion of an epicardial vessel (atherosclerosis + thrombus). A thin rim (~0.1 mm) of subendocardial myocardium is spared by diffusion from the ventricular lumen.
- Subendocardial (nontransmural) infarct: Involves inner layers only. Occurs when a thrombus lyses before necrosis extends transmurally, or due to global hypoperfusion (shock) - in which case damage is circumferential, not limited to one vessel territory.
- Multifocal microinfarction: From small intramural vessel pathology (microembolism, vasculitis, cocaine-induced vasospasm).
Temporal Evolution of Morphologic Changes (Table 12.5)
| Time | Gross Appearance | Light Microscopy | Electron Microscopy |
|---|---|---|---|
| 0-0.5 hr | None | None | Myofibrillar relaxation; glycogen loss; mitochondrial swelling |
| 0.5-4 hr | None | Usually none; variable waviness of fibers at border | Sarcolemmal disruption; mitochondrial amorphous densities |
| 4-12 hr | Dark mottling (occasional) | Early coagulative necrosis; edema; hemorrhage | - |
| 12-24 hr | Dark mottling | Ongoing coagulative necrosis; nuclear pyknosis; myocyte hypereosinophilia; marginal contraction band necrosis; early neutrophilic infiltrate | - |
| 1-3 days | Mottling with yellow-tan infarct center | Coagulative necrosis with loss of nuclei and striations; brisk neutrophilic infiltrate | - |
| 3-7 days | Hyperemic border; central yellow-tan softening | Disintegrating dead myofibers; dying neutrophils; early macrophage phagocytosis at borders; early granulation tissue | - |
| 7-10 days | Maximally yellow-tan and soft, with depressed red-tan margins | Well-developed phagocytosis; granulation tissue at margins | - |
| 10-14 days | Red-gray depressed infarct borders | Established granulation tissue with new vessels and collagen deposition | - |
| 2-8 weeks | Gray-white scar, advancing from border toward core | Increased collagen; decreased cellularity | - |
| >2 months | Dense gray-white scar | Dense collagenous scar | - |
Key Autopsy Techniques
Coronary Pathology to Document
- Evidence of atherosclerotic plaque disruption/erosion
- Superimposed thrombus (present in ~90% of cases when angiography done within 4 hrs of onset)
- Degree of luminal stenosis
- Presence of collateral vessels
Search for recent research on collateral vessel development in chronic CAD0 marks answer for md Fmt paper
"coronary collateral" AND "chronic coronary" AND "arteriogenesis"
"collateral circulation"[MeSH Terms] AND "coronary artery disease"[MeSH Terms]
PMID: 41144984
"coronary collateral"[MeSH Terms] AND "angiogenesis"
"collateral vessels" AND "coronary artery disease" AND "prognosis"
PMID: 36072863
"arteriogenesis"[MeSH Terms] AND "coronary artery disease"[MeSH Terms]
"coronary collateral flow" AND "VEGF" OR "growth factor" AND "chronic ischemia"
PMID: 41144984
"coronary collateral" AND "development" AND "chronic total occlusion"
PMID: 38674237
PMID: 37417706
PMID: 41892713
Collateral Vessel Development in Chronic Coronary Artery Disease: Recent Research Summary
Background
1. Functional Role of Collaterals in Stable CAD
- Collateral flow index (CFI) correlated strongly with ischemic burden: lower FFR/iFR was associated with greater collateral recruitment (Somers' D 0.302, Pr = 0.999)
- Higher CFI was independently associated with lower pain intensity during balloon occlusion (Somers' D = 0.341, Pr = 0.999)
- Daily angina frequency showed little correlation with FFR or iFR alone - collateralization may explain the known nonlinear relationship between stenosis severity and symptom burden
- No evidence of ischemic preconditioning between sequential occlusion episodes
Clinical implication: Collateral adequacy - not stenosis severity alone - determines symptom burden in chronic stable CAD, and should be factored into revascularization decisions.
2. MicroRNA Mediators of Collateral Development (Mechanobiology)
- Patients with favorable collaterals had significantly higher CFI (0.45 ± 0.02 vs 0.38 ± 0.03, p < 0.001)
- miR-26a and miR-21 showed strong positive correlations with CFI (r = 0.715 and r = 0.663, respectively)
- let-7d and miR-663 were negatively correlated with CFI (r = -0.684 and r = -0.604)
- Significant correlations found between:
- TGF-β and miR-126 (r = 0.673)
- VEGF and miR-10a (r = 0.602)
- Multivariate regression identified hemoglobin, smoking, beta-blocker use, miR-26a, and miR-663 as independent determinants of CFI
Mechanistic insight: Shear stress-responsive miRNAs modulate the VEGF and TGF-β signaling axes that drive arteriogenesis and angiogenesis in CTO. These represent potential therapeutic targets and non-invasive biomarkers.
3. Endothelial Dysfunction as a Predictor of Poor Collateral Formation
- Poorly developed CCC (Rentrop grades 0-1) was present in 37.6% of patients
- Well-developed CCC group had significantly lower EASIX (median 0.44 vs 0.67, p < 0.001) and higher HDL cholesterol
- EASIX independently predicted poor collateral development: OR 2.536 per 1-SD increase (95% CI 1.734-3.710, p < 0.001)
- ROC analysis: AUC = 0.718, sensitivity 72.9%, specificity 62.1% at cutoff > 0.51
- Neutrophil-to-lymphocyte ratio was also elevated in the poor-collateral group
Clinical implication: Systemic endothelial stress - measurable via a simple, low-cost index - is a significant determinant of collateral vessel adequacy. EASIX may help risk-stratify CTO patients before revascularization planning.
4. Diabetes, Dyslipidemia, and Impaired Collateral Formation
- Patients with diabetic microvascular complications (DMC - neuropathy, nephropathy, retinopathy) had higher prevalence of collaterals (92.0% vs 75.6%, p = 0.006) and higher-grade collaterals (73.3% vs 47.6%, p = 0.001)
- A positive association was found between the number of DMC and prevalence of high-grade CCC
This challenges the assumption that diabetes uniformly impairs collaterals; chronic ischemic stimulus from microvascular disease may itself promote collateral arteriogenesis in some T2DM patients.
- Mechanisms: Altered lipid profiles cause glycoxidative modification of LDL, endothelial dysfunction, and blunting of endothelial progenitor cell (EPC) responses
- Elevated triglycerides, hypercholesterolemia, raised Lp(a), and HDL quality/quantity defects all independently impair collateral growth and maturation
- Lipid-lowering therapies (statins, PCSK9 inhibitors) may partially restore collateral capacity via anti-inflammatory and EPC-stimulating effects
5. Summary of Key Mechanisms and Biomarkers
| Factor | Effect on Collateral Development | Evidence |
|---|---|---|
| Shear stress / mechano-miRs (miR-26a, miR-21) | Promote arteriogenesis via VEGF/TGF-β signaling | PMID 38674237 |
| Endothelial dysfunction (high EASIX) | Impairs collateral formation | PMID 41892713 |
| Diabetic dyslipidemia (high LDL, low HDL, high Lp(a)) | Impairs EPC response and collateral maturation | PMID 36072863 |
| Diabetic microvascular complications | Paradoxically associated with better collaterals (chronic ischemia stimulus) | PMID 37417706 |
| Collateral adequacy (CFI) | Reduces ischemic pain; explains angina-stenosis disconnect | PMID 41144984 |
| High HALP score / prognostic nutritional index | Positive associations with better CCC grades in CTO | PMID 41937261, 35068879 |
Gaps and Future Directions
- Most CTO-collateral studies rely on angiographic Rentrop grading, which has limited resolution compared to pressure-wire CFI measurements
- The paradox of DMC and enhanced collateral formation needs prospective validation
- mechano-miR profiling (miR-26a, miR-21) and EASIX require multicenter prospective validation before clinical adoption
- Therapeutic strategies (gene therapy with VEGF, cell-based EPC therapy) have not yet shown consistent benefit in RCTs; the mRNA-VEGF delivery approach in porcine chronic ischemia models showed no therapeutic effect, highlighting translation challenges (PMID 34494459)