From the basic of complete cardio vascular and other important topic before Ecg, Then complete master class of Ecg,TMT,haltter and Echo.
What's Included - Master Class Structure
PART 1: Cardiovascular Basics (Pre-ECG Foundation)
- 1.1 Cardiac Anatomy - Chambers, layers, valves, coronary circulation with vessel territories
- 1.2 Microanatomy & E-C Coupling - Cardiomyocyte structure, sarcomere, calcium cycling, SERCA, Frank-Starling law (from Braunwald's Heart Disease)
- 1.3 Action Potential & Conduction System - 5 phases, pacemaker AP, SA→AV→His→Bundle→Purkinje pathway with speeds
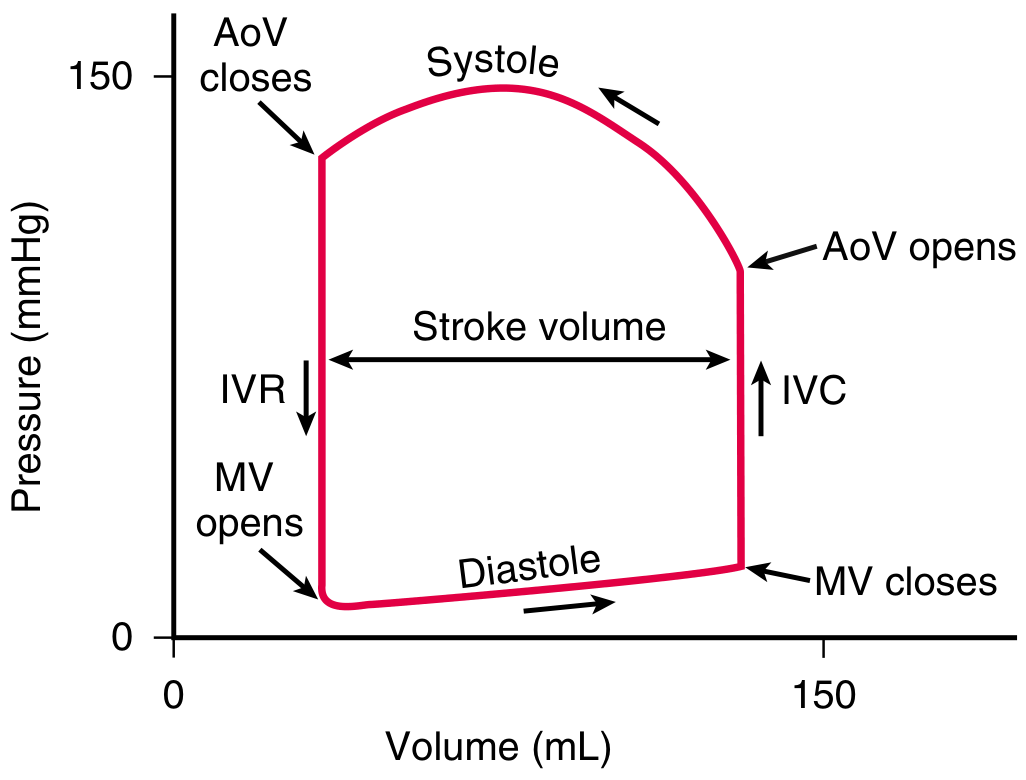
- 1.4 The Cardiac Cycle - All phases of systole and diastole, pressure values, heart sounds, key formulas (CO, EF, preload, afterload)
- 1.5 Autonomic Control - Sympathetic (chronotropy, inotropy, dromotropy) and parasympathetic effects
- 1.6 Pre-ECG Electrophysiology - Ion channel table, refractory periods, QT and Bazett's formula
PART 2: ECG Master Class
- 2.1-2.2 ECG basics, paper speed, the 12 leads, anatomical groupings
- 2.3 All waveforms (P, PR, QRS, ST, T, QT, U) with normal values
- 2.4 Systematic 8-step ECG interpretation method
- 2.5 Axis determination (quick I + aVF method + causes)
- 2.6 RBBB, LBBB, Sgarbossa criteria, fascicular blocks
- 2.7 Chamber enlargement (LAE, RAE, LVH with Sokolow + Cornell, RVH)
- 2.8 Ischemia cascade, STEMI evolution and localization by territory, De Winter T waves, NSTEMI
- 2.9 Full arrhythmia section - AF, flutter, AVNRT, WPW, all AV blocks, VT, VF, Torsades
- 2.10 Electrolyte changes (hyperkalemia stages, hypokalemia, Ca)
- 2.11 Brugada, pericarditis (4 stages), PE (S1Q3T3), digoxin effect, hypothermia Osborn waves
PART 3: TMT / Exercise Stress Test
- Indications, absolute and relative contraindications
- Bruce Protocol table with METs, modified protocol
- Target HR calculation, test conduct, monitoring
- Stopping criteria (absolute and relative)
- Positive criteria for ischemia, high-risk features
- Duke Treadmill Score formula + risk categories
- BP response, false positives, false negatives, sensitivity/specificity
PART 4: Holter Monitoring
- Types of ambulatory monitoring (24h Holter → ILR 3 years)
- All indications including cryptogenic stroke AF detection
- Interpretation parameters (PVC burden, pauses, HRV, AF burden)
- ILR and the CRYSTAL-AF trial data
PART 5: Echocardiography
- Ultrasound physics, Doppler types (PW, CW, Color, TDI) with uses
- Standard echo views (PLAX, PSAX, A4C, A2C, subcostal, suprasternal)
- LV systolic function (EF, Simpson's, wall motion 17-segment model)
- Diastolic function (E/A, e', E/e', ASE 2016 grading table)
- Valve quantification: AS (continuity equation, severity table), MS (PHT method, Wilkins score), AR, MR (PISA method) - all from Textbook of Clinical Echocardiography
- PA pressure estimation (TR jet + RAP)
- RV assessment (TAPSE, FAC, S')
- IVC and volume status
- Pericardial effusion and tamponade echo signs
- Stress echo / dobutamine echo (viability "biphasic response")
- TEE indications
More detailed analysis and information with case studies all the normal and abnormalities.
What's New in This Expanded Edition
Section A - Cardiovascular Physiology Deep Dive
- Pressure-Volume Loop traced point-by-point through all phases of the cardiac cycle, with how disease (HF, hypertension, volume overload, inotropes) shifts the loop
- LV Geometry patterns: concentric remodeling, concentric hypertrophy, eccentric hypertrophy (with RWT formula)
- Global Longitudinal Strain (GLS): -20% normal, detection of subclinical dysfunction before EF drops
Section B - ECG: 20 Case Studies
- Case 1: Normal sinus rhythm (step-by-step reference)
- Cases 2-4: Sinus bradycardia, sinus tachycardia (cause analysis), sick sinus syndrome
- Cases 5-6: LAE (P-mitrale mechanism), RAE (P-pulmonale)
- Cases 7-8: LVH with strain (Sokolow + Cornell criteria), pathological vs normal Q waves
- ST Elevation Differential Table (10 causes with distinguishing features)
- Cases 9-11: Inferior STEMI with RV infarct (NTG contraindication), Anterior STEMI, De Winter T waves (must-not-miss STEMI equivalent)
- Case 12: Posterior STEMI (looks like NSTEMI in V1-V2; confirmed by V7-V9)
- Cases 13-16: AF (CHA2DS2-VASc scoring, anticoagulation rules), atrial flutter (vagal maneuver distinguishes from SVT), AVNRT mechanism + treatment, WPW (DANGEROUS drugs to avoid, management)
- Cases 17-19: VT vs SVT-aberrancy (full Brugada algorithm), Torsades de Pointes (drugs that cause it, magnesium treatment), Complete AV block (management of wide vs narrow escape)
- Case 20: Hyperkalemia progressive ECG changes (K+ 5.5 → K+ >8) with emergency treatment sequence
Section C - TMT: 4 Cases
- Case 21: Completely normal TMT (reference interpretation, Duke score +12)
- Case 22: Positive TMT with false positive discussion (women's rate)
- Case 23: HIGH-RISK TMT (Stage 1 positivity, exertional hypotension, Duke score -18 → urgent cath)
- Case 24: Non-diagnostic TMT (beta-blocker effect, what to do next)
Section D - Holter: 5 Cases
- Case 25: Normal 24-hour Holter (full quantitative report with HRV values)
- Case 26: PVC-induced cardiomyopathy (24% burden, RVOT origin, reversible with ablation)
- Case 27: Cryptogenic stroke → AF on Holter (CRYSTAL-AF trial data, ILR)
- Case 28: Sick sinus syndrome (5.8-second pause causing syncope documented in real-time)
- Case 29: Post-MI risk stratification (low HRV + NSVT + EF 35% → ICD indication)
Section E - Echo: 10 Cases
- Case 30: Normal quantitative echo (all numbers - reference standard)
- Case 31: Dilated cardiomyopathy - DCM (EF 21%, restrictive filling, functional MR, LV thrombus risk, GLS)
- Case 32: HOCM (asymmetric septal hypertrophy, SAM, LVOT gradient 65 mmHg, risk stratification, mavacamten)
- Case 33: Severe AS (continuity equation worked through, paradoxical low-flow AS explained, TAVR planning)
- Case 34: Severe mitral stenosis (Wilkins score, BMC candidacy, TEE for LAA thrombus)
- Case 35: Cardiac tamponade (RA collapse, RV collapse, IVC plethora, Doppler pulsus paradoxus)
- Case 36: LV apical thrombus post-STEMI (echo diagnosis, contrast use, anticoagulation)
- Case 37: Infective endocarditis with aortic root abscess (TTE vs TEE sensitivity, surgical indications)
- Cardiomyopathy comparison table: DCM vs HCM vs RCM vs ARVC
Section F - 3 Integrated Cases
- Case F.1: Diabetic woman → ECG → resting echo → TMT → stress echo → coronary angiography (two-vessel CAD)
- Case F.2: Young man with syncope → ECG → HCM echo → Holter (NSVT) → TMT (abnormal BP response) → ICD decision
- Case F.3: Post-cardiac surgery tamponade → POCUS diagnosis → emergency pericardiocentesis
More deeply explanation,information and analysis with pictures ,diagrams and graphs with complete pre ecg topics like what is heart,it's location, circulation, conduction, coronary ,action potential etc. And how all are inter relatable and what changes and abnormalities can affect the other and how it will appear in cardiac reports. The history of cardiology, ecg, tmt,holter,echo.how to prepare the patient. What is ecf paper,gelly and it's fundamentals, the theories, principles. What is color coding and why. Why the p,qrs,t and why not the other alphabet.
history of ECG electrocardiogram Einthoven PQRST naming origin Willem 1902
ECG paper standard 25mm/sec squares millivolts history ECG gel electrodes color coding limb leads
history of echocardiography Edler Hertz 1953 TMT treadmill stress test history Holter monitor history 1961
Complete Chapter Map of This Edition
Chapter 0 - History of Cardiology (The Full Timeline)
- Ancient Egypt (1550 BCE) → Ebers Papyrus; heart as center of life
- Aristotle (384 BCE) → wrong about brain cooling, correct about heart as center
- Ibn al-Nafis (1213 CE) → FIRST to describe pulmonary circulation (300 years before Harvey!)
- William Harvey (1628) → "De Motu Cordis" - quantitative proof of systemic circulation; Father of Modern Cardiology
- René Laennec (1816) → Invented the stethoscope from rolled paper
- Luigi Galvani (1791) → Discovered bioelectricity (frog legs experiment)
- Augustus Waller (1887) → First human ECG recording; his dog Jimmie was the first ECG "patient"
- Einthoven (1893-1924) → Named PQRST; String galvanometer; Nobel Prize 1924
- WHY PQRST NOT ABCDE - full 3-theory explanation (Descartes convention; room for future waves; practical reason - he already used A-D for the uncorrected tracing)
- History of Holter (Norman Holter 1914-1983; 38 kg backpack 1949 → modern patch)
- History of TMT (Master's Two-Step 1929 → Bruce Protocol 1956)
- History of Echo (Edler + Hertz 1953; borrowed industrial reflectoscope; "Father of Echocardiography")
Chapter 1 - What Is the Heart
- Heart = 100,000 beats/day, 2.5 billion in a lifetime, 60,000 miles of vessels
- Precise location (mediastinum, 2/3 left of midline, apex at 5th ICS MCL)
- Why the heart is tilted left (embryonic cardiac tube looping on day 23-28)
- Detailed 3-layer diagram (pericardium → myocardium → endocardium)
- All 4 chambers with internal landmarks (crista terminalis, fossa ovalis, moderator band, LA appendage)
- Valves - mechanism of opening/closing, MV leaflets (P1/P2/P3), aortic cusp anatomy and why Valsalva sinuses exist
Chapter 2 - Circulation
- Dual circulation diagram with pressures
- Coronary circulation in depth: LMCA → LAD (septal perforators + diagonals) + LCx (marginals); RCA (SA nodal artery + AV nodal artery + PDA)
- Coronary dominance (70% right, 15% left, 10-15% co-dominant) - why it matters clinically
- Ischemia Cascade diagram (seconds → diastolic dysfunction → wall motion → ECG → symptoms → necrosis → troponin) - explains timing for all tests
- Coronary → ECG → Echo wall segment correlation table
Chapter 3 - Conduction System
- Full conduction pathway diagram with locations, blood supply, intrinsic rates, speeds
- SA node (60-100 bpm; SA nodal artery); AV node (40-60 bpm; Koch's triangle); His bundle; RBB (moderator band!); LBB (3 fascicles); Purkinje (4 m/s fastest)
- Ventricular AP graph: all 5 phases with ions (INa, Ito, ICaL, IKr/IKs, IK1) + corresponding QT segments
- SA node AP graph: pacemaker potential, funny current (If), HCN channels, ivabradine mechanism
- Hierarchy of automaticity explained
- Conduction block at each level → ECG pattern summary
Chapter 4 - ECG Fundamentals
- ECG paper complete - 25 vs 50 mm/sec tables; thermosensitive paper; small box = 0.04 sec, large box = 0.20 sec (at 25mm/sec)
- Voltage calibration - 10mm = 1mV; double/half standard; always check calibration box
- ECG Gel chemistry - NaCl electrolytes, carbomer thickener, why it works (reduces skin impedance 100,000 Ω → 1,000 Ω)
- Electrode types (disposable self-adhesive Ag/AgCl hydrogel vs reusable suction)
- TWO COLOR CODING STANDARDS - AHA vs IEC full table for all 10 leads; mnemonics; consequences of lead reversal (mimics dextrocardia)
- Einthoven's Triangle - mathematical derivation; Einthoven's Law (II = I + III); augmented leads
- PQRST wave-by-wave explanation with why T is upright (reverse repolarization: EPI→ENDO repolarization + ENDO→EPI depolarization = both produce upward deflection in left-sided leads)
- U wave origin (Purkinje / M-cell repolarization)
Chapter 5 - Patient Preparation
- ECG: Supine position (why), skin prep steps, artifact recognition and causes (muscle, wander, AC interference)
- TMT: Day-before instructions, in-lab pre-test protocol, emergency equipment checklist, during and post-test monitoring
- Holter: Electrode positions (3-channel), patient diary instructions, activity restrictions, return protocol
- Echo: TTE (minimal prep), contrast echo, TEE full protocol (6-hour fast, sedation, bite guard, left lateral decubitus, post-procedure gag reflex recovery)
Chapter 6 - Interrelationships
- Grand unified diagram: Anatomy ↔ Echo; Physiology ↔ Echo; Electrophysiology ↔ ECG/Holter; Perfusion ↔ TMT/Stress Echo
- How Hypertension → LVH → affects all 4 tests simultaneously
- How MI → affects all 4 tests across acute/subacute/chronic phases
- How AF → affects all 4 tests
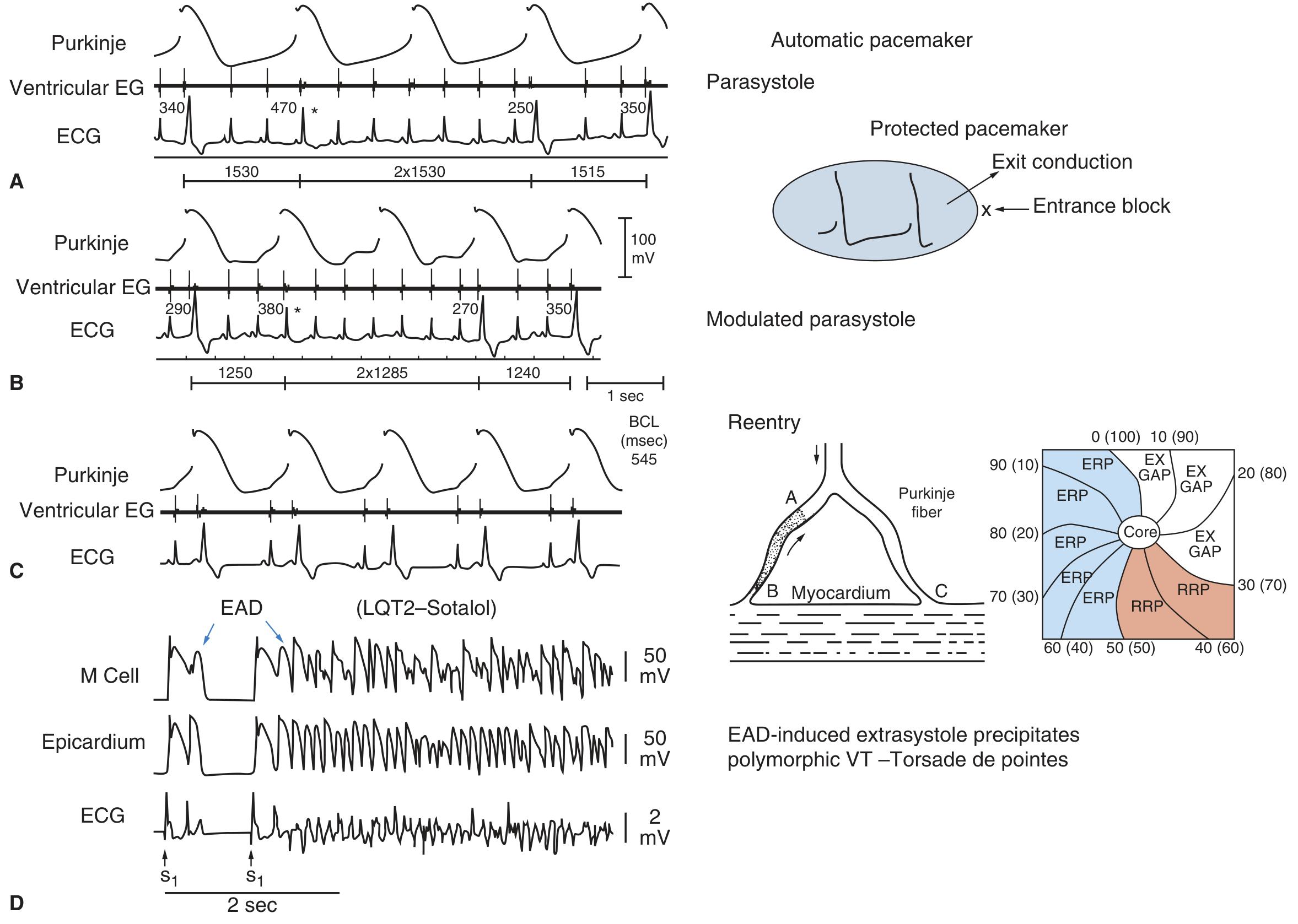
- 3 mechanisms of ALL arrhythmias (automaticity, triggered [EAD/DAD], reentry) with ECG examples
- Electrolytes (K+, Ca2+, Mg2+) → exactly how each affects AP phases → exactly what ECG changes result
- Complete cardiac examination flow diagram (when to order which test in which sequence)