I have my exam, pharmacology, final exam, uh, for MBBS. So my topic is insulin and oral antidiabetic drugs. Tell me everything that I should know. Done.
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything I need to write a comprehensive, exam-ready answer. Let me compile it all.
Insulin & Oral Antidiabetic Drugs - Complete MBBS Pharmacology Guide
Sources: Katzung's Basic & Clinical Pharmacology 16e, Lippincott Illustrated Reviews Pharmacology
Quick Orientation - Diagnostic Criteria (Know These Cold)
| Parameter | Normal | Prediabetes | Diabetes |
|---|---|---|---|
| Fasting plasma glucose | <100 mg/dL | 100-125 mg/dL | ≥126 mg/dL |
| 2h post-load glucose | <140 mg/dL | 140-199 mg/dL | ≥200 mg/dL |
| HbA1c | <5.7% | 5.7-6.4% | ≥6.5% |
Target HbA1c in treatment: ≤7% (ADA recommendation)
PART 1: INSULIN
Chemistry
Insulin is a small protein (MW 5808) with 51 amino acids in 2 chains (A and B) linked by disulfide bonds. It is synthesized as proinsulin (single chain) in the Golgi apparatus of beta cells, then cleaved into insulin + C-peptide (by removal of 4 amino acids). Both are secreted in equimolar amounts.
Exam fact: C-peptide has no known physiologic function but is a better marker of endogenous insulin secretion than plasma insulin itself (because insulin undergoes significant hepatic/renal extraction but C-peptide does not).
Insulin is stored in beta-cell granules as hexameric crystals (2 zinc atoms + 6 insulin molecules). The entire pancreas contains ~8 mg = ~200 biologic units.
Mechanism of Insulin Secretion (Very Exam-Heavy)
Glucose-stimulated pathway:
- Glucose enters beta cell via GLUT-2 transporter
- Phosphorylated by glucokinase (the glucose sensor)
- Glucose metabolism generates ATP
- Elevated ATP closes ATP-sensitive K+ channels (K-ATP channels)
- Membrane depolarization opens voltage-gated Ca2+ channels
- Ca2+ influx triggers pulsatile insulin exocytosis
Other stimulants of insulin release:
- Amino acids (leucine, arginine - gluconeogenic)
- GLP-1, GIP, glucagon, cholecystokinin
- Beta-adrenergic activity, acetylcholine
- Drugs: sulfonylureas, meglitinides, isoproterenol
Inhibitors of insulin release:
- Alpha-adrenergic activity, somatostatin, leptin
- Insulin itself (feedback), IAPP (amylin)
- Drugs: diazoxide (K-ATP channel opener), phenytoin, verapamil, clonidine, vinblastine, colchicine
Insulin Receptor & Mechanism of Action
The insulin receptor is a receptor tyrosine kinase (RTK) - a tetramer with 2 alpha subunits (extracellular, bind insulin) and 2 beta subunits (transmembrane, have intrinsic tyrosine kinase activity).
Binding of insulin → autophosphorylation of receptor → phosphorylation of insulin receptor substrates (IRS) → downstream signaling via PI3K/Akt pathway.
Metabolic effects of insulin:
| Tissue | Effect |
|---|---|
| Liver | ↑ glycogen synthesis, ↑ lipogenesis, ↓ gluconeogenesis, ↓ glycogenolysis, ↓ ketogenesis |
| Muscle | ↑ glucose uptake (GLUT-4), ↑ glycogen synthesis, ↑ protein synthesis |
| Adipose | ↑ glucose uptake (GLUT-4), ↑ lipogenesis, ↓ lipolysis |
| General | ↑ K+ entry into cells (used in hyperkalemia treatment!) |
Insulin Preparations - The Most Exam-Tested Table
| Preparation | Onset | Peak | Duration | Key Notes |
|---|---|---|---|---|
| Rapid-acting (lispro, aspart, glulisine) | 5-15 min | 1-1.5 h | 3-4 h | Give 15-30 min before meals |
| Regular (Short-acting) | 30-60 min | 2 h | 6-8 h | Only insulin given IV (emergencies) |
| Inhaled (Technosphere) | 5-15 min | 1 h | 3 h | Rapid-acting, inhalation only |
| NPH (Intermediate) | 2-4 h | 6-7 h | 10-20 h | Cloudy suspension, protamine added |
| Glargine (Long-acting) | 0.5-1 h | Flat (no peak) | ~24 h | Peakless, once daily |
| Detemir (Long-acting) | 0.5-1 h | Flat | 17 h | Albumin-bound |
| Degludec (Ultra-long) | 0.5-1.5 h | Flat | >42 h | Longest acting |
Mechanism of prolonged action for analogs:
- Glargine: Amino acid substitutions at A21 (Asn→Gly) and B30-31 (Arg added) → precipitates at physiological pH (SC tissue) → slow absorption
- Detemir: Fatty acid chain attached → binds albumin → slow release
- Lispro: Reversal of Pro-Lys at B28-29 → prevents hexamer formation → faster absorption
- Aspart: Asp substituted at B28 → same rapid effect
Exam rule: Regular insulin is the ONLY insulin given IV. All others are subcutaneous only.
Adverse Effects of Insulin
- Hypoglycemia - most common and serious
- Weight gain
- Lipodystrophy at injection site
- Lipoatrophy (older animal insulins) - corrects with human insulin injection at site
- Lipohypertrophy (still occurs) - prevent by rotating sites
- Insulin allergy - IgE-mediated, immediate hypersensitivity, rare with modern human/analog insulins. Severe cases: anaphylaxis
- Immune insulin resistance - IgG antibodies (usually low titer, clinically insignificant; rarely causes true resistance)
- Hypokalemia - insulin drives K+ into cells
Standard vs. Intensive Insulin Therapy
| Standard | Intensive | |
|---|---|---|
| Injections | 2/day | ≥3/day |
| Monitoring | Routine | Frequent glucose checks |
| HbA1c | Higher | ≤7% target |
| Hypoglycemia risk | Lower | Higher |
| Microvascular complications | More | Significantly reduced (retinopathy, nephropathy, neuropathy) |
Intensive therapy should not be used in: long-standing diabetes, significant microvascular complications, elderly, hypoglycemic unawareness.
PART 2: ORAL ANTIDIABETIC DRUGS (Type 2 Diabetes)
The progression of Type 2 DM and treatment escalation:
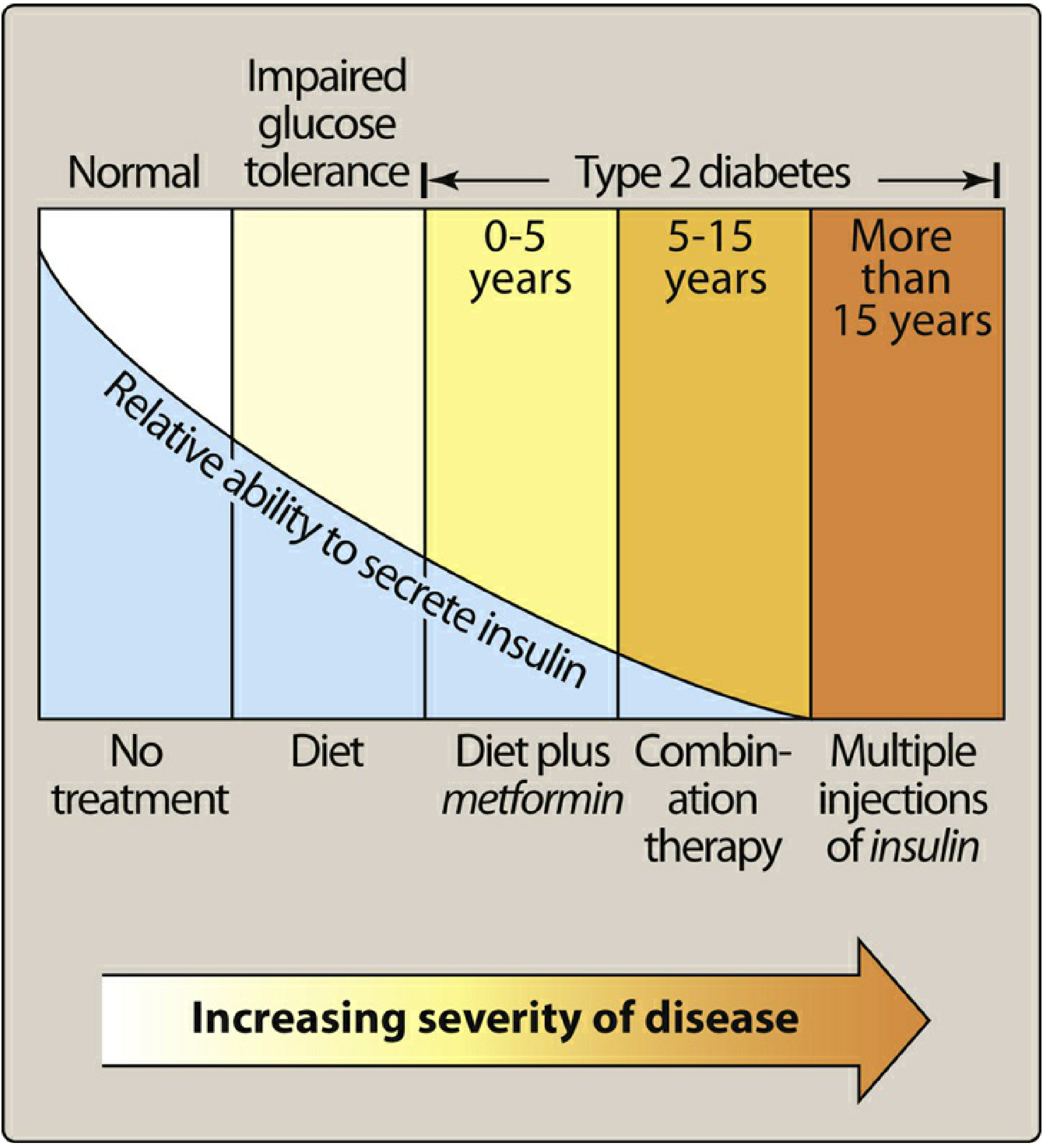
Categories (Katzung's 6-Group Classification)
- Insulin secretagogues acting on K-ATP channel (sulfonylureas, meglitinides)
- Insulin sensitizers (biguanides, thiazolidinediones)
- Alpha-glucosidase inhibitors (delay carbohydrate absorption)
- Incretin-based (GLP-1 receptor agonists, DPP-4 inhibitors)
- SGLT2 inhibitors (renal glucose excretion)
- Others (pramlintide, bromocriptine, colesevelam)
1. BIGUANIDES - Metformin (FIRST-LINE DRUG)
Drug: Metformin (only available biguanide)
Mechanism:
- Primarily reduces hepatic gluconeogenesis (main mechanism)
- Slows intestinal absorption of sugars
- Improves peripheral glucose uptake and utilization (increases insulin sensitivity)
- Activates AMPK (AMP-activated protein kinase) - underlying molecular mechanism
- Does NOT stimulate insulin secretion → minimal hypoglycemia risk when used alone
Pharmacokinetics:
- Well absorbed orally, not protein-bound, not metabolized
- Excreted unchanged by kidneys
Adverse effects:
- GI (most common): nausea, diarrhea, vomiting - minimize by slow dose titration, take with meals
- Lactic acidosis (rare but serious, especially in renal failure)
- Weight loss (appetite suppression - desirable)
- Long-term use → Vitamin B12 deficiency (reduced absorption)
- Does NOT cause hypoglycemia alone
Contraindications:
- eGFR < 30 mL/min/1.73 m² (contraindicated due to lactic acidosis risk)
- eGFR 30-45: use with caution
- Acute MI, liver disease, severe dehydration, contrast dye use (hold 48h)
- Alcoholism
Special uses: Also used in polycystic ovary syndrome (PCOS) and prevention of T2DM in prediabetes
2. SULFONYLUREAS (Insulin Secretagogues)
Drugs:
- 1st generation (older): Tolbutamide, chlorpropamide, tolazamide
- 2nd generation (preferred): Glibenclamide (glyburide), glipizide, glimepiride, gliclazide
Mechanism:
- Bind to sulfonylurea receptor (SUR-1) on beta cell K-ATP channels
- Block K+ efflux → membrane depolarization → Ca2+ influx → insulin release
- Require functional beta cells to work (useless in Type 1 DM)
- Some extrapancreatic effects (↑ insulin receptor sensitivity) - minor
Pharmacokinetics:
- All well-absorbed orally, highly protein-bound (albumin)
- Chlorpropamide: longest half-life (~35h), renally excreted - avoid in elderly/renal disease
- Glipizide: short-acting, preferred in elderly
- Glimepiride: once-daily, weight neutral
Adverse effects:
- Hypoglycemia - most important (especially chlorpropamide, glyburide - long-acting)
- Weight gain
- GI upset, skin reactions
- Disulfiram-like reaction with alcohol (chlorpropamide especially)
- Hyponatremia (SIADH - chlorpropamide)
- Cholestatic jaundice (rare)
- Hemolytic anemia in G6PD deficiency
Drug interactions:
- Potentiated by: NSAIDs, sulfonamides, warfarin, fluconazole (displace from protein binding)
- Inhibited by: thiazides, corticosteroids, phenytoin, rifampicin
Contraindications: Type 1 DM, pregnancy, renal/hepatic failure, stress states (surgery, infection)
3. MEGLITINIDES (Glinides)
Drugs: Repaglinide, Nateglinide
Mechanism:
- Also bind SUR-1 (different binding site than sulfonylureas) → close K-ATP channels → insulin release
- Glucose-dependent - only effective when glucose is elevated
- Short-acting - taken just before meals, cover postprandial glucose
Advantages over sulfonylureas:
- Shorter action = less hypoglycemia risk
- More flexibility (can skip dose if skipping meal)
- Can be used in mild renal impairment
Adverse effects: Hypoglycemia (less than SU), weight gain
4. THIAZOLIDINEDIONES (TZDs / Glitazones)
Drugs: Pioglitazone, Rosiglitazone
Mechanism:
- Bind PPARγ (peroxisome proliferator-activated receptor gamma) - a nuclear receptor
- Alter gene transcription → ↑ insulin sensitivity in muscle, liver, adipose tissue
- ↑ GLUT-4 expression, ↑ adiponectin, ↓ FFA levels
- Do NOT stimulate insulin secretion
- Require insulin to be present to work
Adverse effects:
- Weight gain (fluid retention + increased fat mass)
- Fluid retention / edema → can precipitate or worsen heart failure (contraindicated in heart failure)
- Rosiglitazone: associated with increased risk of MI - significantly restricted/withdrawn in many countries
- Pioglitazone: associated with increased risk of bladder cancer (prolonged use)
- Bone fractures (increased in women, especially at distal extremities)
- Elevated LFTs (hepatotoxicity - troglitazone withdrawn for this reason)
- Anemia (hemodilution)
Onset: Slow - takes 4-12 weeks for full effect (gene transcription mechanism)
5. ALPHA-GLUCOSIDASE INHIBITORS
Drugs: Acarbose, Miglitol, Voglibose
Mechanism:
- Reversibly inhibit alpha-glucosidase enzymes (sucrase, maltase, etc.) in the brush border of the small intestine
- Delay digestion and absorption of complex carbohydrates
- Lower postprandial glucose (not fasting glucose)
Pharmacokinetics: Minimally absorbed (works locally in gut)
Adverse effects:
- Flatulence, abdominal bloating, diarrhea (most common - undigested carbs fermented by gut bacteria)
- Rarely: elevated liver enzymes (high doses of acarbose)
- Do NOT cause hypoglycemia alone
Important: If hypoglycemia occurs in a patient on acarbose + insulin/sulfonylurea, treat with glucose (dextrose), NOT sucrose - because acarbose blocks sucrase!
6. DPP-4 INHIBITORS (Gliptins)
Drugs: Sitagliptin, Saxagliptin, Alogliptin, Linagliptin, Vildagliptin
Mechanism:
- Inhibit dipeptidyl peptidase-4 (DPP-4) enzyme
- DPP-4 normally degrades incretin hormones (GLP-1, GIP) - they have half-life of ~2 minutes
- Inhibiting DPP-4 → ↑ endogenous GLP-1 and GIP levels
- → ↑ glucose-dependent insulin secretion, ↓ glucagon
- Glucose-dependent → low hypoglycemia risk
Adverse effects:
- Generally well tolerated
- Nasopharyngitis, upper respiratory tract infections
- Pancreatitis (risk - black box warning)
- Joint pain (arthralgia)
- Saxagliptin: increased risk of heart failure hospitalizations
Advantage: Weight neutral, low hypoglycemia risk
7. GLP-1 RECEPTOR AGONISTS (Incretin Mimetics)
Drugs: Exenatide, Liraglutide, Dulaglutide, Semaglutide, Lixisenatide
Mechanism:
- Mimic GLP-1 (incretin hormone from gut L-cells)
- Glucose-dependent ↑ insulin secretion, ↓ glucagon
- Slow gastric emptying (reduces postprandial glucose)
- Decrease appetite (central satiety effect) → weight loss
- Some: cardioprotective effects (MACE reduction - liraglutide, semaglutide)
Route: Subcutaneous injection (except semaglutide - also available orally)
Adverse effects:
- Nausea, vomiting (most common - usually transient)
- Pancreatitis risk
- Risk of thyroid C-cell tumors (rodent data - avoid in medullary thyroid cancer, MEN2)
- Weight loss (beneficial in obese T2DM)
Advantages: Weight loss, low hypoglycemia risk, cardiovascular benefit (liraglutide, semaglutide approved for CV risk reduction)
Exam fact: GLP-1 agonists are not broken down by DPP-4 because they are structurally modified - they are "DPP-4 resistant."
8. SGLT2 INHIBITORS (Gliflozins / Flozins)
Drugs: Empagliflozin, Dapagliflozin, Canagliflozin, Ertugliflozin
Mechanism:
- Inhibit Sodium-Glucose Co-Transporter 2 (SGLT2) in the proximal renal tubule
- SGLT2 is responsible for ~90% of renal glucose reabsorption
- Inhibition → glucosuria (glucose excreted in urine) → lowers blood glucose
- Also causes natriuresis → reduces blood pressure and preload
- Insulin-independent mechanism
Additional benefits:
- Cardiovascular: Reduce hospitalization for heart failure, mortality (empagliflozin and dapagliflozin approved for heart failure with and without diabetes)
- Renal: Slow progression of CKD (dapagliflozin beneficial even without diabetes)
- Weight loss (calorie loss in urine)
Adverse effects:
- Genital mycotic infections (women > men) - most common
- Urinary tract infections, pyelonephritis, urosepsis
- Euglycemic diabetic ketoacidosis (rare - especially if Type 1 off-label or very insulin-deficient T2DM)
- Necrotizing fasciitis of perineum (Fournier gangrene) - rare but serious
- Hypotension / volume depletion
- Canagliflozin: increased fracture risk, increased amputation risk (toes)
- Modest LDL increase (canagliflozin, empagliflozin)
Contraindications: eGFR < 45 (for glycemic benefit); eGFR < 30 (contraindicated)
9. AMYLIN ANALOG
Drug: Pramlintide
Mechanism:
- Synthetic analog of amylin (IAPP - co-secreted with insulin from beta cells)
- Delays gastric emptying, ↓ postprandial glucagon, ↑ satiety
- SC injection before meals
Use: Adjunct to mealtime insulin in Type 1 and Type 2 DM
Adverse effects:
- Nausea, vomiting, anorexia
- Severe hypoglycemia - reduce mealtime insulin dose by 50% when starting
- Cannot be mixed in same syringe as insulin
- Contraindicated in: gastroparesis, hypoglycemic unawareness
PART 3: KEY COMPARISONS & EXAM TABLES
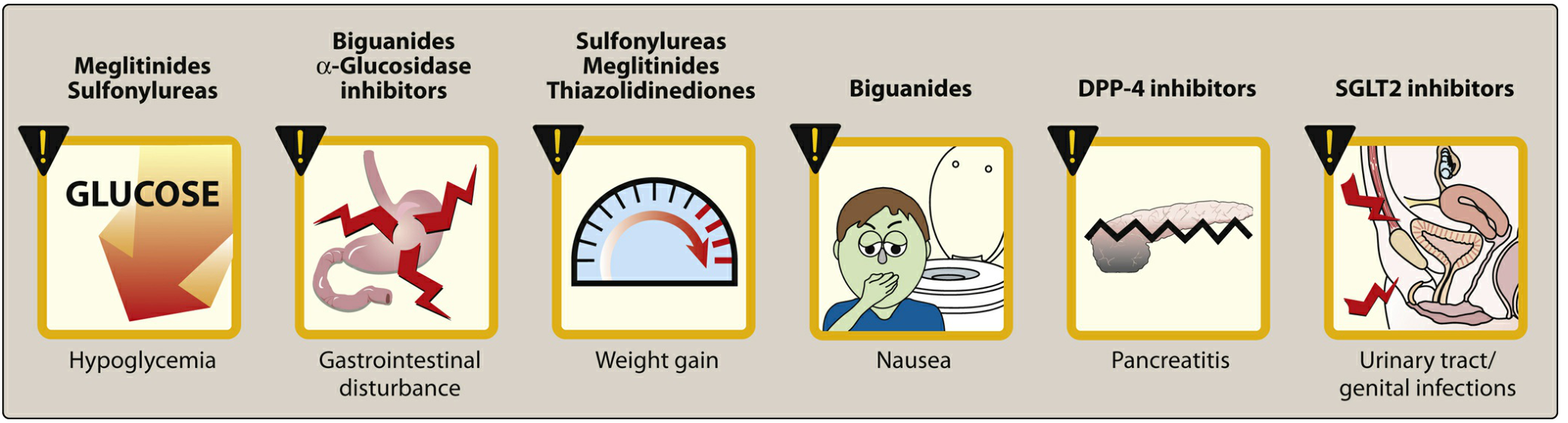
Adverse Effects Summary Chart
Which Drugs Cause Hypoglycemia?
| Cause Hypoglycemia | Do NOT Cause Hypoglycemia Alone |
|---|---|
| Insulin | Metformin |
| Sulfonylureas | Thiazolidinediones |
| Meglitinides | Alpha-glucosidase inhibitors |
| (When combined with insulin secretagogues) | DPP-4 inhibitors |
| GLP-1 agonists | |
| SGLT2 inhibitors |
Weight Effects
| Weight Gain | Weight Loss/Neutral |
|---|---|
| Insulin | Metformin (mild loss) |
| Sulfonylureas | GLP-1 agonists (loss) |
| Meglitinides | SGLT2 inhibitors (loss) |
| Thiazolidinediones | DPP-4 inhibitors (neutral) |
| Alpha-glucosidase inhibitors (neutral) |
Drug Choice in Special Situations (High-Yield Exam Topics)
| Situation | Drug of Choice |
|---|---|
| First-line Type 2 DM | Metformin |
| Type 2 DM + Heart Failure | SGLT2 inhibitors (empagliflozin, dapagliflozin) |
| Type 2 DM + CKD | SGLT2 inhibitors (also renoprotective) |
| Type 2 DM + Obesity | GLP-1 agonists (weight loss benefit) |
| Type 2 DM + CV disease | GLP-1 agonists or SGLT2 inhibitors |
| Type 2 DM + Elderly (hypoglycemia risk) | Glipizide (short-acting SU) or DPP-4 inhibitor |
| Pregnancy | Insulin (only safe option - metformin/glibenclamide used off-label in some guidelines) |
| Type 1 DM | Insulin (mandatory) |
| Postprandial glucose control | Alpha-glucosidase inhibitors, meglitinides, rapid-acting insulin |
| Hyperglycemic emergency (DKA, HHS) | IV Regular Insulin |
| PCOS with insulin resistance | Metformin |
Contraindications Summary
| Drug | Key Contraindication |
|---|---|
| Metformin | eGFR <30, liver failure, contrast dye, acute MI |
| Thiazolidinediones | Heart failure, liver disease, bladder cancer (pioglitazone) |
| SGLT2 inhibitors | eGFR <45 (glycemic benefit), Type 1 DM (DKA risk) |
| GLP-1 agonists | Medullary thyroid carcinoma, MEN2, pancreatitis history |
| Sulfonylureas | Type 1 DM, renal failure (avoid long-acting), pregnancy |
| Pramlintide | Gastroparesis, hypoglycemic unawareness |
Mechanism Quick Reference
| Drug Class | MOA in One Line |
|---|---|
| Sulfonylureas | Block K-ATP channels → depolarization → Ca2+ influx → insulin release |
| Meglitinides | Same (different SUR binding site), shorter acting, meal-time |
| Biguanides (Metformin) | ↓ hepatic gluconeogenesis via AMPK activation |
| TZDs | Activate PPARγ → ↑ insulin sensitivity |
| Alpha-glucosidase inhibitors | Block brush border enzymes → delay carbohydrate absorption |
| DPP-4 inhibitors | Inhibit DPP-4 → ↑ endogenous GLP-1/GIP → ↑ glucose-dependent insulin secretion |
| GLP-1 agonists | Mimic GLP-1 → ↑ glucose-dependent insulin, ↓ glucagon, ↓ gastric emptying |
| SGLT2 inhibitors | Block renal glucose reabsorption → glucosuria |
| Pramlintide | Amylin analog → ↓ gastric emptying, ↓ glucagon, ↑ satiety |
PART 4: HIGH-YIELD EXAM POINTS (Don't Miss These)
-
C-peptide = better measure of endogenous insulin (insulin undergoes hepatic first-pass; C-peptide does not). Equimolar with insulin secretion.
-
Glucokinase = the glucose sensor of beta cells (not hexokinase - glucokinase has low affinity, not saturated at normal glucose, acts only when glucose is high).
-
Regular insulin = only insulin for IV use. Used in emergencies (DKA, HHS, hyperkalemia).
-
NPH = Neutral Protamine Hagedorn - protamine is added to retard absorption (intermediate-acting, cloudy).
-
Glargine = peakless - precipitates at physiological pH in SC tissue due to its pH modification (prepared at pH 4, precipitates at pH 7.4).
-
Lactic acidosis with metformin = most feared adverse effect, especially with renal failure (drug accumulates).
-
Disulfiram-like reaction = chlorpropamide (1st generation SU) + alcohol.
-
Hyponatremia/SIADH = chlorpropamide (1st gen SU, potentiates ADH).
-
Rosiglitazone = associated with MI (restricted globally). Pioglitazone = bladder cancer risk. Both TZDs worsen heart failure.
-
Acarbose + hypoglycemia = treat with dextrose (glucose), NOT sucrose (blocked by acarbose).
-
GLP-1 half-life = ~2 min (degraded by DPP-4). Synthetic GLP-1 analogs are modified to resist DPP-4.
-
Euglycemic DKA = SGLT2 inhibitor complication - glucose is normal but pH is low. Dangerous because patient/doctor may be misled by normal glucose.
-
Fournier gangrene = necrotizing fasciitis of perineum - rare SGLT2 inhibitor adverse effect.
-
Pramlintide + mealtime insulin = reduce insulin dose by 50% to avoid severe hypoglycemia.
-
Incretin effect = oral glucose causes much greater insulin secretion than IV glucose (due to gut incretin hormones GLP-1, GIP) - this effect is reduced in Type 2 DM.
Katzung's Basic and Clinical Pharmacology, 16th Edition, Ch. 41; Lippincott Illustrated Reviews: Pharmacology, Ch. 24
This is a shared conversation. Sign in to Orris to start your own chat.