Answer to questions Colles fracture Anterior shoulder dislocation [manuvers,managemnet,complications] Blood supply of neck of femur from standard orthopedic textbook according to cbme circulum in detail
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the information needed for a comprehensive, well-illustrated answer. Here is the complete response:
1. COLLES' FRACTURE
Definition
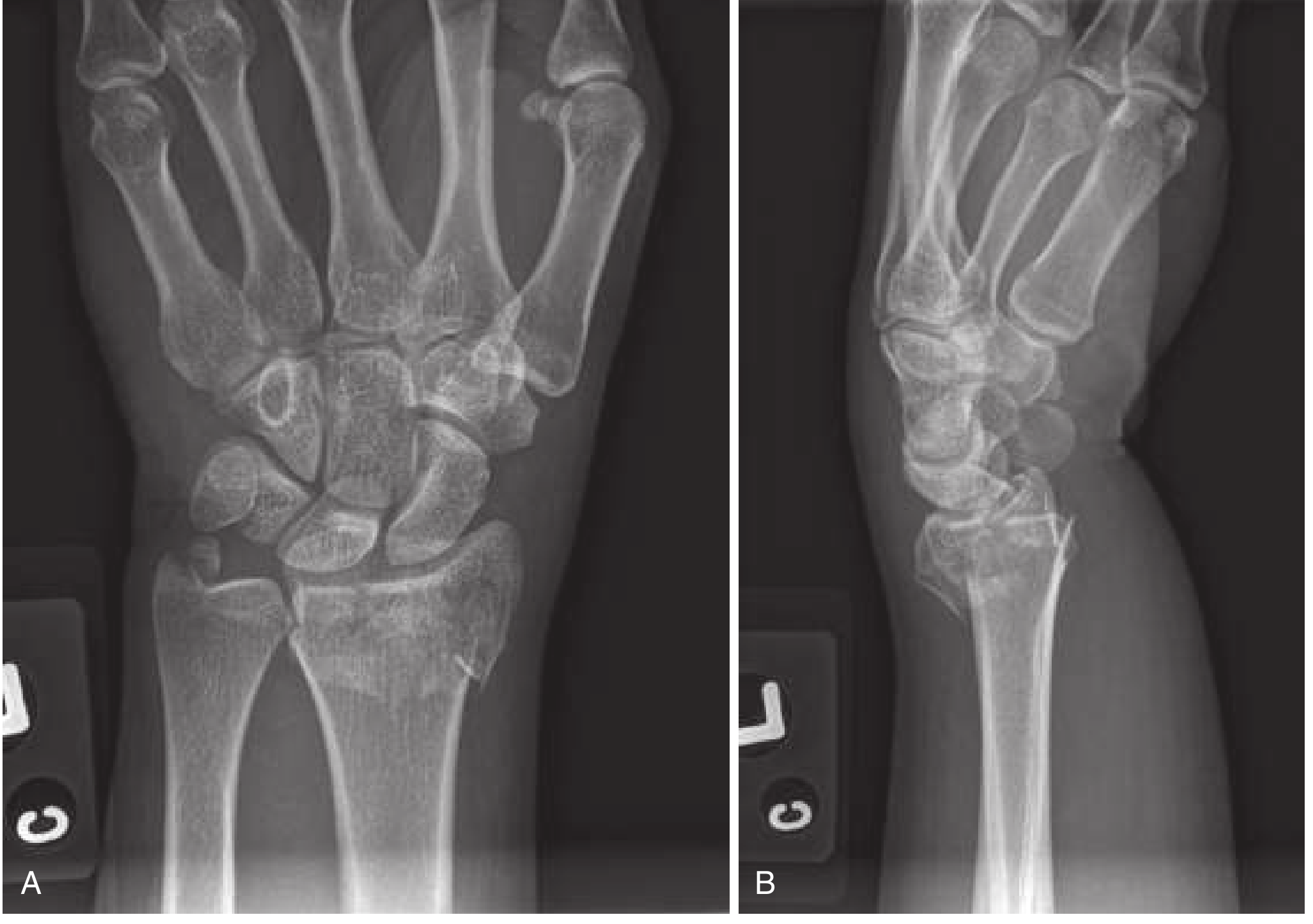
A Colles' fracture is a transverse fracture of the distal radial metaphysis (within 2 cm of the radial articular surface) that is dorsally displaced and angulated (dorsal displacement + dorsal angulation). It results from a fall on the outstretched, extended hand (FOOSH injury).
Classic Features
- Dinner fork deformity - wrist has dorsiflexion deformity resembling an upside-down fork
- Occurs mostly in elderly women (osteoporotic bone)
- May be associated with: dorsal comminution, intra-articular extension into radiocarpal/radioulnar joints, and ulnar styloid fracture (which may indicate triangular fibrocartilage complex (TFCC) injury)
- Median nerve compression may present as palmar paresthesias
Radiological Features
- PA view: shortened radius, possible intra-articular extension, associated ulnar styloid fracture
- Lateral view: dorsal angulation and displacement, loss of normal volar tilt of distal radial articular surface
Signs of Instability (requiring surgery)
- Dorsal angulation >20 degrees
- Intra-articular involvement
- Marked comminution
- Radial shortening >1 cm
Management
Stable fractures
- Compression dressing and splint; orthopedic follow-up in 7-10 days
Unstable fractures - Closed Reduction
Goal: Restore volar tilt, radial inclination, and radial length
Anesthesia options:
- Hematoma block: 22-gauge needle into dorsum of distal radius, aspirate hematoma, instill 5-10 mL of 1% or 2% lidocaine
- IV regional anesthesia (Bier block)
- Regional nerve blocks (median, radial, ulnar, brachial plexus)
- Procedural sedation
Reduction technique (finger trap method):
- Apply finger traps to relax deforming muscle spasm
- Apply traction with finger traps
- Push fragment distal and palmar while holding the forearm firmly
- Restore volar tilt (minimum neutral/zero degrees acceptable)
Immobilization: Double sugar-tong splint (NOT circumferential cast acutely - edema risk). Short-arm cast may be used if bivalved. Immobilize 4-6 weeks.
Operative Indications
- Open fractures
- Neurovascular compromise
- Unstable/severely comminuted/intra-articular fractures
- Failed closed reduction
Complications
Occur in 6-80% of cases (more common in elderly, comminuted, displaced fractures):
| Complication | Notes |
|---|---|
| Median nerve injury | Most common nerve injury; acute contusion, traction, or compression; also from cast pressure |
| Malunion | Most common long-term complication; residual dorsal angulation |
| Sudeck's atrophy (CRPS I) | Complex regional pain syndrome |
| Rupture of extensor pollicis longus (EPL) | Classic delayed complication; rupture at Lister's tubercle |
| Carpal tunnel syndrome | Due to median nerve compression |
| Radiocarpal / radioulnar arthritis | Especially with intra-articular fractures |
| Stiffness | Finger/wrist stiffness from immobilization |
| Distal radioulnar joint instability | From TFCC injury or malunion |
| Ulnar nerve injury | Less common than median |
Source: Rosen's Emergency Medicine; Tintinalli's Emergency Medicine
2. ANTERIOR SHOULDER DISLOCATION
Overview
Anterior dislocations account for ~95% of all shoulder dislocations. The humeral head typically displaces subcoracoid (most common), subglenoid, or subclavicular. The mechanism is usually forced external rotation and abduction.
Reduction Maneuvers
A. Stimson Maneuver (Gravity-assisted)
- Patient lies prone with arm hanging off the edge of the stretcher
- 5 kg weights are attached to the wrist/forearm
- Gravity pulls the humeral head inferiorly for 20-30 minutes
- Scapular manipulation or gentle ER/IR rotation can be added to aid reduction
- Safe, requires no force, but slow
B. Scapular Manipulation
- Can be done with patient prone (combined with Stimson) or seated
- Rotate the inferior tip of the scapula medially and dorsally toward the spine using thumbs
- If seated: assistant applies traction on the arm while countertraction is on the ipsilateral clavicle
C. "Best of Both" Technique
- Patient seated sideways with unaffected shoulder and hip against stretcher head
- Operator applies downward force on patient's flexed forearm with gentle IR/ER rotation
- Assistant simultaneously performs scapular manipulation
D. External Rotation Method (Hennepin Technique)
- Fully adduct the arm, flex elbow to 90 degrees
- Hold the patient's wrist and guide the arm into slow, gentle external rotation
- Pause momentarily if patient experiences pain
- Continue until forearm is lying on the bed (full ER)
- No traction applied - very gentle, low force
E. Milch Technique
- Start with arm at 10-20 degrees of flexion and slight abduction
- Slowly elevate (abduct) the arm overhead with gentle distal traction
- Once overhead, apply gentle direct pressure on the humeral head to guide it into the glenoid
- If reduction does not occur, bring arm through a full lateral downward arc with outward traction
F. Traction-Countertraction Method
- One sheet wrapped around affected axilla and assistant's waist (countertraction)
- Another sheet around patient's flexed arm and operator's waist (traction)
- Both lean back simultaneously
- Can adduct the arm after traction is applied and apply lateral traction on the humerus
G. Spaso Technique
- Patient supine; operator lifts the arm toward the ceiling applying gentle vertical traction
- Assistant applies countertraction at the shoulder
- Gentle external rotation applied during the procedure
- Single-operator technique; 87.5% success rate reported; comparable efficacy to external rotation method but faster
H. Hippocratic Technique (Historical only - NOT recommended)
- Operator places foot against chest wall for countertraction
- No longer recommended due to serious neurovascular trauma risk
Management
Pre-reduction
- X-ray to confirm direction of dislocation and check for fractures (AP + axillary/scapular Y view)
- Analgesia and muscle relaxation (procedural sedation, intra-articular lidocaine, or IV opioids)
- Neurovascular exam (axillary nerve - test deltoid sensation and motor function)
Reduction
- Choose maneuver based on patient cooperation and operator experience
- External rotation and Spaso techniques work well without sedation
- Stimson and traction-countertraction require more assistance
Post-reduction
- Confirm reduction with post-reduction X-ray
- Repeat neurovascular exam
- Immobilization in a sling:
- Age <20 years: 3 weeks
- Age 20-40 years: 1-2 weeks
- Age >60 years: <1 week (to avoid stiffness)
- Physiotherapy after immobilization with emphasis on internal rotator strengthening
- Avoid external rotation + abduction combined for 3 months
Indications for Surgery
- Irreducible dislocation (rare; may need general anesthesia)
- Associated greater tuberosity fracture displaced >1 cm
- Associated glenoid rim fracture (bony Bankart) with >25% glenoid defect
- Recurrent instability (Bankart repair, Latarjet procedure)
Complications
| Complication | Details |
|---|---|
| Axillary nerve injury | Most common nerve injury; numbness over deltoid "regimental badge" area; test before and after reduction |
| Hill-Sachs lesion | Impaction fracture on posterolateral humeral head from dislocation against glenoid rim; present in up to 50% of anterior dislocations |
| Bankart lesion | Avulsion of the anteroinferior glenoid labrum with or without bony fragment; predisposes to recurrence |
| Recurrent instability/dislocation | Age at first dislocation is the main predictor; young patients (<20 yrs) have up to 90% recurrence rate |
| Rotator cuff tear | More common in patients >40-60 years; especially supraspinatus |
| Greater tuberosity fracture | Associated in ~15% of anterior dislocations |
| Vascular injury | Axillary artery injury; rare but serious; more common in elderly with atherosclerosis |
| Brachial plexus injury | Less common; usually neurapraxia |
| Hemarthrosis | More common with inferior dislocation and age >60 |
| Iatrogenic fracture | From forceful reduction technique |
Source: Roberts and Hedges' Clinical Procedures in Emergency Medicine; Pfenninger and Fowler's Procedures for Primary Care
3. BLOOD SUPPLY OF THE NECK OF FEMUR
Overview
The blood supply to the femoral head and neck is precarious due to the anatomy of the hip joint capsule. This is clinically critical because displaced intracapsular fractures and hip dislocations can disrupt these vessels, leading to avascular necrosis (AVN) of the femoral head.
Sources of Blood Supply
The femoral head receives blood from three main sources:
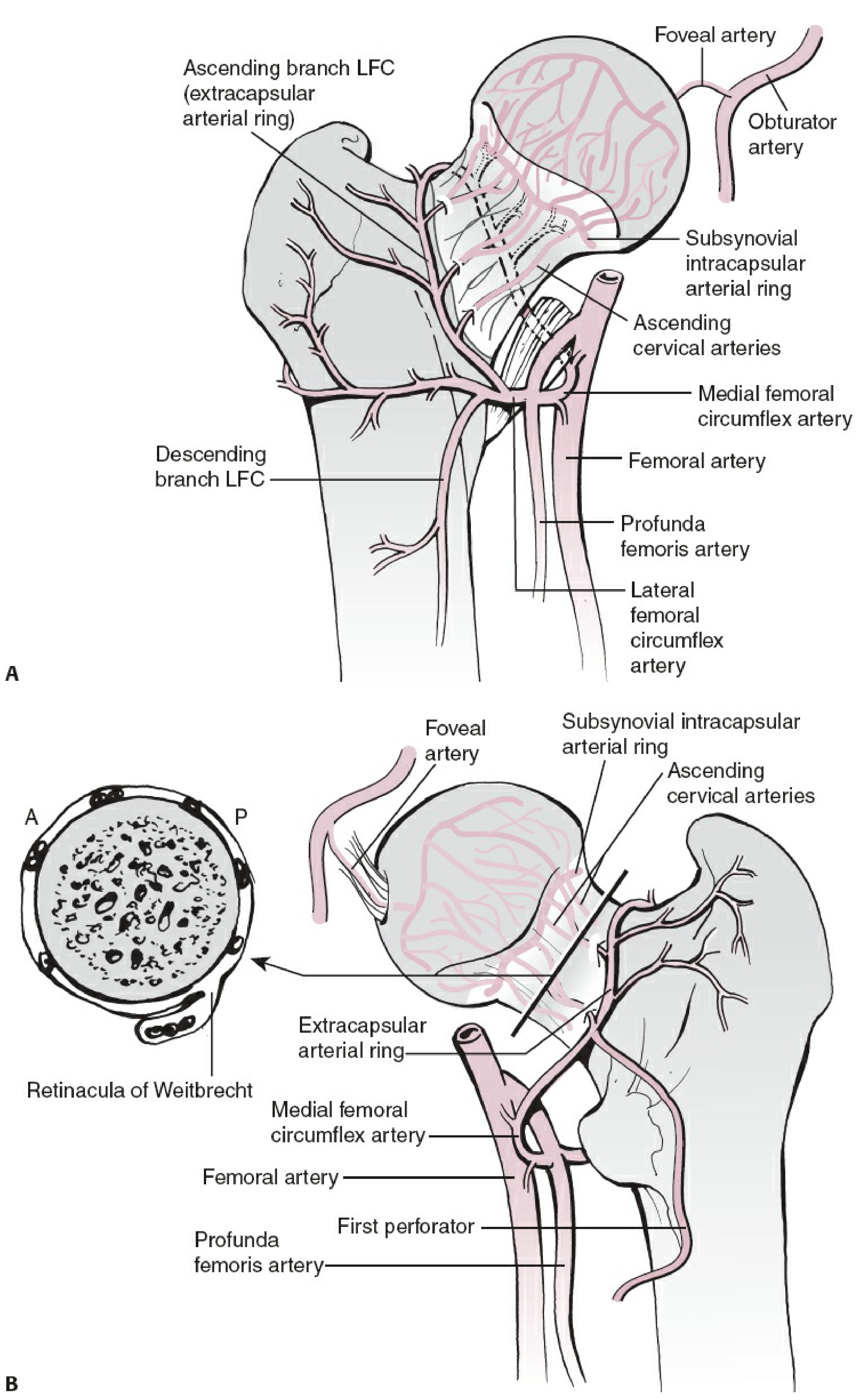
1. Medial Femoral Circumflex Artery (MFCA) - MOST IMPORTANT
- Arises from the profunda femoris (deep femoral artery) - occasionally directly from the femoral artery
- Runs posteriorly around the femoral neck
- Provides ~82% of total femoral head blood supply
- At the level of the femoral neck, the MFCA divides into terminal branches called retinacular arteries (also called capsular vessels or capital vessels)
- These retinacular vessels travel along the femoral neck under the synovium (subsynovial intracapsular ring) and penetrate the femoral head at the cervicocephalic junction
- There are 4 groups of retinacular vessels (anterior, medial, lateral - largest contributor, posterior)
- The lateral (superior) retinacular arteries are the most important - they supply the critical weight-bearing area of the femoral head
2. Lateral Femoral Circumflex Artery (LFCA)
- Also from profunda femoris
- Provides ~18% of femoral head blood supply (less important)
- Anastomoses with MFCA to form the extracapsular arterial ring at the base of the femoral neck
3. Artery of the Ligamentum Teres (Foveal Artery)
- Branch of the obturator artery (or MFCA)
- Enters the femoral head through the ligamentum teres at the fovea
- Supplies a small area around the fovea
- NOT sufficient to maintain viability of the entire femoral head if retinacular vessels are disrupted
- In adults, its contribution is variable and generally minor
4. Metaphyseal Vessels (Medullary Vessels)
- Enter via the femoral neck medullary canal
- Also disrupted in displaced neck fractures
Vascular Architecture (Step-by-Step)
Femoral artery / Profunda femoris
│
├── Medial Femoral Circumflex A (MFCA) [posterior route]
│ │
│ └── Extracapsular arterial ring
│ │
│ └── Retinacular arteries (travel under synovium along neck)
│ │
│ └── Subsynovial intracapsular arterial ring
│ │
│ └── Ascending cervical arteries → Femoral head
│
├── Lateral Femoral Circumflex A (LFCA) [anterior route]
│ └── Extracapsular arterial ring (minor contribution)
│
└── Obturator artery
└── Foveal artery (ligamentum teres) → Fovea of femoral head
Key Anatomical Points
- The Retinacula of Weitbrecht are condensations of the hip joint capsule along the femoral neck surface that carry the retinacular vessels
- The hip joint capsule extends to the intertrochanteric line anteriorly, but posteriorly only covers the medial half of the femoral neck - the lateral half of the posterior neck is extracapsular
- The MFCA must be protected in surgical approaches to the hip (e.g., at the level of the piriformis tendon/posterior capsule where it gives its terminal branches)
Why Femoral Neck Fractures Cause AVN
- The retinacular vessels travel along the surface of the femoral neck inside the capsule
- A displaced intracapsular fracture (subcapital >> transcervical) shears these vessels
- The foveal artery alone cannot supply the whole head
- Loss of blood supply → osteonecrosis of the femoral head (rate: ~15-50% in displaced fractures)
The Garden classification of femoral neck fractures predicts AVN risk:
- Garden I & II (undisplaced) - low AVN risk
- Garden III & IV (displaced) - high AVN risk (30-50%)
Source: Rockwood and Green's Fractures in Adults 10th ed (2025); THIEME Atlas of Anatomy - General Anatomy and Musculoskeletal System; Osteosynthesis and Hemiarthroplasty textbook
This is a shared conversation. Sign in to Orris to start your own chat.