Estrogen drug
Reading File
Finding Sources
Searching PubMed
"estrogen" AND "pharmacology"
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a thorough overview of estrogen drugs based on Goodman & Gilman's Pharmacological Basis of Therapeutics.
Estrogen Drugs - Complete Pharmacology
1. What Are Estrogens?
Estrogens are female sex hormones - both endogenous and synthetic - that act on estrogen receptors (ERs) to regulate reproduction, metabolism, bone density, cardiovascular function, and many other physiological processes. The most potent naturally occurring estrogen is 17β-estradiol, followed by estrone and estriol. Each contains a phenolic A ring with a hydroxyl group at carbon 3, which is the key structural feature for receptor binding. - Goodman & Gilman's, Chapter 48
2. Endogenous Estrogens
| Estrogen | Relative Potency | Source |
|---|---|---|
| 17β-Estradiol (E2) | Most potent | Ovarian granulosa cells (premenopausal) |
| Estrone (E1) | Intermediate | Conversion from androstenedione (postmenopausal) |
| Estriol (E3) | Weakest | Fetoplacental unit (dominant in pregnancy) |
Biosynthesis requires aromatase (CYP19), which converts androgens (androstenedione, testosterone) into estrogens by aromatizing the A ring.
3. Mechanisms of Action
Estrogens act via two main pathways:
Genomic (Nuclear Receptor) Pathway - Primary Mechanism
Estrogens bind to nuclear ERα or ERβ receptors, causing:
- Receptor dimerization
- Binding to Estrogen Response Elements (EREs) on DNA (consensus sequence: GGTCAnnnTGACC)
- Recruitment of coactivators (SRC-1, SWI/SNF, p300, TRAP complex) → chromatin remodeling → gene transcription
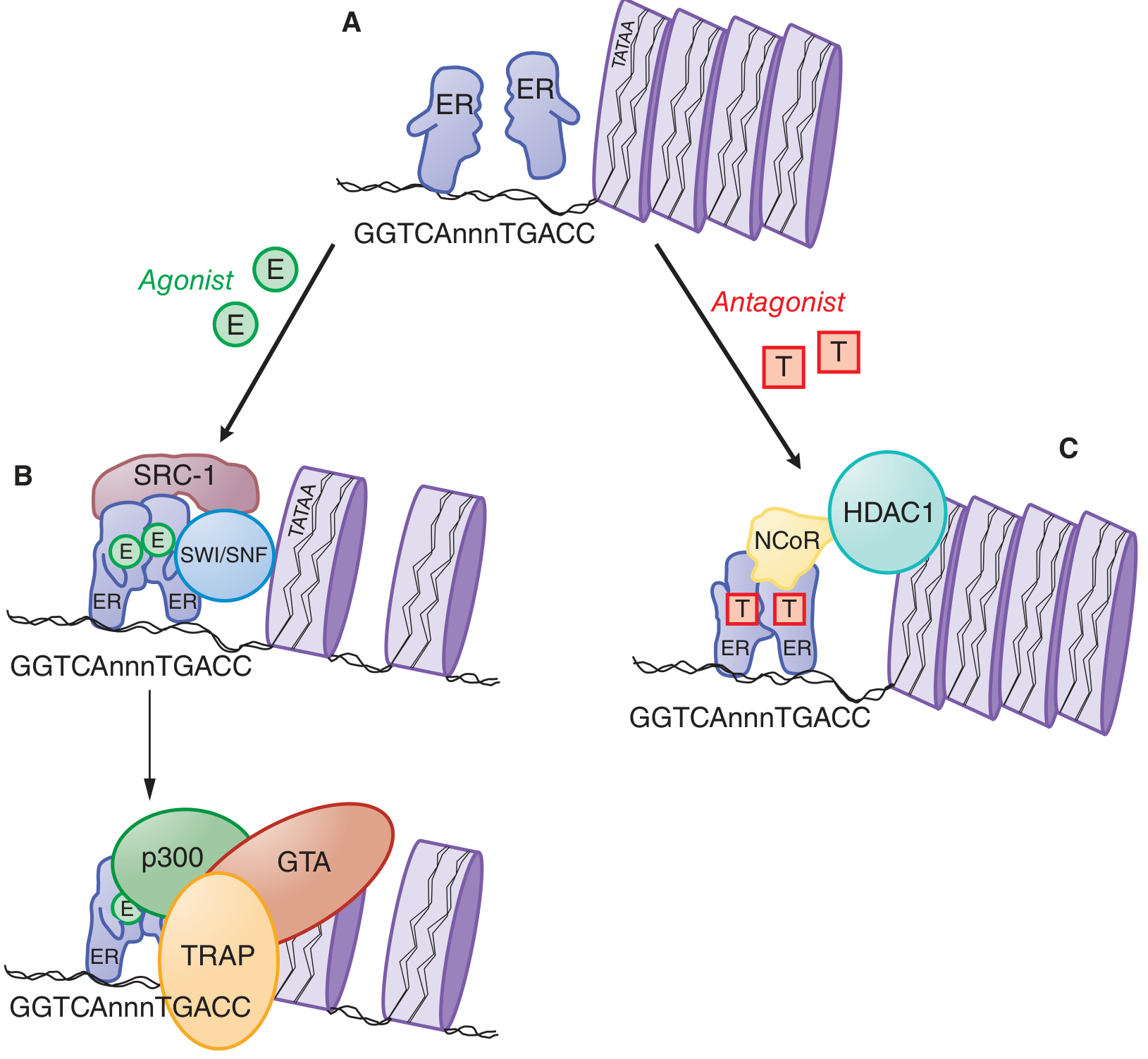
Figure: (A) Unliganded ER monomers. (B) Agonist (E2) binding causes dimerization, ERE binding, and coactivator recruitment (SRC-1, SWI/SNF, p300, TRAP) leading to gene transcription. (C) Antagonist (T = tamoxifen) produces a different ER conformation that recruits corepressors (NCoR, HDAC1) and silences transcription.
Non-genomic (Rapid) Signaling
- Membrane-associated ERα and GPER (GPR30, a G protein-coupled receptor) mediate rapid effects
- Crosstalk with EGF/IGF-1 pathways via MAPK and PI3K-Akt → phosphorylation of ERα at serine 118 causes ligand-independent activation
Receptor Isoforms
- ERα: Predominant in uterus, vagina, ovaries, mammary gland, hypothalamus, vascular endothelium
- ERβ: Predominant in prostate, ovaries, lung, bone, brain
- Both can form homodimers or heterodimers; ERβ can inhibit ERα-mediated transcription when co-expressed
4. Pharmacological Preparations & Routes
| Preparation | Route | Examples |
|---|---|---|
| Oral | Tablets | Micronized estradiol, conjugated equine estrogens (CEE), ethinyl estradiol, estropipate |
| Transdermal | Patch (1-2x/week) | Estradiol patches - avoids first-pass hepatic metabolism |
| Topical | Gel, emulsion (daily) | Estradiol gel (arm), emulsion (thigh/calf) |
| Intramuscular | Oil-based injection | Estradiol valerate, estradiol cypionate (every 1-4 weeks) |
| Vaginal | Cream, ring, tablet | Estradiol cream/ring, conjugated estrogen cream |
| Intravenous/IM | Injection | Conjugated estrogens (acute use) |
Key note: Ethinyl substitution at C17 (ethinyl estradiol) greatly increases oral potency by blocking first-pass hepatic metabolism - making it much more potent than conjugated estrogens orally. Transdermal route bypasses hepatic first-pass, minimizing effects on hepatic protein synthesis and lipids.
5. Therapeutic Uses
A. Hormonal Contraception
Ethinyl estradiol (combined with a progestin) suppresses LH/FSH surges, preventing ovulation. Available as combined oral contraceptive pills (COCPs), patches, and vaginal rings.
B. Menopausal Hormone Therapy (MHT)
- Relieves hot flashes, urogenital atrophy, mood changes
- Prevents postmenopausal osteoporosis
- Women with intact uterus must have a progestin added (to prevent endometrial hyperplasia)
- Preferred: Lowest effective dose for shortest duration
C. Induction of Sexual Maturation
Used in Turner syndrome and other causes of primary hypogonadism to induce puberty.
D. Osteoporosis Prevention
Estrogens maintain bone density by inhibiting osteoclast activity.
E. Genitourinary Syndrome of Menopause
Low-dose vaginal estrogens for vaginal atrophy, dryness, dyspareunia.
F. Palliative Cancer Treatment
High-dose estrogens used in some hormone-responsive breast and prostate cancers.
6. Estrogen Agonists/Antagonists: SERMs and Antiestrogens
These are drugs that modulate estrogen receptors in a tissue-selective manner.
Selective Estrogen Receptor Modulators (SERMs)
They produce different ER conformations that recruit different coactivators/corepressors depending on the tissue:
| Drug | Agonist at | Antagonist at | Main Use |
|---|---|---|---|
| Tamoxifen | Bone, liver (lipids) | Breast | Breast cancer treatment/prevention |
| Raloxifene | Bone | Breast, uterus | Osteoporosis + breast cancer prevention |
| Toremifene | Bone | Breast | Breast cancer (similar to tamoxifen) |
| Clomiphene | Hypothalamus/pituitary (antagonism → increases GnRH/FSH/LH) | - | Ovulation induction (infertility) |
Pure Antiestrogens
- Fulvestrant: 7α-alkylamide derivative of estradiol; pure ER antagonist in all tissues; causes receptor downregulation. Used for breast cancer after tamoxifen failure.
7. Estrogen Synthesis Inhibitors (Aromatase Inhibitors)
These block conversion of androgens to estrogens by inhibiting aromatase (CYP19):
| Type | Drug | Mechanism | Use |
|---|---|---|---|
| Steroidal (Type I) | Exemestane | Suicide (irreversible) inhibitor | Breast cancer |
| Non-steroidal (Type II) | Anastrozole, Letrozole | Reversible (heme binding) | Breast cancer |
Aromatase inhibitors are superior to tamoxifen in postmenopausal adjuvant breast cancer treatment. They do NOT increase uterine cancer or VTE risk (unlike tamoxifen) but do cause bone loss and hot flashes.
8. Physiological Effects of Estrogens
| System | Effect |
|---|---|
| Reproductive tract | Endometrial proliferation, cervical mucus thinning, vaginal epithelium thickening |
| Breast | Ductal development, promotes growth |
| Bone | Inhibits osteoclast activity; maintains bone density |
| Cardiovascular | Improves lipid profile (↑ HDL, ↓ LDL); vasodilation |
| Coagulation | ↑ Factors II, VII, IX, X, XII; ↓ Protein C, S, antithrombin III; ↑ fibrinolysis |
| CNS | Thermoregulation, mood, neuroprotection |
| Liver | Increases production of SHBG, TBG, coagulation factors, angiotensinogen |
| Metabolism | Affects carbohydrate and fat metabolism; slight increase in TG with oral estrogens |
9. Adverse Effects & Contraindications
| Adverse Effect | Notes |
|---|---|
| Venous thromboembolism (VTE) | Due to procoagulant effects; higher risk with oral vs. transdermal |
| Breast cancer | Risk increased with prolonged combined HRT (estrogen + progestin) |
| Endometrial cancer | Risk with unopposed estrogen in women with intact uterus |
| Cardiovascular events | Timing hypothesis: protective if started early in menopause; harmful if started >10 years post-menopause |
| Nausea, bloating | Common at initiation |
| Hypertension | Via ↑ angiotensinogen |
| Gallbladder disease | Increased risk with oral estrogens |
Absolute contraindications: Estrogen-dependent cancers (breast, endometrial), active thromboembolism, unexplained vaginal bleeding, liver disease, pregnancy.
10. Summary: Drug Classes at a Glance
ESTROGEN DRUGS
├── Estrogen Agonists (Replacement/Contraception)
│ ├── 17β-Estradiol (natural, patches, gels, IM)
│ ├── Ethinyl estradiol (oral contraceptives)
│ └── Conjugated equine estrogens (CEE - Premarin)
│
├── SERMs (Selective Estrogen Receptor Modulators)
│ ├── Tamoxifen (breast CA treatment)
│ ├── Raloxifene (osteoporosis + breast CA prevention)
│ ├── Toremifene (breast CA)
│ └── Clomiphene (ovulation induction)
│
├── Pure Antiestrogens
│ └── Fulvestrant (breast CA after tamoxifen failure)
│
└── Estrogen Synthesis Inhibitors (Aromatase Inhibitors)
├── Exemestane (steroidal, irreversible)
├── Anastrozole (non-steroidal, reversible)
└── Letrozole (non-steroidal, reversible)
Source: Goodman & Gilman's The Pharmacological Basis of Therapeutics, Chapter 48 (Estrogens and Progestins)
Estrogen
Asking for Preferences
Estrogen drugs
The previous response already covered estrogen drugs in detail. Here is a clean, well-organized summary of everything covered:
Estrogen Drugs - Complete Overview
1. Endogenous Estrogens (Natural)
| Estrogen | Potency | Main Source |
|---|---|---|
| 17β-Estradiol (E2) | Most potent | Ovaries (premenopausal) |
| Estrone (E1) | Intermediate | Peripheral conversion (postmenopausal) |
| Estriol (E3) | Weakest | Fetoplacental unit (pregnancy) |
All share a phenolic A ring with -OH at C3. Biosynthesis requires aromatase (CYP19) to convert androgens to estrogens.
2. Mechanism of Action
Genomic Pathway (Primary)
- Estrogen binds ERα or ERβ in the nucleus
- Receptor dimerizes → binds Estrogen Response Elements (EREs) on DNA
- Recruits coactivators (SRC-1, SWI/SNF, p300) → gene transcription
Non-Genomic (Rapid)
- Membrane-associated ER and GPER (GPR30) → fast signaling via MAPK, PI3K-Akt
Receptor Distribution
- ERα: Uterus, vagina, ovaries, breast, hypothalamus, vascular endothelium
- ERβ: Prostate, ovaries, lung, bone, brain
3. Pharmacological Preparations
| Preparation | Route | Key Examples |
|---|---|---|
| Micronized estradiol | Oral | Estrace |
| Conjugated equine estrogens | Oral / IV / IM | Premarin (CEE) |
| Ethinyl estradiol | Oral | Combined OCP (most potent oral form) |
| Estropipate | Oral | Ogen |
| Estradiol patch | Transdermal | Vivelle, Climara (1-2x/week) |
| Estradiol gel/emulsion | Topical | Estrogel, Estrasorb |
| Estradiol valerate / cypionate | IM injection | Given every 1-4 weeks |
| Estradiol cream / ring / tablet | Vaginal | Vagifem, Estring |
Ethinyl estradiol has a C17 ethinyl group that blocks first-pass hepatic metabolism, making it far more potent orally than conjugated estrogens. Transdermal routes avoid first-pass and minimize hepatic effects (lipids, coagulation factors).
4. Therapeutic Uses
| Indication | Drug/Approach |
|---|---|
| Combined oral contraception | Ethinyl estradiol + progestin |
| Menopausal HRT (hot flashes, atrophy) | Estradiol or CEE ± progestin |
| Osteoporosis prevention | Estradiol (maintains bone density) |
| Genitourinary syndrome of menopause | Low-dose vaginal estradiol |
| Primary hypogonadism / Turner syndrome | Estradiol (induces puberty) |
| Hormone-responsive cancers (palliative) | High-dose estrogens |
5. SERMs - Selective Estrogen Receptor Modulators
Tissue-selective agonist/antagonist activity based on differential coactivator recruitment:
| Drug | Agonist at | Antagonist at | Use |
|---|---|---|---|
| Tamoxifen | Bone, liver | Breast | Breast cancer treatment/prevention |
| Raloxifene | Bone | Breast, uterus | Osteoporosis + breast cancer prevention |
| Toremifene | Bone | Breast | Breast cancer |
| Clomiphene | Hypothalamus (blocks feedback → ↑FSH/LH) | - | Ovulation induction (infertility) |
6. Pure Antiestrogens
| Drug | Mechanism | Use |
|---|---|---|
| Fulvestrant | Pure ER antagonist + receptor downregulation | Breast cancer after tamoxifen failure |
7. Aromatase Inhibitors (Estrogen Synthesis Inhibitors)
Block CYP19 (aromatase), stopping androgen → estrogen conversion:
| Type | Drug | Mechanism | Use |
|---|---|---|---|
| Steroidal (Type I) | Exemestane | Irreversible suicide inhibitor | Breast cancer |
| Non-steroidal (Type II) | Anastrozole, Letrozole | Reversible heme binding | Breast cancer |
Superior to tamoxifen in postmenopausal adjuvant breast cancer. No uterine cancer or VTE risk (unlike tamoxifen), but cause bone loss and hot flashes.
8. Physiological Effects
| System | Effect |
|---|---|
| Reproductive tract | Endometrial proliferation, cervical mucus thinning, vaginal epithelium thickening |
| Breast | Ductal development |
| Bone | Inhibits osteoclasts → maintains bone density |
| Cardiovascular | ↑ HDL, ↓ LDL; vasodilation |
| Coagulation | ↑ Factors II, VII, IX, X, XII; ↓ Protein C, S, antithrombin III |
| Liver | ↑ SHBG, TBG, angiotensinogen, coagulation proteins |
| CNS | Thermoregulation, mood, neuroprotection |
9. Adverse Effects & Contraindications
| Adverse Effect | Mechanism / Note |
|---|---|
| VTE (DVT/PE) | Procoagulant effect; oral > transdermal |
| Breast cancer | Long-term combined HRT (estrogen + progestin) |
| Endometrial cancer | Unopposed estrogen in women with intact uterus |
| Cardiovascular risk | Harmful if started >10 yrs post-menopause |
| Nausea, bloating | Common at initiation |
| Hypertension | ↑ angiotensinogen |
| Gallbladder disease | Increased with oral estrogens |
Absolute contraindications: Estrogen-dependent cancers, active VTE, unexplained vaginal bleeding, active liver disease, pregnancy.
10. Quick Summary Diagram
ESTROGEN DRUGS
├── Agonists (Replacement / Contraception)
│ ├── 17β-Estradiol (patches, gels, IM, vaginal)
│ ├── Ethinyl estradiol (oral contraceptives)
│ └── Conjugated equine estrogens - CEE (Premarin)
│
├── SERMs
│ ├── Tamoxifen → breast cancer Rx
│ ├── Raloxifene → osteoporosis + breast CA prevention
│ ├── Toremifene → breast cancer
│ └── Clomiphene → ovulation induction
│
├── Pure Antiestrogen
│ └── Fulvestrant → breast CA (post-tamoxifen)
│
└── Aromatase Inhibitors (stop estrogen synthesis)
├── Exemestane (irreversible)
├── Anastrozole (reversible)
└── Letrozole (reversible)
Source: Goodman & Gilman's The Pharmacological Basis of Therapeutics, Chapter 48
Progesterone from lippincot
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the content needed from Lippincott. Here is the complete, well-organized answer:
Progesterone & Progestogens - Lippincott Illustrated Reviews: Pharmacology
1. Overview of Progestogens
The term progestogens includes both:
- Progesterone - the naturally occurring hormone (secreted by corpus luteum)
- Progestins - synthetic compounds with progesterone-like activity (more stable, better oral bioavailability)
2. Mechanism of Action
Progestogens act like all steroid hormones - they diffuse across the cell membrane and bind to specific nuclear progesterone receptors. The activated hormone-receptor complex interacts with nuclear chromatin to initiate specific RNA synthesis, producing proteins that mediate physiological effects.
Key physiological actions of progesterone:
| Phase | Action |
|---|---|
| Luteal phase | Promotes secretory transformation of endometrium to accommodate embryo implantation |
| During pregnancy | Maintains endometrium favorably; reduces uterine contractions (prevents preterm labor) |
| Negative feedback | High progesterone from corpus luteum inhibits gonadotropins (LH, FSH) → prevents further ovulation |
| Menstruation trigger | Corpus luteum regresses → progesterone falls abruptly → menstruation begins |
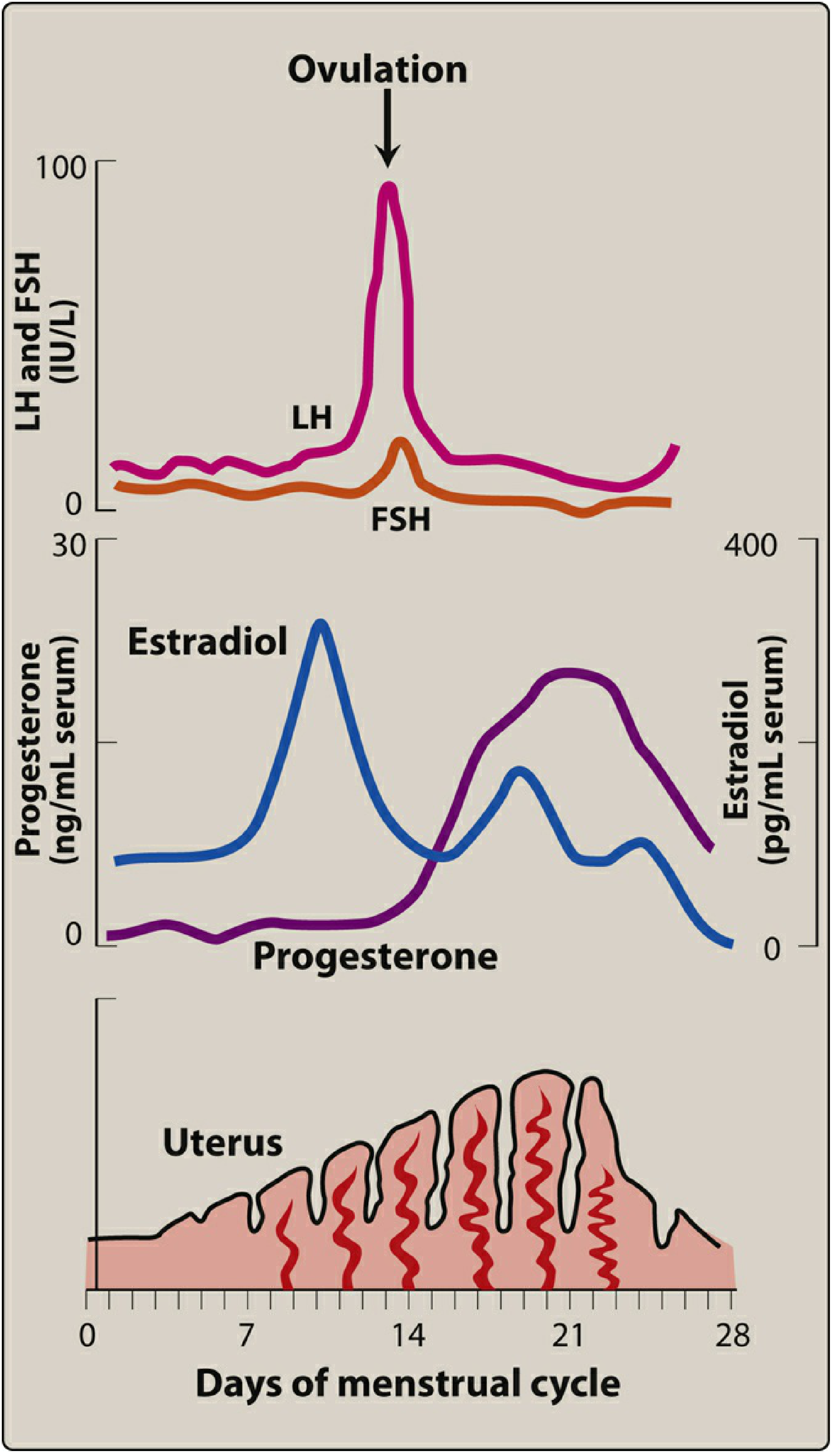
Figure 25.6 (Lippincott): The menstrual cycle - progesterone rises sharply after ovulation (day 14), peaks around day 21 in the luteal phase, then falls to trigger menstruation.
3. Synthetic Progestins (Drugs Used Clinically)
Natural progesterone is NOT used as a contraceptive because of its rapid first-pass hepatic metabolism and low oral bioavailability. Synthetic progestins are more stable.
Progestins for Contraception
| Drug | Route / Form | Brand |
|---|---|---|
| Levonorgestrel | Oral (emergency) | Plan B One-Step |
| Levonorgestrel | IUD | Mirena, Kyleena, Liletta, Skyla |
| Levonorgestrel | With EE - oral | Generic |
| Levonorgestrel | With EE - transdermal | Twirla |
| Etonogestrel | Subdermal implant | Nexplanon |
| Etonogestrel | With EE - vaginal ring | NuvaRing |
| Norethindrone | Oral (progestin-only pill) | Generic |
| Norethindrone acetate | With EE - oral | Loestrin |
| Drospirenone | Progestin-only pill | Slynd |
| Drospirenone | With EE - oral | Yasmin, Yaz |
| Norgestimate | With EE - oral | Ortho Tri-Cyclen, Sprintec |
| Desogestrel | In combination OCP | Generic |
| Dienogest | With estradiol valerate | Natazia |
| Norelgestromin | With EE - transdermal patch | Xulane |
| Medroxyprogesterone acetate | Injectable (IM/SC) | Depo-Provera |
Progestins for Hormone Therapy (HT)
| Drug | Route | Brand |
|---|---|---|
| Progesterone (micronized) | Oral | Prometrium |
| Medroxyprogesterone acetate | Oral | Provera |
| Medroxyprogesterone acetate | With CEE - oral | Prempro |
| Norethindrone acetate | With estradiol - oral | Activella |
| Norethindrone acetate | With estradiol - transdermal | CombiPatch |
| Levonorgestrel | With estradiol - transdermal | Climara Pro |
| Drospirenone | With estradiol - oral | Angeliq |
4. Therapeutic Uses
- Contraception - oral, injectable, transdermal, implant, IUD
- Menopausal hormone therapy (HT) - combined with estrogen to protect endometrium from unopposed estrogen-induced hyperplasia
- Control of heavy menstrual bleeding (menorrhagia) - levonorgestrel IUD especially effective
- Dysmenorrhea - reduce uterine contractions
- Endometriosis - suppress endometrial growth
- Infertility management - luteal phase support
5. Pharmacokinetics
| Drug | Key PK Feature |
|---|---|
| Progesterone (micronized, oral) | Short plasma half-life; metabolized in liver to pregnanediol → glucuronide/sulfate conjugates → excreted in urine |
| Medroxyprogesterone (oral) | Half-life 16-30 hours |
| Medroxyprogesterone (IM/SC) | Half-life ~40-50 days; provides contraception for ~3 months (Depo-Provera) |
| Other progestins | Half-lives 7-30 hours; allow once-daily dosing |
Synthetic progestins are less rapidly metabolized than natural progesterone, making them suitable for once-daily oral dosing.
6. Adverse Effects
| Adverse Effect | Notes |
|---|---|
| Headache | Common |
| Depression | Common |
| Weight gain | Common |
| Changes in libido | Common |
| Acne & hirsutism | Progestins derived from 19-nortestosterone (norethindrone, levonorgestrel) have androgenic activity due to structural similarity to testosterone |
| Hyperkalemia | Drospirenone (an analog of spironolactone) has anti-mineralocorticoid effects → ↑ serum K⁺; risk increases with ACE inhibitors or K⁺-sparing drugs |
Less androgenic progestins (norgestimate, drospirenone) are preferred in women with acne.
7. Progesterone Antagonist - Mifepristone (RU-486)
Mifepristone [mih-feh-PRIH-stone]
- Pure progesterone receptor antagonist
- Terminates pregnancy by blocking progesterone needed to maintain the endometrium
- Usually combined with misoprostol (prostaglandin analog) to induce uterine contractions
- Brand: Mifeprex
- Adverse effects: abdominal pain, uterine bleeding, risk of incomplete termination
8. Progesterone Agonist/Antagonist - Ulipristal
Ulipristal acetate [ue-li-PRIS-tal]
- A selective progesterone receptor modulator (acts as agonist/antagonist)
- Used as emergency contraception (up to 120 hours after unprotected intercourse)
- Brand: Ella
- Better tolerated than estrogen-progestin combination emergency contraceptives
9. Contraceptive Mechanisms (Summary)
In combination hormonal contraceptives:
- Estrogen → negative feedback → blunts FSH release → prevents follicle development
- Progestin → inhibits LH surge → prevents ovulation; also thickens cervical mucus to prevent sperm penetration
- Withdrawal of progestin (pill-free week) → withdrawal bleeding
10. Drug Interactions
| Interacting Drug | Effect |
|---|---|
| CYP3A4 inducers (rifampin, carbamazepine, phenytoin) | Reduce contraceptive efficacy - use alternate barrier method |
| Antibiotics (broad-spectrum) | Alter GI flora → reduce enterohepatic recycling of estrogen in combination pills → may reduce efficacy |
| ACE inhibitors / K⁺-sparing drugs | Combined with drospirenone → risk of hyperkalemia |
Source: Lippincott Illustrated Reviews: Pharmacology, Chapter 25 - Estrogens, Progestogens, and Contraceptives
Progesterone from lip Pinchot
"Lip Pinchot" is your autocorrect for Lippincott - the full answer was just provided above from Lippincott Illustrated Reviews: Pharmacology, Chapter 25.
Here's a quick recap of the key points:
Progesterone - Lippincott Summary
Mechanism
- Binds nuclear progesterone receptors → activates gene transcription
- Promotes secretory endometrium for implantation
- Inhibits LH/FSH (negative feedback) → prevents ovulation in luteal phase
- Maintains pregnancy + reduces uterine contractions
- Fall in progesterone → triggers menstruation
Key Drugs (Progestins)
| Drug | Use | Route |
|---|---|---|
| Progesterone micronized (Prometrium) | HRT | Oral |
| Medroxyprogesterone (Depo-Provera) | Contraception | IM injection (3 months) |
| Levonorgestrel (Mirena, Plan B) | Contraception | IUD / Oral |
| Norethindrone | Contraception | Oral |
| Drospirenone (Yaz) | Contraception | Oral |
| Etonogestrel (Nexplanon, NuvaRing) | Contraception | Implant / Vaginal ring |
| Mifepristone (Mifeprex) | Medical abortion | Oral (+ misoprostol) |
| Ulipristal (Ella) | Emergency contraception | Oral |
Adverse Effects
- Headache, depression, weight gain, libido changes
- Acne/hirsutism - 19-nortestosterone-derived progestins (norethindrone, levonorgestrel) have androgenic activity
- Hyperkalemia - drospirenone (spironolactone analog) - caution with ACE inhibitors
Pharmacokinetics
- Natural progesterone: rapid first-pass metabolism - NOT used for contraception
- Synthetic progestins: more stable, once-daily oral dosing
- Depo-Provera (IM): half-life ~40-50 days, lasts 3 months
Source: Lippincott Illustrated Reviews: Pharmacology, Chapter 25
Give me full answer
The full answer was already provided two responses ago. Here it is again in complete form, directly from Lippincott Illustrated Reviews: Pharmacology, Chapter 25:
Progesterone & Progestogens
Lippincott Illustrated Reviews: Pharmacology - Chapter 25
1. What Are Progestogens?
The term progestogens covers two categories:
- Progesterone - the natural hormone secreted by the corpus luteum
- Progestins - synthetic analogs with progesterone-like activity (more stable, better oral bioavailability)
Natural progesterone is NOT used as a contraceptive because of its rapid first-pass hepatic metabolism resulting in low bioavailability when taken orally.
2. Mechanism of Action
Progestogens act like all steroid hormones:
- Diffuse across the cell membrane
- Bind to specific nuclear progesterone receptors
- Activated hormone-receptor complex binds nuclear chromatin
- Initiates specific RNA synthesis → specific protein production → physiological effects
Physiological Actions of Progesterone
| Situation | Action |
|---|---|
| Luteal phase (days 15-28) | Promotes secretory endometrium to accommodate embryo implantation |
| Negative feedback | High levels from corpus luteum inhibit LH/FSH → prevents further ovulation |
| If conception occurs | Continues to maintain endometrium; reduces uterine contractions to preserve pregnancy |
| If no conception | Corpus luteum regresses → progesterone falls abruptly → menstruation begins |
Figure 25.6: The menstrual cycle. Progesterone rises sharply after ovulation (~day 14), peaks in the luteal phase (~day 21), then falls to trigger menstruation at day 28.
3. Classification of Progestogen Drugs
A. Natural Progesterone
| Drug | Brand | Route |
|---|---|---|
| Progesterone (micronized) | Prometrium | Oral |
| Progesterone | Various | Vaginal gel/suppository |
Micronized form has larger surface area for better absorption, but still undergoes significant first-pass metabolism.
B. Synthetic Progestins - For Contraception
Derived from two structural classes:
19-Nortestosterone derivatives (have some androgenic activity - can cause acne/hirsutism):
| Drug | Route / Delivery | Brand |
|---|---|---|
| Norethindrone | Oral (progestin-only pill) | Generic |
| Norethindrone acetate | With EE - oral | Loestrin |
| Norethindrone acetate | With estradiol - oral | Activella |
| Norethindrone acetate | With estradiol - transdermal | CombiPatch |
| Levonorgestrel | Oral (emergency contraception) | Plan B One-Step |
| Levonorgestrel | IUD | Mirena, Kyleena, Liletta, Skyla |
| Levonorgestrel | With EE - oral | Generic |
| Levonorgestrel | With EE - transdermal | Twirla |
| Levonorgestrel | With estradiol - transdermal | Climara Pro |
| Etonogestrel | Subdermal implant | Nexplanon |
| Etonogestrel | With EE - vaginal ring | NuvaRing |
| Norelgestromin | With EE - transdermal patch | Xulane |
Less androgenic / newer progestins (preferred in women with acne):
| Drug | Route / Delivery | Brand |
|---|---|---|
| Norgestimate | With EE - oral | Ortho Tri-Cyclen, Sprintec |
| Desogestrel | In combination OCP | Generic |
| Dienogest | With estradiol valerate - oral | Natazia |
| Drospirenone | Progestin-only pill | Slynd |
| Drospirenone | With EE - oral | Yasmin, Yaz |
| Drospirenone | With estradiol - oral (HT) | Angeliq |
Pregnane derivatives:
| Drug | Route / Delivery | Brand |
|---|---|---|
| Medroxyprogesterone acetate | Oral (HT) | Provera |
| Medroxyprogesterone acetate | IM injection | Depo-Provera |
| Medroxyprogesterone acetate | With CEE - oral (HT) | Prempro |
4. Therapeutic Uses
| Use | Drug(s) of Choice |
|---|---|
| Oral contraception | Norethindrone, levonorgestrel, norgestimate, drospirenone + EE combinations |
| Long-acting injectable contraception | Medroxyprogesterone acetate IM (Depo-Provera) - 3 months |
| Subdermal implant contraception | Etonogestrel (Nexplanon) - up to 3 years |
| Intrauterine contraception | Levonorgestrel IUD (Mirena etc.) - 3-8 years |
| Emergency contraception | Levonorgestrel (Plan B), ulipristal (Ella) |
| Menopausal hormone therapy (HT) | Progesterone (Prometrium), MPA (Prempro), norethindrone acetate - added to estrogen to protect endometrium |
| Heavy menstrual bleeding | Levonorgestrel IUD; MPA |
| Dysmenorrhea | Combined OCP or progestin-only |
| Endometriosis | Progestins suppress endometrial growth |
| Infertility / luteal phase support | Progesterone vaginal gel |
5. Pharmacokinetics
| Drug | Half-life | Notes |
|---|---|---|
| Progesterone (micronized, oral) | Short | Extensive first-pass metabolism → pregnanediol → glucuronide/sulfate conjugates → excreted in urine |
| Medroxyprogesterone (oral) | 16-30 hours | Once daily dosing |
| Medroxyprogesterone (IM/SC - Depo-Provera) | ~40-50 days | Provides contraception for ~3 months per injection |
| Other progestins | 7-30 hours | Once-daily oral dosing |
6. Contraceptive Mechanism of Action (How Progestins Prevent Pregnancy)
In combination hormonal contraceptives (pill, patch, ring):
- Estrogen → negative feedback → blunts FSH release from pituitary → prevents follicle development
- Progestin → inhibits LH surge → prevents ovulation
- Progestin also thickens cervical mucus → blocks sperm from reaching the egg
- Withdrawal of progestin (during the pill-free / patch-free week) → withdrawal bleeding (not true menstruation)
In progestin-only methods (mini-pill, implant, injection, IUD):
- Primary mechanism: thickening of cervical mucus + thinning of endometrium
- Ovulation may still occur
7. Adverse Effects
| Adverse Effect | Details |
|---|---|
| Headache | Common |
| Depression | Common - especially with 19-nortestosterone derivatives |
| Weight gain | Common |
| Changes in libido | Common |
| Acne & hirsutism | Due to androgenic activity of 19-nortestosterone progestins (norethindrone, levonorgestrel) - structural similarity to testosterone |
| Hyperkalemia | Drospirenone only - spironolactone analog with anti-mineralocorticoid activity → raises serum K⁺; risk ↑ with ACE inhibitors, ARBs, K⁺-sparing diuretics |
| Breakthrough bleeding | Especially with progestin-only pills and new users |
Tip: For women with acne, prefer norgestimate or drospirenone - less androgenic than norethindrone or levonorgestrel.
8. Progesterone Antagonist - Mifepristone (RU-486)
Mifepristone [mih-feh-PRIH-stone] | Brand: Mifeprex
- Pure progesterone receptor antagonist
- Blocks the progesterone required to maintain the endometrium
- Results in termination of early pregnancy
- Almost always combined with misoprostol (a prostaglandin E1 analog) to:
- Induce uterine contractions
- Complete evacuation of uterine contents
Adverse effects:
- Abdominal/uterine cramping
- Uterine bleeding (expected)
- Risk of incomplete termination of pregnancy
9. Progesterone Agonist/Antagonist - Ulipristal
Ulipristal acetate [ue-li-PRIS-tal] | Brand: Ella
- Selective progesterone receptor modulator (partial agonist/antagonist)
- Mechanism: delays or inhibits ovulation; may also affect endometrial receptivity
- Used as emergency contraception - effective up to 120 hours (5 days) after unprotected intercourse
- Better tolerated than levonorgestrel + estrogen combination regimens
10. Drug Interactions with Progestin-Containing Contraceptives
| Interacting Drug | Mechanism | Clinical Action |
|---|---|---|
| Rifampin, carbamazepine, phenytoin | CYP3A4 inducers → increased progestin/estrogen metabolism | Avoid or add barrier method |
| Broad-spectrum antibiotics | Alter GI flora → reduce enterohepatic recycling of estrogen in combined pills | Warn patients; consider backup contraception |
| ACE inhibitors, ARBs, K⁺-sparing diuretics | Combined with drospirenone → additive hyperkalemia risk | Monitor serum potassium |
11. Contraindications
- Active or history of thromboembolic disease
- Estrogen-dependent cancers (for combined products)
- Liver disease
- Pregnancy
- Undiagnosed abnormal vaginal bleeding
- Women >35 years who smoke - avoid estrogen-containing contraceptives (progestin-only preferred)
Summary Diagram
PROGESTOGEN DRUGS (Lippincott Ch. 25)
│
├── NATURAL
│ └── Progesterone (Prometrium, vaginal gel)
│ - Short half-life, first-pass metabolism
│ - Used for HRT & luteal phase support
│
├── SYNTHETIC PROGESTINS
│ ├── 19-Nortestosterone derivatives (androgenic)
│ │ ├── Norethindrone / Norethindrone acetate
│ │ ├── Levonorgestrel (Plan B, Mirena IUD, Twirla)
│ │ ├── Etonogestrel (Nexplanon, NuvaRing)
│ │ └── Norelgestromin (Xulane patch)
│ │
│ ├── Less androgenic
│ │ ├── Norgestimate (Ortho Tri-Cyclen)
│ │ ├── Desogestrel
│ │ ├── Dienogest (Natazia)
│ │ └── Drospirenone (Yaz, Yasmin) ← anti-mineralocorticoid
│ │
│ └── Pregnane derivatives
│ └── Medroxyprogesterone (Provera, Depo-Provera)
│ - Depo: 3-month injection
│
├── PROGESTERONE ANTAGONIST
│ └── Mifepristone (Mifeprex / RU-486)
│ - Medical abortion (+ misoprostol)
│
└── PROGESTERONE AGONIST/ANTAGONIST
└── Ulipristal (Ella)
- Emergency contraception (up to 120 hrs)
Source: Lippincott Illustrated Reviews: Pharmacology, Chapter 25 - Estrogens, Progestogens, and Contraceptives
Parkinsonism pharmacology
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I have all the content I need. Now let me compile the full, complete answer.
Parkinsonism Pharmacology
Lippincott Illustrated Reviews: Pharmacology - Chapter 15
1. What is Parkinsonism?
Parkinsonism is a progressive neurological disorder of muscle movement characterized by:
- Tremors (resting tremor - "pill-rolling")
- Muscular rigidity
- Bradykinesia (slowness of movement)
- Postural and gait abnormalities
Most cases occur in people over 65 years of age.
2. Pathophysiology
The Core Problem
Destruction of dopaminergic neurons in the substantia nigra → reduced dopamine in the neostriatum (basal ganglia)
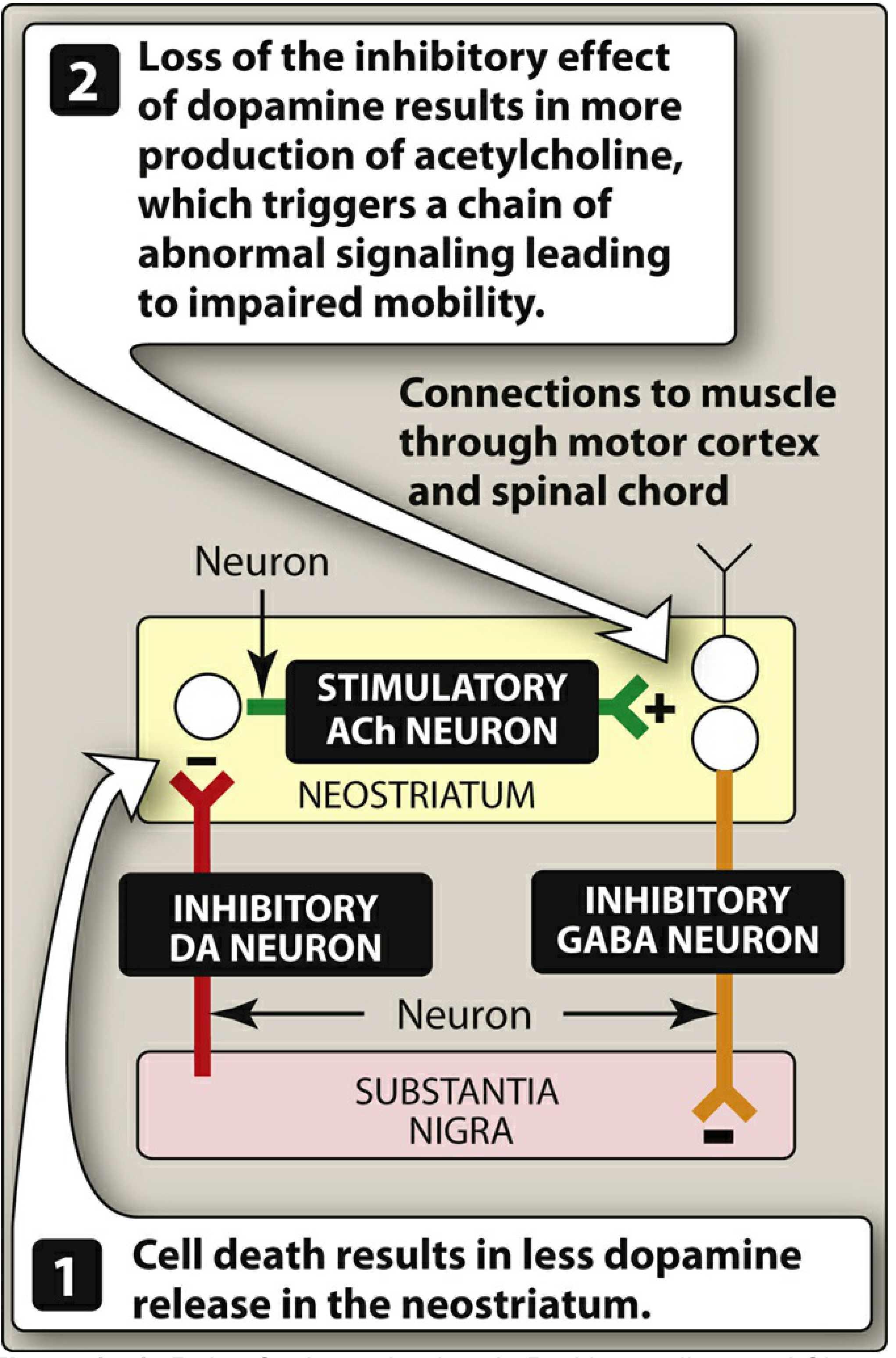
Figure 15.4 (Lippincott): (1) Cell death in substantia nigra → less dopamine released in neostriatum. (2) Loss of dopamine's inhibitory effect → overproduction of ACh by stimulatory cholinergic neurons → abnormal signaling → impaired mobility.
Normal Circuit
- Substantia nigra → Neostriatum: dopaminergic neurons (inhibitory - suppresses ACh)
- Neostriatum → Substantia nigra: GABAergic neurons (inhibitory)
- This mutual inhibition maintains balanced motor control
In Parkinson Disease
- Substantia nigra cells die → dopamine ↓ in neostriatum
- Without dopamine's inhibition → ACh neurons become overactive
- Result: dopamine/ACh imbalance → loss of muscle movement control
Secondary (Drug-Induced) Parkinsonism
Drugs that block dopamine receptors - phenothiazines, haloperidol, and other antipsychotics - produce pseudoparkinsonism. All dopamine receptor blockers carry some risk; use with extreme caution or avoid in PD patients.
3. Treatment Strategy
Two approaches to restore DA/ACh balance:
- Increase dopaminergic activity (main approach) - using levodopa, dopamine agonists, MAO-B inhibitors, COMT inhibitors, amantadine
- Decrease cholinergic activity - using anticholinergics
Current drugs only offer symptomatic relief - they do NOT arrest or reverse neuronal degeneration.
4. Drug Classes
CLASS 1: Levodopa + Carbidopa (FIRST-LINE)
Levodopa [lee-voe-DOE-pa] | Brand: Sinemet (with carbidopa)
Why Levodopa, not Dopamine?
Dopamine does NOT cross the blood-brain barrier (BBB). Levodopa is its metabolic precursor - it is actively transported across the BBB and converted to dopamine by residual neurons in the substantia nigra.
Why Add Carbidopa?
Without carbidopa, most levodopa is decarboxylated to dopamine peripherally before reaching the brain:
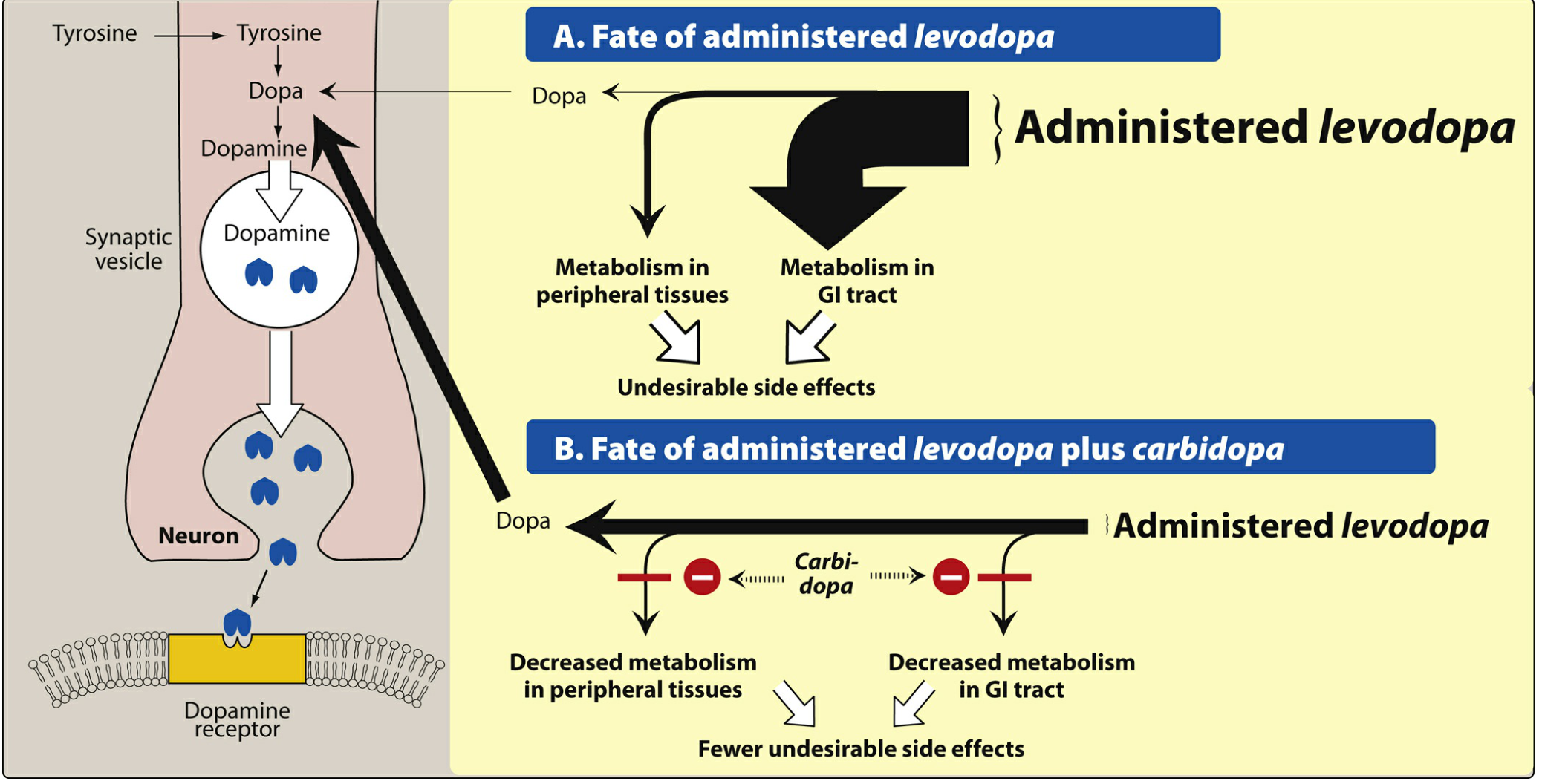
Figure 15.5 (Lippincott): Carbidopa inhibits peripheral dopa decarboxylase → prevents peripheral conversion of levodopa → more levodopa reaches the CNS → more brain dopamine + fewer peripheral side effects.
Carbidopa benefits:
- Reduces levodopa dose by 4-5 fold
- Reduces nausea, vomiting, cardiac arrhythmias, hypotension (from peripheral dopamine)
- Does NOT cross BBB itself - only acts peripherally
Pharmacokinetics
- Absorbed rapidly from small intestine (best on empty stomach - food delays/reduces absorption)
- Short half-life: 1-2 hours → plasma fluctuations → motor fluctuations
- Motor fluctuations include "wearing off" (end-of-dose) and "on-off" phenomenon
Adverse Effects
| Adverse Effect | Mechanism |
|---|---|
| Nausea, vomiting | Peripheral dopamine stimulating CTZ |
| Cardiac arrhythmias | Peripheral dopamine on heart |
| Orthostatic hypotension | Peripheral dopaminergic vasodilation |
| Dyskinesias (involuntary movements) | Excess dopamine; common after long-term use |
| "On-off" phenomenon | Unpredictable oscillation between mobility and immobility |
| Wearing off | Declining response before next dose |
| Hallucinations, psychosis | Central dopamine excess in non-motor areas |
Drug Interactions
- Pyridoxine (Vit B6): accelerates peripheral levodopa metabolism → reduces CNS availability (less relevant when carbidopa is co-administered)
- MAOIs (non-selective): risk of hypertensive crisis - contraindicated
- Antipsychotics: block dopamine receptors - antagonize levodopa
- High-protein diet: amino acids compete for intestinal absorption and BBB transport
Clinical Note
- Effective for ~3-5 years; then motor fluctuations develop as neurons continue to die
- In early disease: ~20% residual substantia nigra neurons still convert levodopa to dopamine adequately
- Withdrawal must be gradual (abrupt withdrawal → neuroleptic malignant-like syndrome)
CLASS 2: Dopamine Agonists
These directly stimulate dopamine receptors - they do NOT require conversion and have longer duration of action than levodopa.
| Drug | Brand | Route |
|---|---|---|
| Pramipexole [pra-mi-PEX-ole] | Mirapex | Oral |
| Ropinirole [roe-PIN-i-role] | Requip | Oral |
| Rotigotine | Neupro | Transdermal patch |
| Bromocriptine [broe-moe-KRIP-teen] | Parlodel | Oral |
| Apomorphine [ay-poe-MOR-feen] | Apokyn, Kynmobi | SC injection / sublingual |
Mechanism
Direct agonists at D2 (and D3) dopamine receptors in the striatum.
Therapeutic Use
- Used as monotherapy in early PD or as adjuncts to levodopa in advanced PD
- Allow reduction of levodopa dose and smooth out motor fluctuations
- Apomorphine: used as rescue therapy for acute "off" episodes
Adverse Effects
- Nausea, vomiting, orthostatic hypotension (like levodopa, but often less severe)
- Hallucinations, confusion (more common than with levodopa, especially in elderly)
- Impulse control disorders: compulsive gambling, hypersexuality, binge eating (especially pramipexole, ropinirole)
- Somnolence (sudden "sleep attacks" while driving - important warning)
- Bromocriptine: ergot-derived - can cause fibrotic reactions (pleuropulmonary, retroperitoneal)
CLASS 3: MAO-B Inhibitors
Block monoamine oxidase type B → reduce dopamine breakdown → increase dopamine in striatum.
| Drug | Brand | Key Features |
|---|---|---|
| Selegiline (Deprenyl) | Eldepryl, Zelapar | Irreversible MAO-B inhibitor; metabolized to methamphetamine + amphetamine → insomnia if taken after midday |
| Rasagiline | Azilect | Irreversible MAO-B inhibitor; 5× more potent than selegiline; NOT metabolized to amphetamine |
| Safinamide | Xadago | Reversible MAO-B inhibitor; adjunct to levodopa-carbidopa |
Selectivity
- At recommended doses: selective for MAO-B only → safe, no tyramine interaction ("cheese effect")
- At high doses: lose selectivity → inhibit MAO-A → risk of hypertensive crisis with tyramine-containing foods
Use
- As adjuncts to levodopa to enhance and prolong its effect; allow levodopa dose reduction
- Selegiline may also have neuroprotective properties (debated)
Adverse Effects
- Nausea, headache, confusion
- Insomnia (selegiline - from amphetamine metabolites - do not give after midday)
- Serotonin syndrome if combined with SSRIs, SNRIs, TCAs, meperidine - avoid concurrent use
CLASS 4: COMT Inhibitors
When carbidopa blocks peripheral dopa decarboxylase, levodopa is instead metabolized by COMT to 3-O-methyldopa (3-OMD), which:
- Competes with levodopa for BBB transport
- Reduces CNS uptake of levodopa
COMT inhibitors block this pathway → more levodopa reaches the brain.
| Drug | Brand | Key Features |
|---|---|---|
| Entacapone | Comtan | Peripheral COMT inhibitor only; short-acting; given with each levodopa dose |
| Opicapone | Ongentys | Once-daily peripheral COMT inhibitor |
| Tolcapone | Tasmar | Peripheral + central COMT inhibition; most potent, but hepatotoxic - reserved for refractory cases; requires LFT monitoring |
Stalevo = levodopa + carbidopa + entacapone (triple combination pill)
Adverse Effects
- Dyskinesias (from increased levodopa effect - may need to reduce levodopa dose)
- Diarrhea, nausea
- Urine discoloration (orange-brown) - harmless
- Tolcapone only: hepatotoxicity (fatal cases reported) - monitor LFTs
CLASS 5: Adenosine A2A Receptor Antagonist
| Drug | Brand | Mechanism |
|---|---|---|
| Istradefylline | Nourianz | Blocks adenosine A2A receptors in striatum → enhances dopaminergic signaling |
- Adjunct to levodopa-carbidopa for "off" episodes
- Adverse effects: dyskinesia, dizziness, nausea, insomnia
CLASS 6: Anticholinergics (for Tremor)
Block muscarinic ACh receptors → reduce the relative excess of cholinergic activity in the striatum.
| Drug | Brand |
|---|---|
| Trihexyphenidyl [try-hex-ee-FEN-ih-dill] | Generic |
| Benztropine [BENZ-troe-peen] | Cogentin |
Use
- Most useful for controlling tremor and rigidity
- Less effective for bradykinesia and postural instability
- Useful for drug-induced (pseudoparkinsonism) caused by antipsychotics
Adverse Effects (Anticholinergic = "Dry" effects)
- Dry mouth, constipation, urinary retention
- Blurred vision (cycloplegia)
- Tachycardia
- Confusion, memory impairment (especially in elderly - use with caution)
- Contraindicated in glaucoma, BPH
CLASS 7: Amantadine
Amantadine [a-MAN-ta-deen] | Brand: Gocovri
Mechanism (Multiple)
- Increases presynaptic dopamine release
- Inhibits dopamine reuptake
- Weak NMDA glutamate receptor antagonist → reduces dyskinesias
- Some anticholinergic activity
Use
- Mild early PD as monotherapy
- Adjunct to levodopa to smooth motor fluctuations
- Treatment of levodopa-induced dyskinesias (extended-release form - Gocovri)
Adverse Effects
- Livedo reticularis (mottled skin discoloration - characteristic side effect)
- Ankle edema
- Confusion, hallucinations
- Insomnia
5. PD Psychosis Management
A major challenge: most PD drugs increase dopamine → can cause hallucinations and psychosis. Yet treating psychosis with dopamine blockers worsens motor symptoms.
Solution:
- Pimavanserin - serotonin 5-HT2A inverse agonist (no dopamine blockade) → treats PD psychosis without worsening motor function
- Antipsychotics with very weak dopamine antagonism (e.g., quetiapine, clozapine) may also be used
6. Complete Drug List (Lippincott Ch. 15)
PARKINSON DISEASE DRUGS
│
├── LEVODOPA COMBINATIONS (First-line)
│ ├── Levodopa + Carbidopa (Sinemet)
│ └── Levodopa + Carbidopa + Entacapone (Stalevo)
│
├── DOPAMINE AGONISTS
│ ├── Pramipexole (Mirapex) - D2/D3 agonist
│ ├── Ropinirole (Requip) - D2/D3 agonist
│ ├── Rotigotine (Neupro) - transdermal patch
│ ├── Bromocriptine (Parlodel) - ergot-derived
│ └── Apomorphine (Apokyn) - rescue SC injection
│
├── MAO-B INHIBITORS
│ ├── Selegiline/Deprenyl (Eldepryl) - → amphetamine metabolites
│ ├── Rasagiline (Azilect) - 5× more potent; no amphetamine
│ └── Safinamide (Xadago) - reversible; adjunct to levodopa
│
├── COMT INHIBITORS
│ ├── Entacapone (Comtan) - peripheral only; per-dose
│ ├── Opicapone (Ongentys) - peripheral only; once-daily
│ └── Tolcapone (Tasmar) - central + peripheral; hepatotoxic
│
├── ADENOSINE A2A ANTAGONIST
│ └── Istradefylline (Nourianz) - adjunct for "off" episodes
│
├── ANTICHOLINERGICS (for tremor/rigidity)
│ ├── Trihexyphenidyl
│ └── Benztropine (Cogentin)
│
└── AMANTADINE (Gocovri)
- Multiple mechanisms: ↑ DA release, blocks reuptake, NMDA antagonist
- Also treats levodopa-induced dyskinesias
7. Summary Table - Mechanisms at a Glance
| Drug Class | Mechanism | Key Drugs |
|---|---|---|
| Levodopa + Carbidopa | DA precursor + peripheral decarboxylase inhibitor | Sinemet, Stalevo |
| Dopamine agonists | Direct D2/D3 receptor stimulation | Pramipexole, Ropinirole, Apomorphine |
| MAO-B inhibitors | Block dopamine breakdown | Selegiline, Rasagiline, Safinamide |
| COMT inhibitors | Block levodopa peripheral metabolism | Entacapone, Tolcapone, Opicapone |
| A2A antagonist | Enhance dopaminergic signaling indirectly | Istradefylline |
| Anticholinergics | Reduce excess ACh activity | Benztropine, Trihexyphenidyl |
| Amantadine | ↑ DA release + NMDA block + anticholinergic | Gocovri |
Source: Lippincott Illustrated Reviews: Pharmacology, Chapter 15 - Drugs for Parkinson Disease and Alzheimer Disease
Parkinsonism
The complete pharmacology of Parkinsonism was covered in detail in the previous response. Here is the full answer again:
Parkinsonism Pharmacology
Lippincott Illustrated Reviews: Pharmacology - Chapter 15
1. Definition & Features
Parkinsonism is a progressive neurological disorder characterized by the classic tetrad:
- Tremor - resting "pill-rolling" tremor
- Rigidity - cogwheel or lead-pipe
- Bradykinesia - slowness of movement
- Postural instability - gait and balance abnormalities
Most common in people >65 years.
2. Pathophysiology
Core Mechanism
Destruction of dopaminergic neurons in the substantia nigra → ↓ dopamine in the neostriatum (basal ganglia)
Fig 15.4: (1) Cell death in substantia nigra → less dopamine in neostriatum. (2) Loss of dopamine's inhibitory effect → ACh neurons overactive → chain of abnormal signaling → impaired mobility.
Normal Circuit
| Pathway | Transmitter | Effect |
|---|---|---|
| Substantia nigra → Neostriatum | Dopamine (DA) | Inhibitory (suppresses ACh) |
| Neostriatum → Substantia nigra | GABA | Inhibitory |
In PD
- DA neurons die → DA ↓
- ACh neurons lose inhibition → ACh ↑ (relatively)
- DA/ACh imbalance → motor dysfunction
Secondary (Drug-Induced) Parkinsonism
Drugs blocking dopamine receptors (phenothiazines, haloperidol, antipsychotics) → pseudoparkinsonism. All DA receptor blockers carry this risk. Avoid or use with extreme caution in PD.
3. Treatment Strategy
| Approach | Goal |
|---|---|
| ↑ Dopaminergic activity | Replace/mimic dopamine (main approach) |
| ↓ Cholinergic activity | Reduce relative ACh excess |
All current drugs give symptomatic relief only - none arrest or reverse neuronal degeneration.
4. Drug Classes
🔵 CLASS 1: Levodopa + Carbidopa — FIRST-LINE
Levodopa | Brand: Sinemet (levodopa/carbidopa), Stalevo (levodopa/carbidopa/entacapone)
Why Levodopa?
Dopamine cannot cross the BBB. Levodopa (its precursor) is actively transported across the BBB → converted to dopamine by residual substantia nigra neurons.
Why Add Carbidopa?
Without carbidopa, levodopa is converted to dopamine peripherally → nausea, vomiting, arrhythmias, hypotension, and very little reaches the brain.
Fig 15.5: Carbidopa inhibits peripheral dopa decarboxylase → less peripheral dopamine → fewer peripheral side effects + 4-5× less levodopa needed.
Key PK Facts
- Absorbed from small intestine - best on empty stomach
- Half-life: 1-2 hours → plasma fluctuations → motor fluctuations
- Effective for 3-5 years, then declines as more neurons die
- Withdrawal must be gradual
Adverse Effects
| Effect | Notes |
|---|---|
| Nausea, vomiting | Peripheral DA at CTZ |
| Orthostatic hypotension | Peripheral DA vasodilation |
| Cardiac arrhythmias | Peripheral DA on heart |
| Dyskinesias | Involuntary movements; dose-related |
| "Wearing off" | Response fades before next dose |
| "On-off" phenomenon | Unpredictable fluctuations unrelated to plasma level |
| Hallucinations, psychosis | Central DA excess in non-motor areas |
Drug Interactions
- Non-selective MAOIs → hypertensive crisis (contraindicated)
- Pyridoxine (Vit B6) → accelerates peripheral metabolism (less relevant with carbidopa)
- Antipsychotics → block DA receptors, antagonize levodopa
- High-protein diet → amino acids compete for intestinal absorption and BBB transport
🟢 CLASS 2: Dopamine Agonists
Directly stimulate DA receptors - do not require metabolic conversion, longer acting than levodopa.
| Drug | Brand | Route |
|---|---|---|
| Pramipexole | Mirapex | Oral |
| Ropinirole | Requip | Oral |
| Rotigotine | Neupro | Transdermal patch |
| Bromocriptine | Parlodel | Oral (ergot-derived) |
| Apomorphine | Apokyn, Kynmobi | SC injection / sublingual |
Mechanism: Direct D2/D3 receptor agonists in striatum
Use: Monotherapy (early PD) or adjunct to levodopa (advanced PD); apomorphine = rescue for acute "off" episodes
Adverse Effects:
- Nausea, hypotension
- Hallucinations/confusion (more than levodopa, especially elderly)
- Impulse control disorders - compulsive gambling, hypersexuality, binge eating (pramipexole/ropinirole)
- Sudden sleep attacks - risk while driving
- Bromocriptine: ergot fibrotic reactions (pulmonary, retroperitoneal)
🟡 CLASS 3: MAO-B Inhibitors
Block monoamine oxidase type B → reduce dopamine breakdown → ↑ synaptic DA.
| Drug | Brand | Key Feature |
|---|---|---|
| Selegiline (Deprenyl) | Eldepryl, Zelapar | Metabolized to methamphetamine + amphetamine → insomnia (don't give after midday) |
| Rasagiline | Azilect | 5× more potent than selegiline; no amphetamine metabolites |
| Safinamide | Xadago | Reversible MAO-B inhibitor; adjunct to levodopa-carbidopa |
Selectivity: At normal doses = MAO-B selective (safe). At high doses = loses selectivity → inhibits MAO-A → hypertensive crisis risk
Adverse Effects:
- Nausea, headache, confusion
- Selegiline: insomnia (amphetamine metabolites)
- Serotonin syndrome with SSRIs, SNRIs, TCAs, meperidine → avoid combination
🟠 CLASS 4: COMT Inhibitors
When carbidopa blocks peripheral decarboxylase, levodopa is instead converted by COMT to 3-O-methyldopa (3-OMD) which competes with levodopa for BBB transport. COMT inhibitors block this → more levodopa enters the CNS.
| Drug | Brand | Key Feature |
|---|---|---|
| Entacapone | Comtan | Peripheral COMT only; short-acting; one tablet per levodopa dose |
| Opicapone | Ongentys | Peripheral COMT only; once-daily |
| Tolcapone | Tasmar | Peripheral + central COMT; most potent; hepatotoxic → monitor LFTs |
Stalevo = levodopa + carbidopa + entacapone (all-in-one pill)
Adverse Effects:
- Dyskinesias (↑ levodopa effect - may need dose reduction)
- Diarrhea
- Orange-brown urine discoloration (harmless)
- Tolcapone: fatal hepatotoxicity reported - reserved for refractory patients
🔴 CLASS 5: Adenosine A2A Receptor Antagonist
| Drug | Brand | Mechanism |
|---|---|---|
| Istradefylline | Nourianz | Blocks adenosine A2A receptors in striatum → enhances dopaminergic tone |
- Adjunct to levodopa-carbidopa for "off" episodes
- Adverse effects: dyskinesia, dizziness, nausea, insomnia
⚪ CLASS 6: Anticholinergics
Block muscarinic ACh receptors → reduce excess cholinergic activity in striatum.
| Drug | Brand |
|---|---|
| Trihexyphenidyl | Generic |
| Benztropine | Cogentin |
Best for: Tremor and rigidity (less effective for bradykinesia)
Also used for: Drug-induced pseudoparkinsonism from antipsychotics
Adverse Effects (classic anticholinergic "ABCDE"):
- Anhydrosis (dry skin)
- Bladder retention (urinary retention)
- Constipation
- Dry mouth / blurred vision / Dysphoria
- Elevated heart rate (tachycardia)
- Confusion and memory impairment - especially dangerous in elderly
Contraindications: Glaucoma, benign prostatic hyperplasia (BPH)
🟣 CLASS 7: Amantadine
Amantadine | Brand: Gocovri
Mechanism (multiple):
- ↑ Presynaptic dopamine release
- Inhibits dopamine reuptake
- NMDA glutamate receptor antagonist → reduces dyskinesias
- Weak anticholinergic activity
Uses:
- Mild early PD (monotherapy)
- Adjunct to levodopa
- Treatment of levodopa-induced dyskinesias (ER formulation - Gocovri)
Adverse Effects:
- Livedo reticularis - mottled purplish skin discoloration (characteristic!)
- Ankle edema
- Confusion, hallucinations
- Insomnia
5. PD Psychosis - Special Consideration
| Problem | Solution |
|---|---|
| PD drugs ↑ DA everywhere → hallucinations, psychosis | Can't easily use standard antipsychotics (they block DA → worsen motor function) |
| Pimavanserin | 5-HT2A inverse agonist - NO dopamine blockade → treats psychosis WITHOUT worsening motor symptoms |
| Quetiapine, Clozapine | Very weak DA blockade - relatively safer than typical antipsychotics |
6. Complete Summary Diagram
PARKINSONISM DRUGS (Lippincott Ch. 15)
│
├── LEVODOPA + CARBIDOPA ──── FIRST-LINE
│ ├── Sinemet (levodopa/carbidopa)
│ └── Stalevo (levodopa/carbidopa/entacapone)
│
├── DOPAMINE AGONISTS ──── D2/D3 direct stimulation
│ ├── Pramipexole (Mirapex) ← impulse control disorders
│ ├── Ropinirole (Requip) ← impulse control disorders
│ ├── Rotigotine (Neupro patch)
│ ├── Bromocriptine (Parlodel) ← ergot - fibrosis risk
│ └── Apomorphine (Apokyn) ← rescue SC injection
│
├── MAO-B INHIBITORS ──── ↓ dopamine breakdown
│ ├── Selegiline (Eldepryl) ← amphetamine metabolite → insomnia
│ ├── Rasagiline (Azilect) ← 5× potent, no amphetamine
│ └── Safinamide (Xadago) ← reversible; adjunct to LD/CD
│
├── COMT INHIBITORS ──── ↑ levodopa CNS availability
│ ├── Entacapone (Comtan) ← per-dose; peripheral only
│ ├── Opicapone (Ongentys) ← once-daily; peripheral only
│ └── Tolcapone (Tasmar) ← central+peripheral; hepatotoxic
│
├── A2A ANTAGONIST ──── indirect DA enhancement
│ └── Istradefylline (Nourianz)
│
├── ANTICHOLINERGICS ──── ↓ ACh excess; best for tremor
│ ├── Trihexyphenidyl
│ └── Benztropine (Cogentin)
│
└── AMANTADINE (Gocovri)
└── ↑ DA release + ↓ reuptake + NMDA block
→ also treats levodopa-induced dyskinesias
7. Quick Comparison Table
| Drug Class | Mechanism | Best For | Key Side Effect |
|---|---|---|---|
| Levodopa/Carbidopa | DA precursor + peripheral decarboxylase inhibitor | Bradykinesia, rigidity, tremor | Dyskinesias, on-off |
| Dopamine agonists | Direct D2/D3 stimulation | Early PD or adjunct | Impulse control, sleep attacks |
| MAO-B inhibitors | ↓ DA metabolism | Adjunct, prolong levodopa | Serotonin syndrome |
| COMT inhibitors | ↓ levodopa peripheral conversion | Reduce off-time | Diarrhea; tolcapone → hepatotoxicity |
| A2A antagonists | Indirect DA enhancement | "Off" episodes | Dyskinesia |
| Anticholinergics | ↓ ACh excess | Tremor, drug-induced parkinsonism | Confusion in elderly, dry effects |
| Amantadine | Multi-mechanism DA + NMDA block | Dyskinesias, mild PD | Livedo reticularis |
Source: Lippincott Illustrated Reviews: Pharmacology, Chapter 15
This is a shared conversation. Sign in to Orris to start your own chat.