phenytoin
Reading File
Finding Sources
Searching PubMed
phenytoin antiepileptic pharmacology
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Here is a comprehensive overview of phenytoin drawn from Goodman & Gilman's Pharmacological Basis of Therapeutics and Katzung's Basic & Clinical Pharmacology (16th ed.):
Phenytoin (Diphenylhydantoin)
Chemistry
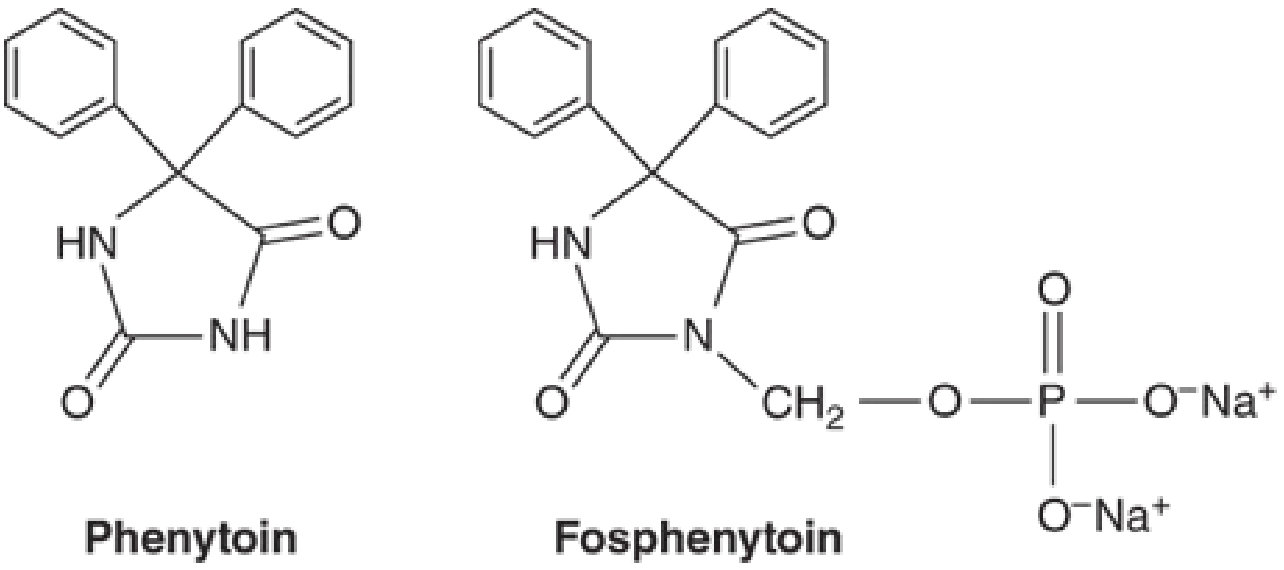
Phenytoin (5,5-diphenylhydantoin) is a hydantoin derivative - a 5-membered ring compound structurally related to barbiturates. It has a pKa of ~8.06-8.33 and is poorly water-soluble in its free-base form. Fosphenytoin is the water-soluble disodium phosphate ester prodrug, rapidly converted to phenytoin in plasma, used for IV/IM administration.
Mechanism of Action
Phenytoin is a voltage-gated sodium channel blocker. It slows the rate of recovery of Na+ channels from inactivation, reducing sustained repetitive firing of action potentials evoked by depolarization. The effect is:
- Voltage-dependent - greater effect when the membrane is depolarized
- Use-dependent - more pronounced during high-frequency firing
At therapeutic concentrations, phenytoin acts selectively on Na+ channels without affecting spontaneous neuronal activity or GABA/glutamate responses. At 5-10x therapeutic concentrations, it also suppresses spontaneous activity and enhances GABA responses - effects that underlie its toxic manifestations.
Clinical Uses
| Indication | Notes |
|---|---|
| Focal (partial) seizures | First-line historically; now second-line |
| Generalized tonic-clonic seizures | Focal-to-bilateral or idiopathic generalized |
| Status epilepticus (IV) | Fosphenytoin preferred IV |
| NOT absence seizures | May worsen them |
| NOT juvenile myoclonic epilepsy | May worsen myoclonic seizures |
| NOT Dravet syndrome | May worsen |
Due to adverse effects and drug interactions, phenytoin is no longer considered first-line for chronic epilepsy management.
Pharmacokinetics
Absorption
- Nearly complete from the GI tract, but highly formulation-dependent
- Extended-release capsule: peak at 4-12 hours (allows once-daily dosing)
- Prompt-release capsule: peak at 1.5-3 hours
- IM injection is NOT recommended - unpredictable absorption with muscle precipitation
Distribution
- Protein binding: ~90% to serum albumin
- Volume of distribution: 0.6-0.7 L/kg
- Small changes in bound fraction dramatically alter free (active) drug levels
- Situations increasing free phenytoin: hypoalbuminemia (liver disease, nephrotic syndrome), hyperbilirubinemia, neonates, elderly, drug displacement (warfarin, valproate)
Metabolism - KEY CONCEPT: Zero-Order / Saturation Kinetics
At low concentrations, phenytoin follows first-order kinetics. As concentrations rise into the therapeutic range, hepatic metabolic capacity becomes saturated, shifting to zero-order (Michaelis-Menten) kinetics - a constant amount (not fraction) is metabolized per unit time.
Clinical implication: Small dose increases can cause disproportionately large rises in plasma levels and rapid toxicity.
- Metabolized by CYP2C9 and CYP2C19 to inactive hydroxylated metabolites
- Half-life: 12-36 hours (average ~24 hours) at low-to-mid therapeutic range; much longer at high concentrations
- Time to steady state: 5-7 days at low levels; up to 4-6 weeks at higher levels
Therapeutic Range
| Parameter | Value |
|---|---|
| Therapeutic total level | 10-20 mcg/mL |
| Nystagmus appears at | ~20 mcg/mL |
| Free phenytoin therapeutic | 0.75-1.25 mcg/mL |
Correction for hypoalbuminemia: Measured total level underestimates free drug. Use the Sheiner-Tozer equation when albumin is low.
Drug Interactions (Extensive)
Phenytoin is both a substrate and inducer of CYP enzymes, creating complex bidirectional interactions:
Drugs that INCREASE phenytoin levels (CYP2C9/2C19 inhibitors):
- Isoniazid (especially slow acetylators)
- Fluoxetine, fluvoxamine
- Metronidazole, miconazole
- Fluorouracil
- Valproate (dual effect: displaces from protein binding + inhibits metabolism)
Drugs that DECREASE phenytoin levels:
- Carbamazepine (CYP induction)
- Alcohol (chronic use)
- Barbiturates
Drugs whose levels are DECREASED by phenytoin (CYP induction):
- Oral contraceptives (risk of contraceptive failure)
- Warfarin
- Corticosteroids
- Many other CYP substrates
Adverse Effects
CNS (dose-related, most common)
- Nystagmus (first sign of toxicity, at ~20 mcg/mL)
- Diplopia, ataxia, dysarthria
- Sedation, cognitive impairment
- At toxic doses: cerebellar atrophy (long-term), worsening seizures
Chronic use
- Gingival hyperplasia - ~20% of chronic users; minimized by good oral hygiene
- Hirsutism - particularly troublesome in females
- Coarsening of facial features
- Osteomalacia / osteoporosis - due to altered vitamin D and vitamin K metabolism; leads to hypocalcemia, elevated alkaline phosphatase
- Megaloblastic anemia - folate-related
- Hyperglycemia/glycosuria - inhibition of insulin secretion
- SIADH suppression (inhibits ADH release)
Hypersensitivity / Idiosyncratic
- Morbilliform rash: 2-5% of patients
- Stevens-Johnson syndrome / toxic epidermal necrolysis (rare but serious)
- Hepatic necrosis
- Hematological: neutropenia, leukopenia, agranulocytosis, aplastic anemia, thrombocytopenia
- Drug-induced SLE
IV Administration
- Purple glove syndrome - purplish-black discoloration with edema/pain distal to IV site (due to propylene glycol vehicle and alkaline pH)
- Cardiac arrhythmias and hypotension with rapid IV infusion
- Maximum IV rate: <50 mg/min (phenytoin) or <150 mg phenytoin equivalents/min (fosphenytoin)
Teratogenicity
- Fetal hydantoin syndrome - craniofacial abnormalities, digit/nail hypoplasia, growth restriction, cognitive impairment
- Neonatal coagulopathy (reduced vitamin K-dependent clotting factors) - treat/prevent with vitamin K
Formulations Summary
| Form | Route | Notes |
|---|---|---|
| Extended-release capsule | Oral | Once-daily dosing possible |
| Prompt-release capsule | Oral | 2-3x daily dosing |
| Suspension / chewable tabs | Oral | Free-base form |
| IV solution | IV | Contains propylene glycol, pH 12; risk of purple glove syndrome |
| Fosphenytoin (Cerebyx) | IV / IM | Water-soluble prodrug; preferred for parenteral use |
Clinical Monitoring
- Monitor total phenytoin levels (therapeutic: 10-20 mcg/mL); correct for albumin when appropriate
- Monitor free phenytoin when protein binding is altered (renal failure, hypoalbuminemia, pregnancy, drug interactions)
- Check LFTs, CBC, and bone density in long-term users
- Serum level monitoring is mandatory when switching formulations
Sources: - Goodman & Gilman's Pharmacological Basis of Therapeutics, Chapter 20 | - Katzung's Basic & Clinical Pharmacology, 16th Ed., Chapter 24
Recent evidence note: A 2025 network meta-analysis (PMID 39808752) of antiseizure medications for post-stroke seizures suggests newer agents may outperform phenytoin in this setting, consistent with its declining role as a first-line agent.
This is a shared conversation. Sign in to Orris to start your own chat.