Cardiac Transplantation university exam answer
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
I now have comprehensive content from multiple major textbooks. Let me compile the complete exam answer:
Cardiac Transplantation - University Exam Answer
1. Introduction and Historical Background
Cardiac (heart) transplantation is the surgical replacement of a diseased, end-stage failing heart with a donor heart from a brain-dead or circulatory-dead donor. The first human cardiac transplant was performed by Christiaan Barnard in Cape Town in 1967. The field was transformed by three key advances:
- Cyclosporine-based immunosuppression (1980s) - dramatically reduced acute rejection
- Endomyocardial biopsy - enabled histopathologic monitoring of rejection
- Careful recipient and donor selection protocols
Today, over 5,000 cardiac transplants are performed worldwide annually, with a 1-year survival of ~90% and 5-year survival >70%.
- Robbins, Cotran & Kumar Pathologic Basis of Disease
- Harrison's Principles of Internal Medicine 22E
2. Indications
Heart transplantation is reserved for patients with ACC/AHA Stage D (advanced, refractory) heart failure - those whose condition is refractory to optimal guideline-directed medical therapy (GDMT).
Specific Indications (ISHLT Guidelines):
| Indication | Detail |
|---|---|
| ACC/AHA Stage D HF | Refractory to optimal GDMT |
| MCS dependence | Dependent on mechanical circulatory support to survive |
| Inotrope dependence | Cannot be weaned from IV inotropes |
| Severely reduced exercise capacity | Peak VO2 ≤14 mL/kg/min (not on β-blocker) or ≤12 mL/kg/min (on β-blocker) on CPET |
| HF prognosis scores | Selected ambulatory patients with ambiguous CPET |
Common underlying etiologies:
-
Ischemic cardiomyopathy (most common in adults in developed countries)
-
Idiopathic dilated cardiomyopathy (DCM) - younger patients
-
Valvular heart disease, viral myocarditis, congenital heart disease
-
Restrictive/hypertrophic cardiomyopathy, amyloidosis, sarcoidosis
-
Sabiston Textbook of Surgery, 21e
3. Contraindications
Absolute Contraindications:
- Pulmonary vascular resistance (PVR) >6 Wood units - heart-lung transplantation should be considered instead
- GFR <30 mL/min/1.73 m² - heart-kidney transplant should be considered
- Active malignancy (depends on prognosis)
- Active systemic infection
- Non-compliance or inability to adhere to lifelong immunosuppression
Relative Contraindications:
-
PVR 4-6 Wood units (efforts to reduce PVR medically first)
-
Age >70 (relative, center-dependent)
-
Diabetes with end-organ damage or HbA1c >7.5% persistently
-
Symptomatic peripheral/cerebrovascular disease not amenable to revascularization
-
Severe irreversible pulmonary disease
-
Morbid obesity (BMI >35)
-
Active substance abuse (alcohol, drugs, tobacco)
-
Severe psychiatric disorder
-
Inadequate social support
-
Sabiston Textbook of Surgery (Table 57.1)
-
Braunwald's Heart Disease
4. Pre-Transplant Evaluation
A multidisciplinary committee (cardiologists, cardiac transplant surgeons, social workers, psychiatrists, care managers) evaluates all candidates. Key workup includes:
- Laboratory: CBC, metabolic panel, LFTs, urinalysis, coagulation, thyroid, urine drug screen, HIV, hepatitis B/C, TB screen, CMV IgG/IgM, RPR/VDRL, panel reactive antibodies (PRA), ABO/Rh blood type, lipids, HbA1c
- Cardiac: ECG, right and left heart catheterization (to assess PVR), cardiopulmonary exercise testing (CPET) with VO2 max
- Pulmonary: CXR, pulmonary function tests
- Screening: Age-appropriate malignancy screening
- Psychosocial: Substance abuse history, mental health assessment, social support
Braunwald's Heart Disease - Evaluation of the Heart Transplant Candidate
5. Donor Selection
5a. Brain Death vs. Circulatory Death Donors
- Donation after Brain Death (DBD): Historically the standard. The cardiopulmonary system remains functional at procurement - no warm ischemia. Brain death declared when there is absence of brainstem reflexes, motor responses, and respiratory drive in a normothermic patient without metabolic derangements.
- Donation after Circulatory Death (DCD): Increasingly used; requires controlled withdrawal of life support and cessation of spontaneous circulation before procurement. Carries a period of warm ischemia, which is injurious. Advances in preservation strategies (normothermic machine perfusion) have made DCD heart transplantation feasible.
5b. Donor Assessment Criteria
- Echocardiography: Normal or near-normal LV/RV function (EF ≥45% generally acceptable); mild depression may improve with time
- ABO compatibility (mandatory)
- HLA matching: Cross-matching performed; virtual crossmatch using PRA
- Size matching: Donor/recipient weight ratio; female donor to male recipient increases risk of primary graft dysfunction
- Ischemic time: Cold ischemia <4-6 hours optimal
- Coronary angiography in older donors
- No active malignancy or transmissible infection
6. Surgical Technique
6a. Recipient Preparation
- Median sternotomy and cardiopulmonary bypass (CPB)
- Anticoagulation with heparin
- Recipient heart is explanted
6b. Orthotopic Heart Transplantation
There are two main anastomotic techniques:
1. Classic Biatrial Technique (Lower and Shumway):
- Posterior walls of the recipient left and right atria are preserved
- Donor atria anastomosed to remaining recipient atrial cuffs
- Five anastomoses: LA, RA, pulmonary artery, aorta
- Disadvantage: leaves native sinoatrial (SA) node tissue - can cause two distinct P-wave rhythms and tricuspid regurgitation
2. Bicaval Technique (current standard):
- Entire right atrium of recipient is excised
- Direct superior vena cava (SVC) and inferior vena cava (IVC) anastomoses between donor and recipient
- Left atrial anastomosis around pulmonary vein orifices
- Plus pulmonary artery and aortic anastomoses (total 5-6 anastomoses)
- Advantages: Preserves normal atrial geometry, less tricuspid regurgitation, better sinus node function, lower incidence of arrhythmias
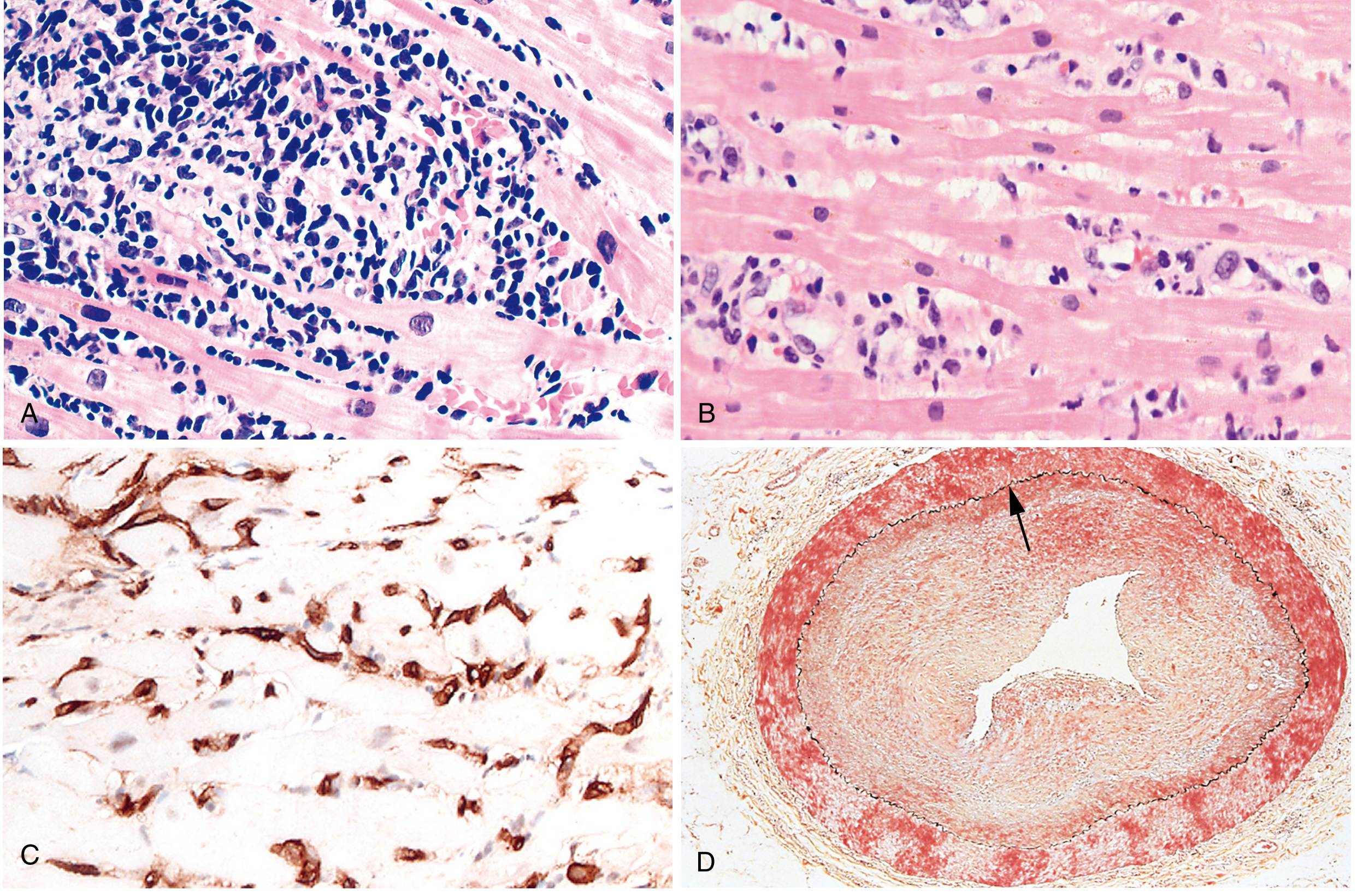
Fig. 12.38 - Complications of heart transplantation (Robbins, Cotran & Kumar Pathologic Basis of Disease): (A) Cellular allograft rejection with lymphocytic infiltrate and myocyte damage. (B) Antibody-mediated rejection with plump activated endothelium. (C) C4d immunostaining of capillaries (complement activation). (D) Allograft vasculopathy with critical concentric intimal stenosis.
7. Cardiac Allograft Preservation
- Cold static storage in cardioplegic solution (University of Wisconsin solution, Custodiol HTK) is standard
- Optimal cold ischemic time: <4 hours (ideally), maximum 6 hours
- Normothermic machine perfusion (NMP): Emerging technology allowing ex-vivo assessment and preservation of DCD hearts - extends viable ischemic time and allows hearts to be assessed before transplantation
- The heart is transported packed in cold saline in a cooler
8. Immunosuppression
Cardiac allografts are of moderate immunogenicity (between lung - most immunogenic, and liver - least immunogenic). The standard is triple-drug immunosuppression:
Standard Maintenance Regimen
Tacrolimus + Mycophenolate Mofetil (MMF) + Prednisone - the most widely used combination
| Drug Class | Drug | Mechanism | Side Effects |
|---|---|---|---|
| Calcineurin inhibitors | Tacrolimus | Binds FK506-binding protein → inhibits calcineurin → blocks NFAT → no IL-2 production → no T-cell activation | Hypertension, dyslipidemia, diabetes, alopecia |
| Cyclosporine | Binds cyclophilin → inhibits calcineurin | Hypertension, dyslipidemia, gum hypertrophy, hirsutism/hypertrichosis | |
| Antiproliferative agents | Mycophenolate Mofetil (MMF) | Inhibits inosine monophosphate dehydrogenase (IMPDH) → blocks de novo purine synthesis → inhibits T and B lymphocyte proliferation | Leukopenia, GI toxicity |
| Azathioprine | Prodrug → 6-mercaptopurine → inhibits DNA synthesis | Bone marrow suppression, pancreatitis, hepatitis | |
| Corticosteroids | Prednisone, Methylprednisolone | Modulates gene transcription, inhibits cytokine production, suppresses inflammatory cell migration | Diabetes, osteoporosis, weight gain, infections |
| mTOR inhibitors | Sirolimus, Everolimus | Bind FKBP12 → inhibit mTOR → block cell cycle at G1→S transition | Delayed wound healing, hyperlipidemia, pneumonitis, pericardial effusion |
Induction Immunosuppression
Given at time of transplant for high-risk patients (multiparous women, allosensitized individuals, retransplants, renal dysfunction):
- Basiliximab (IL-2 receptor antagonist, anti-CD25) - monoclonal antibody; well-tolerated
- Antithymocyte globulin (ATG) - polyclonal; causes T-cell depletion via complement-dependent lysis; side effects: cytokine release syndrome, leukopenia, thrombocytopenia
Steroid Weaning
Over months, as surveillance biopsies confirm quiescence, steroids are gradually weaned - sometimes eliminated after the first year.
- Harrison's Principles of Internal Medicine 22E, Table 27-2
- Sabiston Textbook of Surgery
9. Allograft Rejection
9a. Acute Cellular Rejection (T-cell mediated)
- Most common type
- Pathology: Interstitial lymphocytic infiltrate + myocyte damage (resembles myocarditis)
- May include interstitial edema
- Cytokines can impair contractility without overt myocyte damage
- Monitoring: Routine endomyocardial biopsy (RV) - the only reliable means to diagnose rejection before irreversible damage
- ISHLT Grading:
- Grade 0: No rejection
- Grade 1R (Mild): Interstitial/perivascular infiltrate with ≤1 focus of myocyte damage
- Grade 2R (Moderate): ≥2 foci of infiltrate with myocyte damage
- Grade 3R (Severe): Diffuse infiltrate with multifocal myocyte damage ± edema, hemorrhage, vasculitis
- Treatment: Augmented immunosuppression; IV methylprednisolone pulse therapy; anti-T-cell therapy for resistant cases
9b. Antibody-Mediated Rejection (Humoral)
- Caused by donor-specific antibodies (DSA) directed against MHC (HLA) antigens on donor endothelium
- Mechanism: Complement activation + Fc-receptor-bearing cell recruitment → endothelial injury → microvascular thrombosis
- Pathology: Mild perivascular edema, scattered intravascular inflammatory cells, plump activated endothelium
- Diagnosis confirmed by: Immunohistochemistry for C4d (complement component) in capillaries - strong brown staining
- Treatment: Plasmapheresis, IVIG, anti-B cell therapy (rituximab), aggressive immunosuppression
9c. Chronic Rejection = Allograft Vasculopathy
10. Cardiac Allograft Vasculopathy (CAV)
CAV is the single most important long-term limitation of cardiac transplantation.
- Nature: Late, progressive, diffuse concentric intimal proliferation predominantly in the coronary arteries
- Distinct from native atherosclerosis (which is eccentric, focal, and calcified)
- Caused by chronic immune injury to the graft endothelium (both T-cell and antibody-mediated mechanisms)
- Consequence: Ischemic injury, silent MI (denervated heart - no angina), graft dysfunction, sudden cardiac death
- Within 5 years, significant CAV develops in a substantial proportion of recipients
- CMV infection is associated with accelerated development of CAV
- Monitoring: Annual coronary angiography; intravascular ultrasound (IVUS) more sensitive
- Treatment: Statins (reduce severity), mTOR inhibitors (sirolimus, everolimus - slow progression), PCI for focal lesions, but retransplantation is the only definitive option
11. Other Complications
Early Complications
| Complication | Details |
|---|---|
| Primary Graft Dysfunction (PGD) | Leading cause of early death; LV or RV failure; treated with vasopressors/inotropes, ECMO, VAD |
| Right Ventricular Failure | Donor RV fails against pre-existing elevated recipient PVR; treated with inhaled nitric oxide, sildenafil, milrinone |
| Bleeding | Especially in patients with prior cardiac surgery |
| Arrhythmias | Sinus node dysfunction, need for pacemaker in 5-10%; complete heart block |
Infections
Immunosuppression creates susceptibility to opportunistic infections:
- Bacterial: Most common in early post-operative period (pneumonia, wound infections)
- CMV: Most important viral pathogen - affects GI tract and lung; prophylaxis with valganciclovir (900 mg/day for 3-6 months); CMV+ donor to CMV- recipient = highest risk
- EBV: Associated with post-transplant lymphoproliferative disorder (PTLD) - ~50% of PTLD cases are EBV-associated; treatment includes immunosuppression reduction
- Aspergillus: Invasive pulmonary aspergillosis - mortality >50%; treat with voriconazole or amphotericin B
- PCP (Pneumocystis jiroveci): Prophylaxis with TMP-SMX
Malignancy
- Chronic T-cell immunosuppression increases risk
- EBV-associated B-cell lymphomas (PTLD) - most important
- Skin cancers, Kaposi sarcoma
Renal Dysfunction
- Calcineurin inhibitors are nephrotoxic
- CKD develops in a significant proportion of long-term recipients
- May require kidney transplantation
12. Outcomes and Survival
| Time Point | Survival |
|---|---|
| 1-year | ~90% |
| 5-year | >70% |
| Median survival | ~12-13 years |
Causes of death:
- Early (<30 days): Primary graft dysfunction, surgical complications
- 1 month - 1 year: Rejection, infections
- >1 year: CAV (leading long-term cause), malignancy, rejection
13. Organ Allocation (OPTN/UNOS System)
The US organ allocation system (revised 2018) uses a 6-tier status system prioritizing by medical urgency:
- Status 1: VA-ECMO, VAD malfunction, life-threatening arrhythmias
- Status 2: IABP, TAH, non-dischargeable BiVAD/LVAD
- Status 3: Dischargeable LVAD candidates, certain VAD complications
- Status 4: Device-based therapy or continuous inotropic support
- Status 5: Re-transplantation, adult congenital HD, low EF + restrictive/hypertrophic CMP
- Status 6: All other candidates
14. Bridging to Transplantation
Patients awaiting transplant may be bridged with:
- Inotropic infusions (dobutamine, milrinone)
- Intra-aortic balloon pump (IABP)
- Left Ventricular Assist Device (LVAD): Most common; "bridge to transplantation" or "destination therapy"; outcomes with LVAD bridge are equivalent to direct transplantation
- Total Artificial Heart (TAH): For biventricular failure
- VA-ECMO: Short-term bridge in acute cardiogenic shock
Summary Table
| Aspect | Key Points |
|---|---|
| Indication | ACC/AHA Stage D HF, VO2 max ≤12-14 mL/kg/min, inotrope/MCS dependence |
| Key contraindication | PVR >6 Wood units, GFR <30, active malignancy |
| Surgical technique | Bicaval orthotopic preferred over biatrial |
| Immunosuppression | Tacrolimus + MMF + Prednisone (triple therapy) |
| Rejection monitoring | Endomyocardial biopsy (RV) |
| Cellular rejection | Lymphocytic infiltrate + myocyte damage; treat with IV methylprednisolone |
| Antibody-mediated rejection | DSA + C4d in capillaries; endothelial injury |
| Main long-term limitation | Cardiac allograft vasculopathy (CAV) - diffuse coronary intimal proliferation |
| Survival | 90% at 1 year; >70% at 5 years |
| Key infections | CMV (prophylaxis: valganciclovir), PCP (prophylaxis: TMP-SMX), EBV/PTLD |
Sources:
- Robbins, Cotran & Kumar - Pathologic Basis of Disease (10th ed.)
- Sabiston Textbook of Surgery (21st ed.)
- Braunwald's Heart Disease (12th ed.)
- Harrison's Principles of Internal Medicine (22nd ed., 2025)
- Fuster and Hurst's The Heart (15th ed.)
This is a shared conversation. Sign in to Orris to start your own chat.