Chagas’ disease
Reading File
Finding Sources
Searching PubMed
"Chagas disease"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a thorough response. Let me compile it.
Chagas Disease (American Trypanosomiasis)
Definition & Pathogen
Chagas disease is caused by Trypanosoma cruzi, an obligate intracellular protozoan parasite. It is synonymous with "American trypanosomiasis." T. cruzi is classified in the genus Trypanosoma alongside T. brucei (the cause of African sleeping sickness), but the two diseases are biologically and clinically distinct. - Goldman-Cecil Medicine, p. 3409
Epidemiology
- Endemic range: Mexico and all Central/South American countries; notably NOT the Caribbean islands. It is a zoonosis with a complex sylvatic cycle.
- Global burden: ~6-8 million people are chronically infected; ~28,000 new cases/year; ~12,000 deaths/year. A 2026 GBD analysis (PMID: 41202826) in Lancet Infectious Diseases provides the most current global burden estimates from 1990-2023.
- USA: ~240,000-350,000 immigrants are infected; only 7 documented autochthonous acute cases have been reported. Mandatory blood donor screening began in 2007; confirmed infection rate ~1:13,300 donors.
- Europe: Seen mainly in Latin American immigrants, especially Bolivians (~18% seroprevalence).
- Vector control success: Uruguay (1997), Chile (1999), and Brazil (2006) were certified free of vector transmission following major international insecticide/housing programs.
Vectors: Triatomine insects ("kissing bugs," reduviid bugs) - found in the walls and roofs of primitive dwellings, biting at night.
Transmission routes:
- Vector bite - parasite-laden feces contact skin breaks or mucosae (classic route)
- Blood transfusion / organ transplantation
- Congenital (mother-to-fetus) - occurs in ~1-2% of affected pregnancies
- Ingestion of contaminated food/drink
- Laboratory accidents
Life Cycle & Pathobiology
The triatomine bug ingests blood containing trypomastigotes, which multiply in its gut and are shed in feces during feeding. The metacyclic trypomastigotes contaminate the bite wound or mucosae of the new host. Once inside the host:
- Trypomastigotes enter local cells, transform into amastigotes, and multiply intracellularly, forming pseudocysts (host cells packed with amastigotes - pathognomonic histologic finding)
- When cells rupture, trypomastigotes re-enter the bloodstream, spreading systemically
- Tissues most heavily parasitized: myocardium, smooth muscle (GI tract), and autonomic ganglia of the heart, esophagus, and colon
Chronic disease mechanisms:
- Persistent low-level inflammation and immune-mediated damage (even with minimal parasites)
- Mononuclear cell infiltration, fibrosis, and destruction of intramural nerve ganglia (myenteric and submucosal plexuses)
- The resulting denervation drives both cardiomyopathy and GI megadisease
Clinical Phases
1. Acute Phase
Usually affects children; can occur at any age. Most patients are asymptomatic or mildly symptomatic.
| Feature | Details |
|---|---|
| Chagoma | Inflammatory swelling at parasite entry site, with local lymphadenopathy |
| Romaña sign | Painless unilateral periorbital edema - classic but rarely seen; occurs when conjunctiva is the portal of entry |
| Systemic symptoms | Fever, malaise, anorexia, edema of face/lower extremities, generalized lymphadenopathy, hepatosplenomegaly |
| Severe complications | Myocarditis (sometimes fatal), meningoencephalitis (rare) |
| Duration | Self-limiting over 6-8 weeks without treatment; patient then enters indeterminate phase |
2. Indeterminate Phase
- Subpatent parasitemia (undetectable on smear)
- No signs or symptoms
- Positive serology
- Can last a lifetime in ~70-80% of chronically infected persons
- These individuals can still transmit via blood donation or vertically to offspring
3. Chronic Symptomatic Phase (~20-30% of infected)
Develops insidiously over years to decades after initial infection.
A. Chagasic Cardiomyopathy
The most common and life-threatening manifestation:
- Biventricular dilation with thinning of walls; right-sided failure can predominate in advanced cases
- Characteristic apex aneurysm of the left ventricle (inferolateral) - hallmark finding
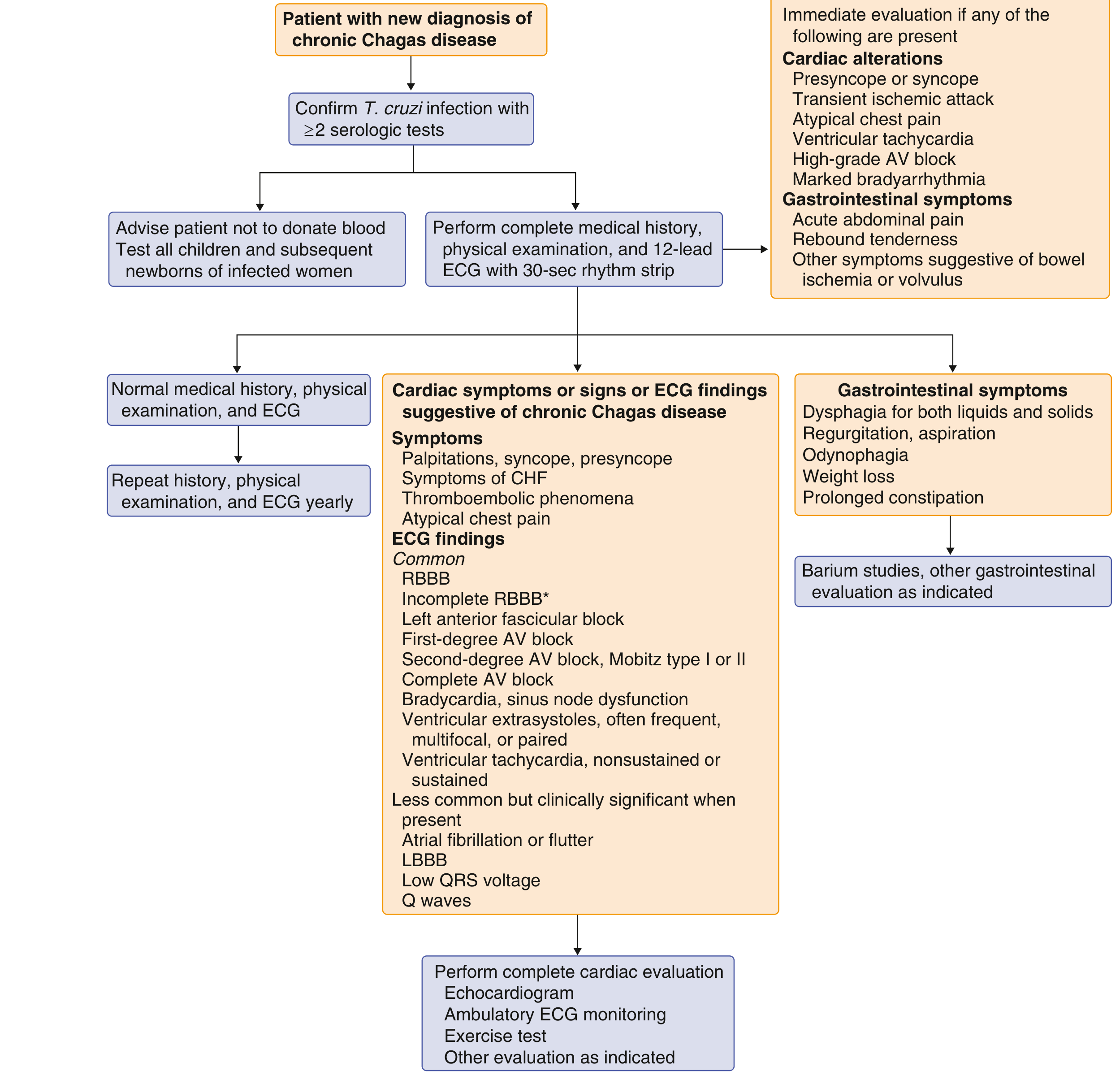
- ECG abnormalities (see diagnostic algorithm below):
- Right bundle branch block (RBBB) - most common early ECG finding
- Left anterior fascicular block
- Complete AV block
- Ventricular extrasystoles (frequent, multifocal, or paired)
- Sustained monomorphic VT from inferolateral scar (RBBB right-axis morphology)
- Sudden death - can be the first manifestation; from VT/VF or heart block
- Thromboembolism - mural thrombi are common; presents as stroke, pulmonary embolism, or peripheral arterial embolism
- Chagas disease is an independent risk factor for stroke
Rassi Score - Predicting Death in Chagas Heart Disease (points):
| Characteristic | Points |
|---|---|
| Male sex | 2 |
| NYHA functional class III or IV | 5 |
| Low QRS voltage on ECG | 3 |
| Cardiomegaly on chest X-ray | 5 |
| LV systolic dysfunction on echo | 3 |
| Nonsustained ventricular tachycardia | 3 |
| LBBB, advanced AV block, or sinus node dysfunction | 3 |
B. Chronic Gastrointestinal Disease ("Megadisease")
Occurs in ~1/3 of patients, particularly in Brazilian strains (megadisease is absent in Colombian strains):
- Megaesophagus: Destruction of myenteric plexus → achalasia-like syndrome; dysphagia, odynophagia, regurgitation, hypersalivation, salivary gland hypertrophy; can cause aspiration pneumonia and malnutrition
- Megacolon: Constipation, fecal impaction, toxic megacolon, volvulus (especially sigmoid)
- Megaduodenum and megajejunum can also occur but are usually asymptomatic
Diagnosis
Acute / Congenital / Reactivation
- Wet preparation of blood: Look for motile trypomastigotes (direct microscopy)
- PCR: Gold standard - highest sensitivity for acute, congenital, and reactivation in immunosuppressed patients
- Culture in special liquid media (less practical)
Chronic Infection
- Serology is the standard: at least 2 different serologic tests must be positive (complement fixation, ELISA, indirect immunofluorescence)
- Serology cross-reacts with malaria, syphilis, leishmaniasis, and some collagen vascular diseases - hence the requirement for confirmatory testing
- Peripheral parasitemia is not reliably detected in chronic disease
Evaluation Algorithm for Newly Diagnosed Chronic Chagas Disease:
Treatment
Antiparasitic Drugs
| Drug | Regimen | Notes |
|---|---|---|
| Benznidazole (preferred) | 5-7 mg/kg/day orally divided q12h for 60 days | FDA-approved in children 2-12 yrs; side effects: allergic dermatitis, peripheral neuropathy, insomnia, GI symptoms |
| Nifurtimox | 8-10 mg/kg/day orally divided q6-8h for 60-90 days | Available in USA via CDC investigational protocol (404-639-2888); side effects: nausea, vomiting, anorexia, weight loss, headache, polyneuropathy |
Cure rates:
- Acute/congenital infection: 80-100%
- Chronic indeterminate phase (children/young adults): Substantial benefit; treatment recommended
- Chronic with established cardiomyopathy or GI disease: Benefit NOT established - neither drug can reverse established cardiac or GI damage
⚠️ Important update: A major randomized controlled trial (the BENEFIT trial) found that treating established chronic Chagas cardiomyopathy with benznidazole did not offer clinical benefit despite reducing parasitemia. This is noted in Katzung's pharmacology and supported by recent systematic reviews. PMID: 40453704 (2024 meta-analysis of treatment options).
Management of Cardiac Complications
- Antiarrhythmics, beta-blockers for VT
- ICD implantation for life-threatening arrhythmias - a recent 2025 systematic review/meta-analysis (PMID: 40924256) assessed ICD outcomes in Chagas heart disease
- Standard heart failure therapy (ACE inhibitors, beta-blockers, diuretics)
- Anticoagulation for thromboembolic risk (mural thrombi)
- Heart transplantation in end-stage disease (T. cruzi can reactivate post-transplant in the immunosuppressed host - treat with antiparasitic agents)
Management of GI Complications
- Megaesophagus: Balloon dilation of lower esophageal sphincter; peroral endoscopic myotomy (POEM) if dilation fails - same approach as idiopathic achalasia
- Megacolon (early): High-fiber diet, laxatives, enemas; manual disimpaction for fecal impaction
- Megacolon (advanced/volvulus): Surgery - typically sigmoid resection with partial rectum removal
Special Populations
Pregnancy
- Vertical transmission occurs in ~1-2% of pregnancies
- Screen women with history of time in endemic areas with T. cruzi serology; confirm via CDC Parasitic Branch
- Antiparasitic treatment is typically delayed until after delivery
- Newborns: Cord blood smear/PCR at birth; repeat at 4-6 weeks if negative; then serology at 9-12 months (maternal IgG crosses placenta)
- If congenital infection confirmed: treat - cure rate >90%
Immunosuppressed Hosts (HIV, transplant recipients)
- Reactivation presents as acute myocarditis, CNS abscesses (chagoma of the brain), or skin lesions
- Diagnose by PCR or blood smear
- Treat with benznidazole or nifurtimox (suppresses acute episode but long-term benefit unclear)
Prevention
- Vector control: Housing improvement, insecticide spraying of dwellings, education
- Blood screening: Universal donor screening in endemic countries; selective screening in USA since 2007
- Oral transmission prevention: Food safety standards (e.g., avoiding contaminated açaí or sugar cane juice)
- Congenital prevention: Treat T. cruzi-infected women before pregnancy
- No validated prophylaxis protocol for immunosuppressed hosts; no licensed vaccine
Sources: Goldman-Cecil Medicine (p. 3406-3412); Rosen's Emergency Medicine; Braunwald's Heart Disease; Sleisenger and Fordtran's GI and Liver Disease; Creasy & Resnik's Maternal-Fetal Medicine; Katzung's Basic and Clinical Pharmacology.
This is a shared conversation. Sign in to Orris to start your own chat.