Large white kidney - specimen pathology
Reading File
Finding Sources
Finding Sources
Searching the Web
large white kidney pathology nephrotic syndrome gross specimen
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information. Let me compile the full answer:
Large White Kidney - Specimen Pathology
What Is It?
"Large white kidney" is a classic gross pathological term describing the macroscopic appearance of the kidney in nephrotic syndrome, most characteristically seen in minimal change disease (MCD) and membranous nephropathy. The kidney is:
- Enlarged (increased in size and weight)
- Pale/white on the cut surface - due to lipid and protein accumulation in tubular cells
- Smooth outer surface
- Waxy or "greasy" texture on cut section (reflecting the lipid content)
The pale color is the direct result of massive lipid and protein uptake by proximal tubular epithelial cells, which absorb the enormous quantities of lipoproteins leaking through the damaged glomerular filter. This is why the historical name for minimal change disease was "lipid nephrosis" - the tubular cells are heavily laden with lipid droplets.
Underlying Causes (in order of association)
| Cause | Notes |
|---|---|
| Minimal Change Disease (MCD) | Most classic association; most common in children 2-6 yrs |
| Membranous Nephropathy | Most common cause in white adults |
| Focal Segmental Glomerulosclerosis (FSGS) | More common in African Americans |
| Diabetic Nephropathy | Secondary cause; kidneys also enlarged |
| Amyloidosis | Waxy large kidneys; pale/gray color |
| Lupus Nephritis | Secondary nephrotic pattern |
Gross Morphology
On specimen examination, the kidney shows:
- Increased size and weight - enlarged due to edema, lipid/protein accumulation
- Pale/white cortex - loss of normal pink color from lipid deposition in tubular cells
- Smooth capsule - no scarring or bosselation (unlike chronic kidney disease)
- Yellow streaks may be visible in the cortex - due to tubular lipid deposits (particularly prominent in MCD)
- Preserved corticomedullary distinction - unlike end-stage kidney disease
Microscopic Pathology
Light Microscopy
Minimal Change Disease:
- Glomeruli appear completely normal by light microscopy - this is the defining feature
- Proximal tubular cells heavily laden with lipid droplets and protein (PAS-positive hyaline droplets)
- No inflammation, no proliferation, no immune deposits
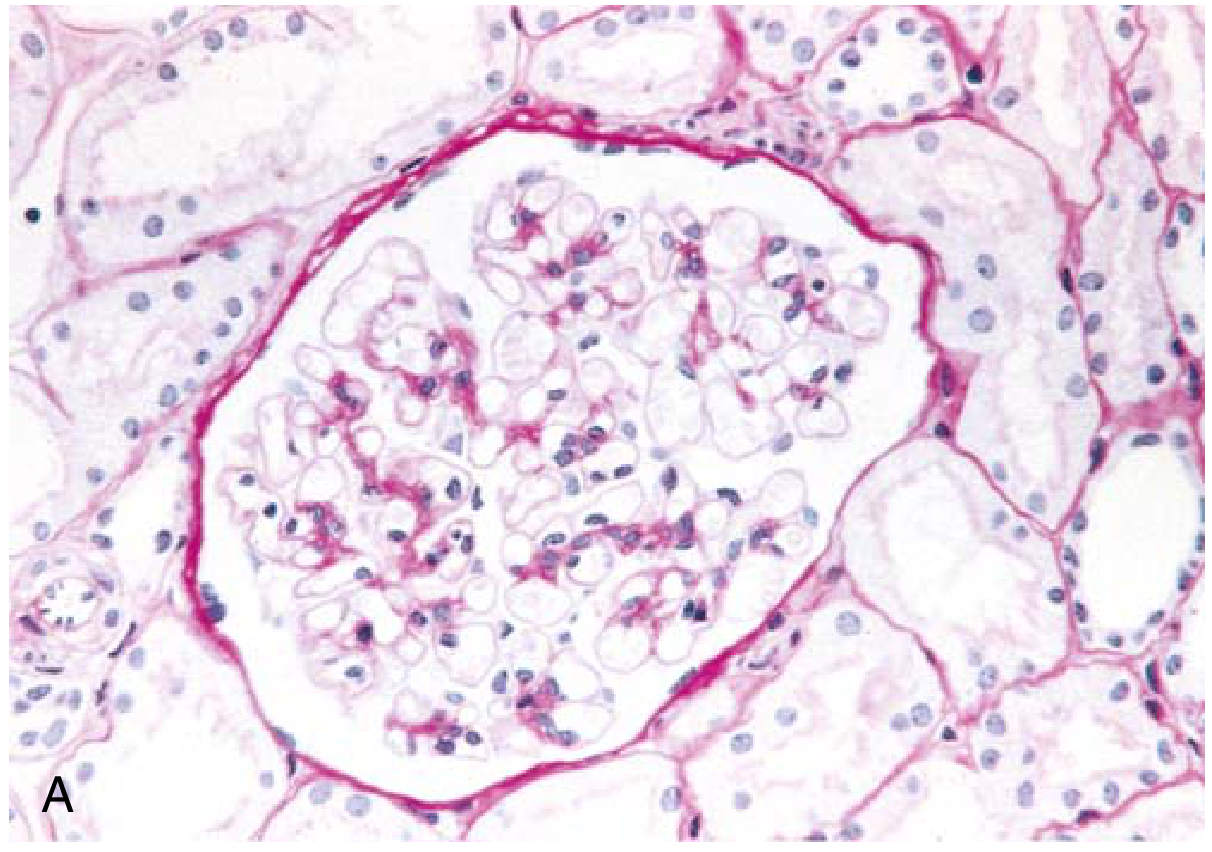
Minimal change disease: Normal glomerulus on PAS stain. Note the lack of proliferation or deposits - Robbins & Kumar Basic Pathology, Fig. 12.4A
Electron Microscopy
The hallmark lesion is:
- Diffuse effacement (fusion) of podocyte foot processes - seen on all capillary loops
- The GBM appears normal thickness
- No electron-dense deposits
- Podocytes show vacuolization, microvillus formation, focal detachment
- This foot process effacement represents simplification of epithelial cell architecture with flattening and retraction due to collapse of the central actin cytoskeleton
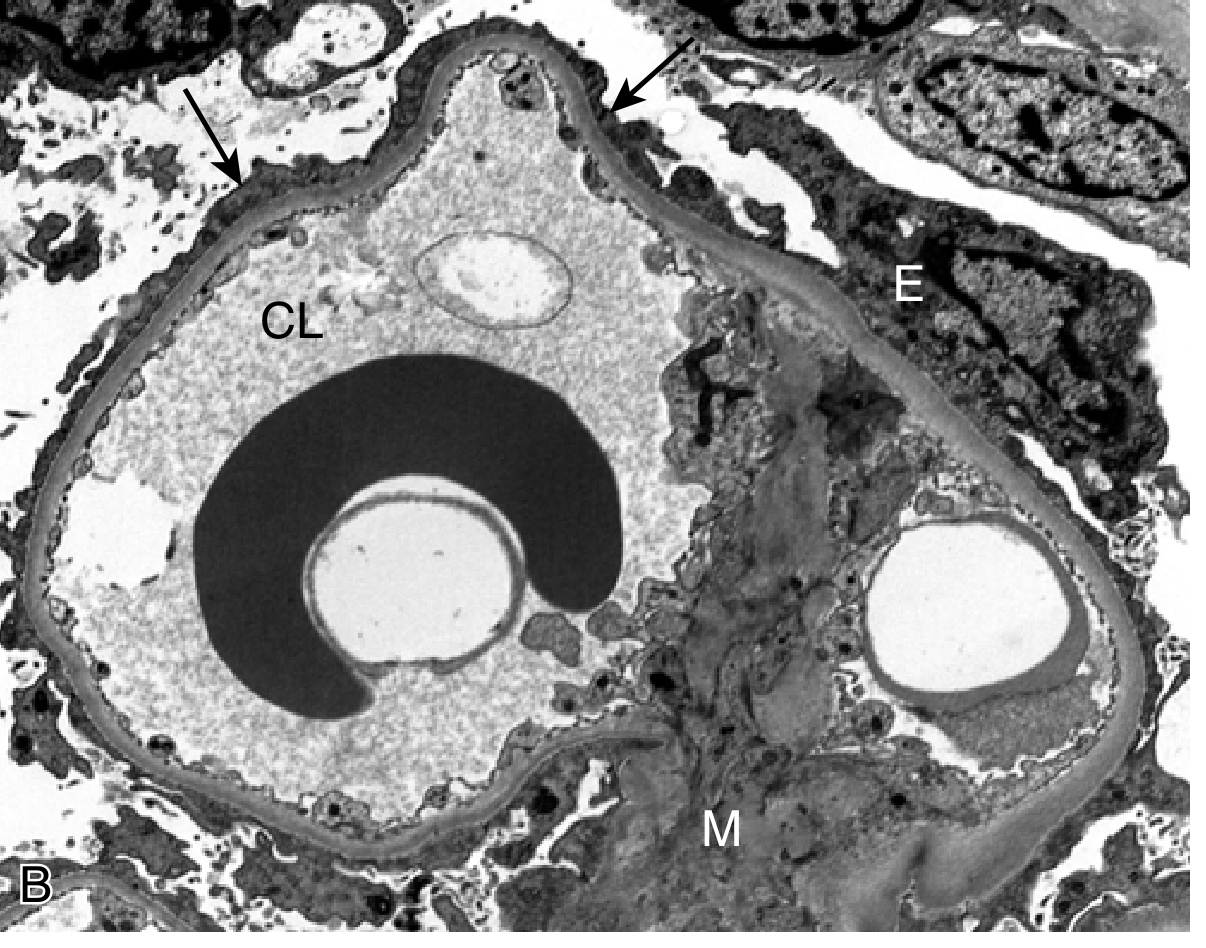
EM of minimal change disease: Arrows point to effaced foot processes. CL = capillary lumen, E = epithelial cell, M = mesangium - Robbins & Kumar Basic Pathology, Fig. 12.4B
Immunofluorescence
- Negative in MCD (no deposits of IgG, IgM, IgA, or complement)
- Sometimes subtle, diffuse fine granular IgM staining may be seen
- Recent work shows IgG staining colocalizing with clustered nephrin (anti-nephrin antibodies) in a subset
Pathogenesis (MCD)
The current leading hypothesis is autoantibody-mediated:
- Circulating anti-nephrin antibodies directed against nephrin - a transmembrane podocyte protein and essential slit diaphragm component
- These antibodies cause podocyte injury via interference with nephrin crosslinking
- This leads to rapid breakdown of the podocyte slit diaphragm
- Diffuse foot process effacement follows
- Massive, highly selective proteinuria results (mainly albumin - "selective proteinuria")
- Tubular cells absorb leaked lipoproteins → lipid-laden tubular cells → gross pale appearance
Earlier hypotheses invoked T-cell dysfunction with circulating permeability factors (IL-13, IL-4), increased podocyte CD80 expression, and dysregulated T-cell interactions.
Clinical Features
| Feature | Detail |
|---|---|
| Age | Children 2-6 yrs most common; adults also affected |
| Proteinuria | Massive (>3.5 g/day); average 10 g/24h in MCD |
| Selectivity | Highly selective (mainly albumin) |
| Hematuria | Absent (acellular sediment) |
| Hypertension | Uncommon in children (~30%); variable in adults |
| Renal function | Usually preserved |
| Serum albumin | Severely low (hypoalbuminemia) |
| Hyperlipidemia | Present (compensatory liver synthesis) |
| Edema | Prominent (periorbital in children, dependent edema) |
| Steroid response | Excellent - >90% of children respond within 8 weeks |
Summary Table
| Feature | Finding |
|---|---|
| Gross | Large, pale/white, smooth, waxy kidney |
| Cause of pallor | Lipid/protein-laden tubular cells |
| Light microscopy | Normal glomeruli; lipid in tubules |
| EM | Diffuse foot process effacement; no deposits |
| IF | Negative (or faint IgM/IgG) |
| Proteinuria | Selective (albumin-predominant) |
| Classic disease | Minimal change disease (lipid nephrosis) |
| Treatment | Corticosteroids (>90% response in children) |
Sources:
- Robbins & Kumar Basic Pathology, Minimal Change Disease section
- Robbins, Cotran & Kumar Pathologic Basis of Disease, Morphology of MCD (p. 846)
- Harrison's Principles of Internal Medicine 22E, MCD section
This is a shared conversation. Sign in to Orris to start your own chat.