Ecg
Asking for Preferences
Reading File
Finding Sources
Searching Images
ECG electrocardiogram basic waves intervals interpretation
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Searching Images
ECG waveform diagram P wave PR interval QRS T wave labeled
Reading File
Reading File
Now I have excellent source material. Let me compile a comprehensive ECG basics guide.
ECG Basics & Interpretation
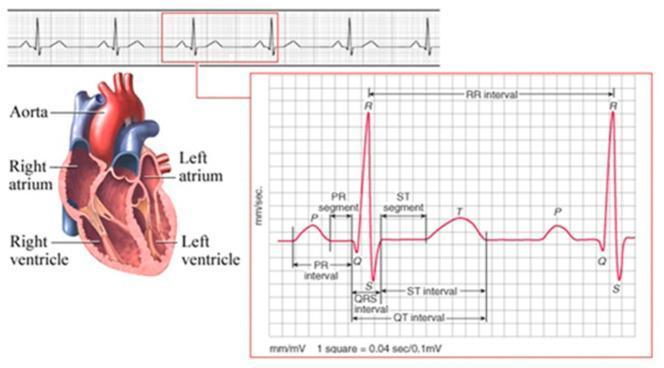
What is an ECG?
The electrocardiogram (ECG/EKG) records the electrical activity of the heart from the body surface. It is recorded on grid paper at a standard speed of 25 mm/sec, with:
- Horizontal axis = time (1 small box = 0.04 sec; 1 large box = 0.2 sec)
- Vertical axis = voltage (1 small box = 0.1 mV; 10 mm = 1 mV)
The ECG Waveforms
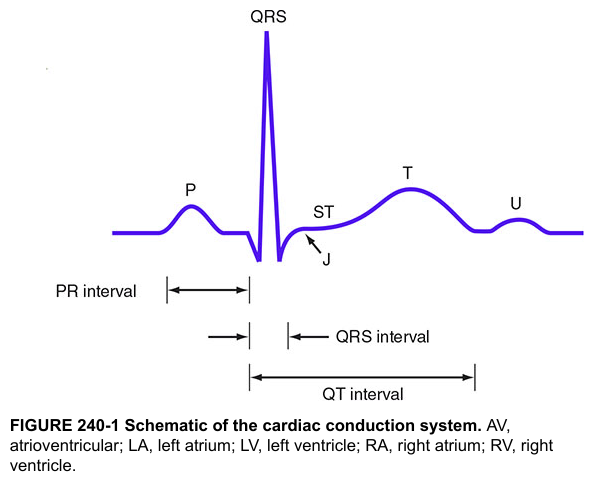
| Wave/Segment | Represents |
|---|---|
| P wave | Atrial depolarization (SA node → atrial muscle) |
| PR interval | Conduction delay through atria, AV node, His-Purkinje system |
| QRS complex | Ventricular muscle depolarization |
| ST segment | Early ventricular repolarization (isoelectric baseline normally) |
| T wave | Ventricular repolarization |
| U wave | Small deflection after T wave (same polarity; mechanism uncertain) |
| J point | Junction between end of QRS and start of ST segment |
The QRS is much larger than the P wave because ventricular muscle mass far exceeds atrial mass. Atrial repolarization exists but is buried under the QRS. — Goldman-Cecil Medicine
Normal Intervals
| Interval | Measurement | Normal Value |
|---|---|---|
| PR interval | Start of P wave → start of QRS | 0.12–0.20 sec (3–5 small boxes) |
| QRS duration | Start → end of QRS complex | < 0.12 sec (< 3 small boxes) |
| QT interval | Start of QRS → end of T wave | Rate-dependent; corrected QTc ≤ 440 ms (men), ≤ 460 ms (women) |
| R-R interval | Between two consecutive QRS complexes | = one cardiac cycle duration |
Heart Rate Calculation
Quick method (regular rhythm):
$$\text{HR} = \frac{300}{\text{Number of large boxes between R-R}}$$
| Large boxes between R waves | Heart rate |
|---|---|
| 1 | 300 bpm |
| 2 | 150 bpm |
| 3 | 100 bpm |
| 4 | 75 bpm |
| 5 | 60 bpm |
| 6 | 50 bpm |
For irregular rhythms, count QRS complexes in a 10-second rhythm strip × 6.
The 12-Lead System
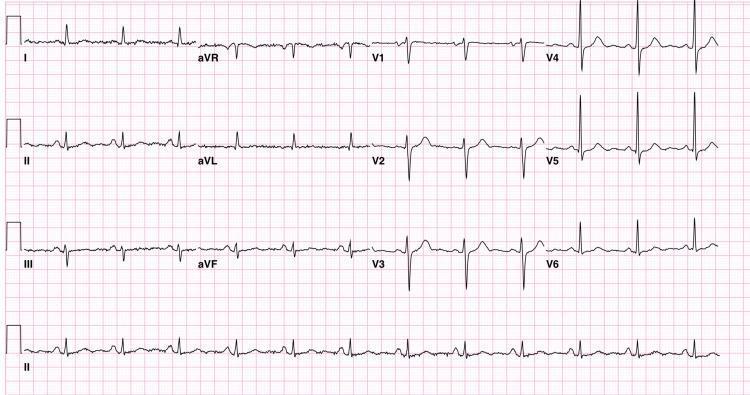
The standard ECG has 12 leads, each viewing the heart's electrical activity from a different angle:
| Group | Leads | Views |
|---|---|---|
| Limb leads | I, II, III | Frontal plane |
| Augmented limb leads | aVR, aVL, aVF | Frontal plane (enhanced) |
| Precordial leads | V1–V6 | Horizontal (transverse) plane |
Regional groupings for ischemia:
- Inferior: II, III, aVF (RCA territory)
- Lateral: I, aVL, V5, V6 (LCx territory)
- Anterior/Septal: V1–V4 (LAD territory)
- aVR: "looks into" the right side of the heart; ST elevation in aVR may indicate left main or proximal LAD occlusion
Systematic ECG Interpretation — The 8-Step Approach
- Rate — Calculate HR (normal: 60–100 bpm)
- Rhythm — Regular or irregular? Is each QRS preceded by a P wave?
- P waves — Present, upright in II, inverted in aVR? Morphology normal?
- PR interval — 0.12–0.20 sec? Constant?
- QRS duration — < 0.12 sec (narrow = supraventricular; wide = bundle branch block or ventricular origin)?
- Axis — Normal (−30° to +90°); LAD or RAD?
- ST segments & T waves — Elevation, depression, inversion?
- QT interval — Prolonged or shortened?
Cardiac Conduction System (the anatomy behind ECG)
The cardiac conduction system initiates and coordinates contraction through four components:
- Sinoatrial (SA) node — pacemaker; located at the junction of the superior vena cava and right atrium; generates the P wave
- Atrioventricular (AV) node — delays conduction (~120 ms); represents most of the PR interval
- Bundle of His + Left/Right bundle branches — carries impulse to the ventricles rapidly
- Purkinje fibers — spreads excitation throughout the ventricular myocardium apex-to-base → produces the QRS
A unidirectional wave of excitation moves from the papillary muscles and apex of the ventricles to the arterial outflow tracts. — Gray's Anatomy for Students
Common ECG Abnormalities at a Glance
| Finding | Cause |
|---|---|
| PR > 0.20 sec | First-degree AV block |
| Wide QRS (> 0.12 sec) | Bundle branch block, hyperkalemia, WPW, ventricular rhythm |
| ST elevation | MI (STEMI), pericarditis, Brugada, early repolarization |
| ST depression | Ischemia, digoxin effect, reciprocal changes |
| Tall peaked T waves | Hyperkalemia (early sign at K⁺ >6 mEq/L) |
| QT prolongation | Drug toxicity, electrolyte disturbances (↓K⁺, ↓Mg²⁺, ↓Ca²⁺), congenital LQTS |
| J wave (Osborn wave) | Hypothermia, hypercalcemia, idiopathic VF risk |
Ion Channel Basis of the ECG
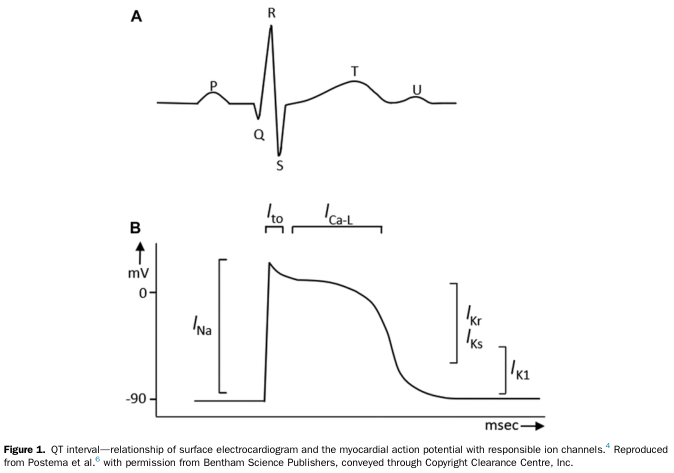
The QRS corresponds to rapid depolarization (I_Na — sodium influx), the plateau phase to I_Ca-L (calcium current), and the T wave to repolarization via I_Kr/I_Ks (potassium currents). This is why drugs blocking these channels (antiarrhythmics, antipsychotics, antibiotics) can prolong the QT interval and risk torsades de pointes.
Sources: Goldman-Cecil Medicine; Medical Physiology (Boron & Boulpaep); Gray's Anatomy for Students; Katzung's Basic & Clinical Pharmacology; Harrison's Principles of Internal Medicine
This is a shared conversation. Sign in to Orris to start your own chat.