Developmental dysplasia of hip
Reading File
Finding Sources
Finding Sources
Searching PubMed
"developmental dysplasia of the hip"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive content from multiple authoritative textbooks with images. Let me compile the complete, well-structured answer.
Developmental Dysplasia of the Hip (DDH)
Definition
DDH describes a spectrum of hip abnormalities ranging from mild acetabular dysplasia with a stable hip to complete irreducible dislocation of the femoral head from the true acetabulum. The term "developmental" replaced the older "congenital dislocation of the hip" because dislocation can develop weeks or months after a normal neonatal examination - the condition is not always present at birth.
The spectrum includes:
-
Acetabular dysplasia - shallow acetabulum, head in joint but poorly covered
-
Subluxation - partial displacement of the femoral head
-
Dislocation - complete displacement of femoral head from the true acetabulum (reducible vs. irreducible)
-
Teratologic dislocation - a separate entity, dislocated in utero, irreducible at birth, associated with neuromuscular conditions
-
Campbell's Operative Orthopaedics 15th Ed 2026, p. 1403
-
Bailey and Love's Short Practice of Surgery 28th Ed, p. 637
Incidence
| Measure | Rate |
|---|---|
| Neonatal hip instability (clinical exam) | ~20 per 1000 live births |
| True dislocation | ~2 per 1000 live births |
| Orthopaedic screening (pooled) | ~11.5 per 1000 |
| Ultrasound screening (all) | up to 55 per 1000 initially, settling to ~5 per 1000 on repeat |
Left hip is more commonly involved than the right; bilateral > isolated right-sided involvement. Many neonatal instabilities resolve spontaneously.
Risk Factors / Aetiology
Mnemonic: "Female Breech Firstborn Families"
| Risk Factor | Detail |
|---|---|
| Female sex | 4-5x more common in girls; possibly due to peripartum hormonal joint laxity (relaxin) |
| Breech presentation | Especially frank/extended breech; combination of female + breech gives ~2.8% DDH rate |
| Birth order | More common in firstborns (tight primigravid uterus restricts movement); left hip affected due to left occiput anterior position |
| Family history | Positive FHx raises risk to ~10%; autosomal dominant tendency |
| Oligohydramnios | Restricts fetal movement and positioning |
| Swaddling with legs adducted | Cultural/postnatal factor - worsens instability |
| Associated anomalies | Congenital muscular torticollis (~8% coexistence), metatarsus adductus, talipes calcaneovalgus |
| Race | Higher in Navajo; lower in Chinese; higher in communities practicing tight swaddling |
DDH associated with neuromuscular disease (e.g. arthrogryposis, cerebral palsy, myelomeningocele) is called teratologic dislocation - these hips are resistant to simpler treatments.
- Bailey and Love's, p. 637; Campbell's, p. 1404
Pathology / Secondary Changes
In a newborn, the femoral head can often be reduced and dislocated. As the child grows without treatment:
- Adductor musculature develops contracture - limiting abduction
- The acetabulum becomes shallower (true acetabulum fills with fibrofatty tissue - the pulvinar)
- The labrum becomes hypertrophied, inverted, and may obstruct reduction (limbus)
- The femoral head migrates superiorly and posteriorly; a false acetabulum (pseudoacetabulum) forms
- The femoral neck develops increased anteversion
- The joint capsule becomes hourglass-shaped
Clinical Features by Age
Neonate (0-3 months)
- Ortolani test (reduction test): Hip is dislocated. Flex hips and knees to 90°, stabilize pelvis, then abduct and lift the greater trochanter anteriorly - a palpable clunk of reduction = positive (reducible dislocation)
- Barlow test (provocation test): Hip is in joint. Adduct the flexed hip and apply posterior pressure - a palpable clunk of dislocation = positive (dislocatable hip)
Key: A clunk (palpable) is significant. A click (audible only) is nonspecific and not diagnostic.

Infant (3-18 months)
- Limited hip abduction (most reliable sign) - due to adductor contracture; compare sides
- Asymmetric thigh/inguinal skin folds (unreliable alone - normal infants can have asymmetry)
- Galeazzi sign (Allis sign): With hips and knees flexed to 90°, apparent femoral length discrepancy - positive for unilateral dislocation
- Limb shortening (telescoping may be present)
Walking Child (>12-18 months)
- Trendelenburg gait (lurching to affected side)
- Waddling gait in bilateral cases
- Lumbar lordosis - compensation for bilateral hip flexion contracture
- Unilateral toe-walking (apparent leg shortening)
- Limited abduction in flexion
Adolescent/Adult
- Exercise-induced hip/groin pain (sometimes referred to the knee)
- Progressive osteoarthritis if untreated - a major cause of OA in young adults
Diagnosis
Neonatal Clinical Screening
The neonatal clinical examination must answer:
- Is the hip dislocated?
- If dislocated - is it reducible (Ortolani +) or not (Ortolani -)?
- If not dislocated - is it dislocatable (Barlow +)?
- If clinically normal - do risk factors demand ultrasound?
Ultrasound (USG) - Investigation of choice in infancy
- Modality of choice from birth up to ~9-12 months (before ossification of the femoral head)
- High-frequency linear probe; coronal view; infant in lateral decubitus, hip flexed and abducted
- Performed at 4-6 weeks for screening; selective use for "at-risk" infants
- Graf classification is standard:
| Graf Type | Description | Alpha Angle | Management |
|---|---|---|---|
| Type I | Normal | ≥60° | Normal |
| Type IIa | Physiologically immature (<3 months) | 50-59° | Observe |
| Type IIb | Delayed ossification (>3 months) | 50-59° | Harness |
| Type IIc | Critical range | 43-49° | Harness |
| Type III | Subluxed | <43° | Treatment |
| Type IV | Dislocated | Any | Treatment |
The alpha (α) angle measures bony acetabular coverage; Morin index (% femoral head coverage) <50% = likely unstable.
Dynamic stress views can demonstrate dislocatability.
Plain Radiograph - From 4-5 months onwards
Once the femoral head ossifies, X-ray becomes useful. Key reference lines on AP pelvis:
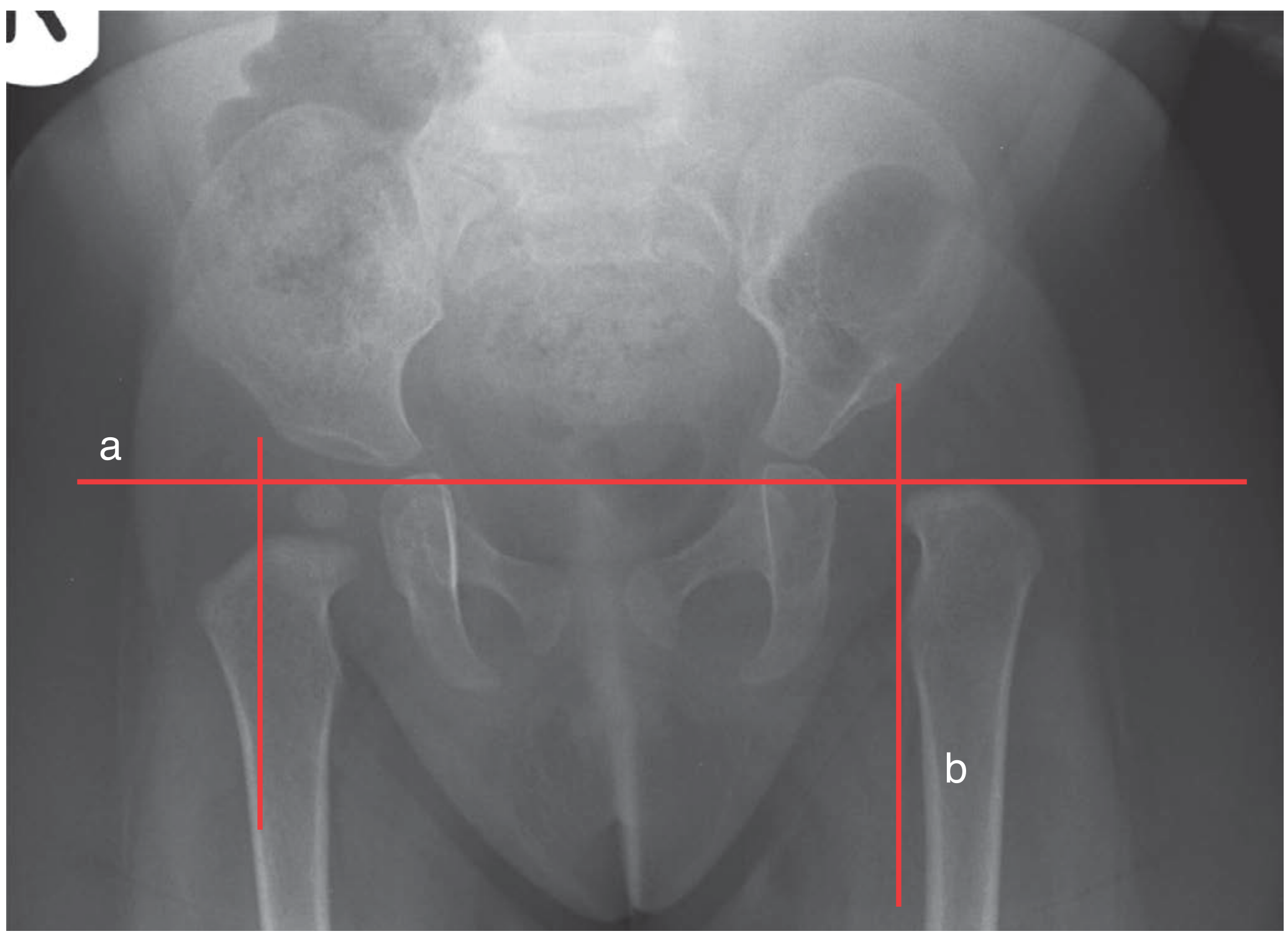
- Hilgenreiner's line (H-line): Horizontal line through both triradiate cartilages
- Perkins' line (P-line): Vertical line through the lateral edge of the acetabulum, perpendicular to H-line
- Normal: femoral head (or metaphyseal beak) in the inner lower quadrant
- DDH: femoral head in the outer or upper quadrant
- Shenton's line: Disrupted in dislocation (normally a smooth arc from femoral neck to superior pubic ramus)
- Acetabular index: Normal ≤30° in newborns, ≤25° by 6 months; elevated = dysplasia
- IHDI grading: Refined classification of dislocation severity
CT/MRI
- Used post-operatively to assess concentric reduction (especially after spica casting)
- MRI is preferred to avoid radiation in children
- Useful if clinical concern persists after operative treatment
Treatment - Age-Based Algorithm
The primary goal is stable, concentric reduction of the femoral head into the true acetabulum.
Birth to 6 weeks
Many unstable hips in the first 2-3 weeks resolve spontaneously - observation is appropriate for mild instability. Pavlik harness if no spontaneous improvement.
0-6 months: Pavlik Harness
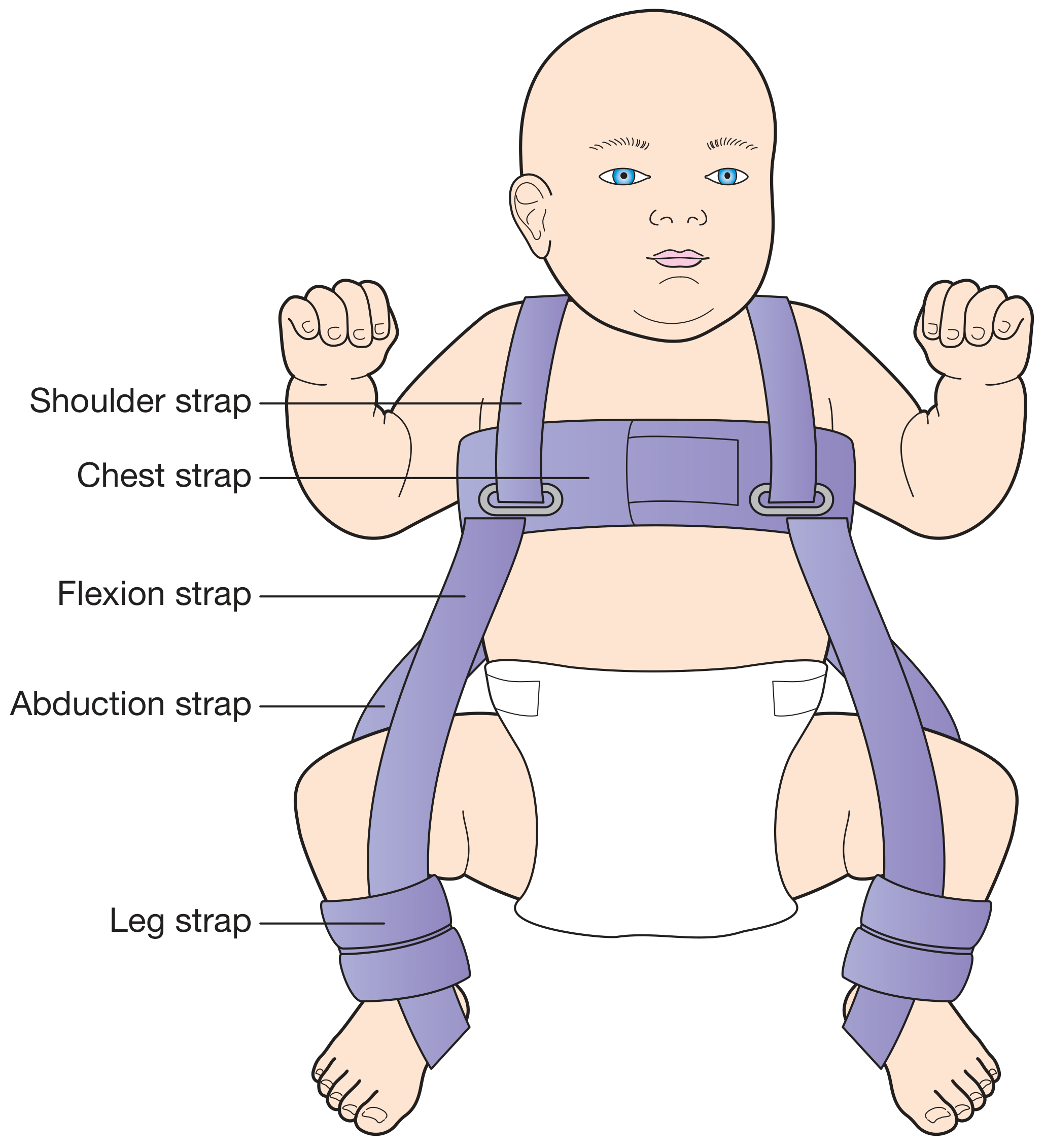
- First-line treatment for DDH in infants up to 4-6 months
- Holds hip in flexion (~100°) and abduction (gentle); anterior strap controls flexion, posterior strap limits adduction and encourages abduction
- Worn full-time for 6-12 weeks, then weaned
- Success rate: ~85-90% for dislocatable hips; lower for true dislocation
- Complications: Avascular necrosis (AVN) of femoral head (avoid extreme flexion >110° and forced abduction), femoral nerve palsy (from excessive flexion)
- Harness treatment is unusual to succeed after 4-6 months
6-18 months: Closed or Open Reduction
If harness fails or patient presents late:
-
Examination Under Anaesthesia (EUA) + Arthrogram + Closed Reduction
- Check for obstacles to reduction (inverted labrum, pulvinar, hourglass capsule, tight psoas/adductors)
- Adductor ± psoas tenotomy if blocking reduction
- Achieve reduction, confirm with arthrogram
- Hip spica cast (human position ~100° flexion, 45° abduction) for 3 months
-
Open Reduction (if closed fails or hip irreducible)
- Medial approach (Ludloff): 6-24 months; direct access to medial structures blocking reduction; capsulorrhaphy not possible
- Anterior approach (Smith-Petersen): from 9-12 months; allows simultaneous capsulorrhaphy and acetabular work
- Followed by spica cast
18 months - 4 years: Open Reduction + Pelvic Osteotomy
Acetabular remodeling is limited; femoral anteversion and acetabular dysplasia must be addressed surgically:
- Pelvic (acetabular) osteotomies - redirect the acetabulum:
- Salter osteotomy: Single innominate; redirects acetabulum anteriorly and laterally; up to ~4 years
- Pemberton osteotomy: Incomplete periarticular; reduces acetabular volume; useful for large dysplastic acetabulum
- Dega osteotomy: Posterolateral coverage; useful in neuromuscular DDH
- Triple osteotomy (Tonnis, Steel, Ganz PAO): For older children and adults with open triradiate cartilage closed
- Femoral osteotomy (derotation + varus shortening): Reduces tension on femoral head, corrects anteversion; shortening reduces risk of AVN
- Combined pelvic + femoral osteotomy is often needed for older children
Adults / Young Adults with Residual Dysplasia
- Periacetabular Osteotomy (Bernese PAO): Redirects acetabulum in all planes; gold standard for symptomatic dysplasia in adults with preserved cartilage
- Total Hip Arthroplasty: For end-stage OA - technically challenging due to deficient bone stock and altered anatomy
Complications of Treatment
| Complication | Notes |
|---|---|
| Avascular necrosis (AVN) of femoral head | Most serious; results from excessive pressure, forced abduction, or vascular compromise; seen with any intervention |
| Redislocation | Failure of reduction or harness |
| Residual acetabular dysplasia | May need osteotomy |
| Femoral nerve palsy | Excessive flexion in Pavlik harness |
| Osteoarthritis | Late sequela of untreated or inadequately treated DDH |
Complications of Untreated DDH
- Progressive acetabular dysplasia
- Formation of a false acetabulum (pseudoacetabulum)
- Premature hip osteoarthritis - a major cause of total hip replacement in adults under 50
- Leg length discrepancy
- Lumbar spondylosis (compensatory)
Screening Summary (AAOS Guidelines)
-
Universal ultrasound screening: Not supported by moderate evidence
-
Selective ultrasound (before 6 months): Recommended for breech presentation, family history, or clinical instability
-
AP pelvic radiograph: Useful from 4 months onwards as an alternative to ultrasound
-
Serial examinations: Until 6 months of age in all at-risk infants
-
Campbell's Operative Orthopaedics 15th Ed 2026; Bailey and Love's Short Practice of Surgery 28th Ed; Grainger & Allison's Diagnostic Radiology; Schwartz's Principles of Surgery 11th Ed
Recent evidence update: A 2025 meta-analysis (PMID 39853978) confirmed breech position and female sex as the strongest risk factors for DDH before 3 months of age. A 2026 genetic study (PMID 41912496) identified novel genes associated with DDH, supporting a strong genetic component - consistent with the clinical finding that family history raises risk to ~10%.
This is a shared conversation. Sign in to Orris to start your own chat.