leptospirosis
Reading File
Finding Sources
Searching PubMed
leptospirosis
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
I now have a thorough, well-illustrated body of content to synthesize a comprehensive answer. Here it is:
Leptospirosis
The Organism
Leptospirosis is a zoonotic infection caused by pathogenic spirochetes of the genus Leptospira. The name comes from Greek: leptos (thin) + speira (coil). These bacteria are 0.1 µm wide and 6-20 µm long, with a characteristic hooked trailing end that inspired the naming of the principal pathogenic species, L. interrogans (its shape resembles a question mark).
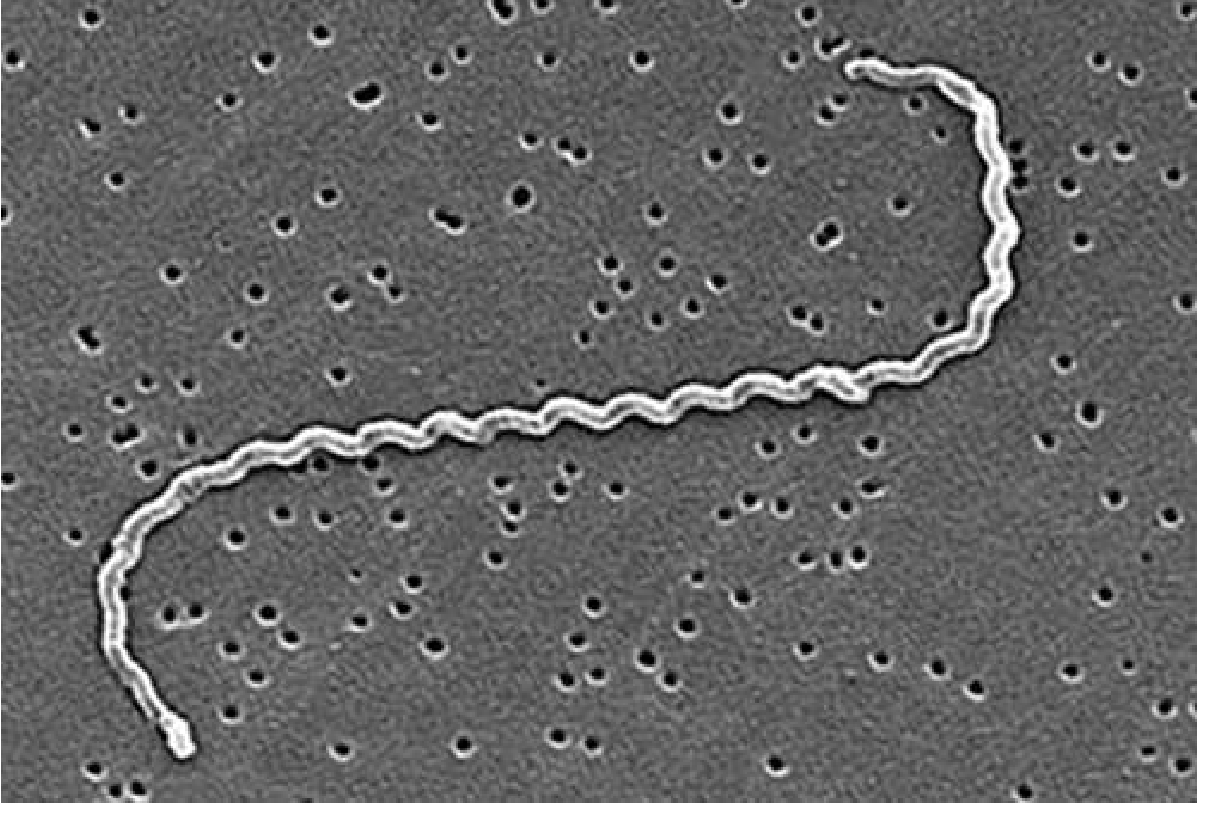
There are >64 species, with 25+ serogroups and 250+ serovars. Leptospiral genomes show extensive horizontal gene transfer, facilitating adaptation to diverse ecologic niches. The organism is not stained by Gram's method.
Epidemiology
Leptospirosis is the world's most common zoonosis, causing approximately 1 million clinical infections and 58,900 deaths annually - with the true burden likely underestimated due to frequent misdiagnosis as dengue, malaria, or influenza.
Reservoir hosts: Rodents (especially the urban brown rat Rattus norvegicus), cattle, dogs, pigs, horses. Animals become chronically infected - leptospires colonize renal tubules and are shed persistently in urine into soil and water.
Human transmission routes:
- Contact with water or soil contaminated with infected animal urine
- Entry via broken skin, conjunctiva, or upper alimentary mucosa
- Occupational: farmers, veterinarians, slaughterhouse workers, sewer workers, garbage collectors
- Recreational: swimming/wading in contaminated water bodies
Geographic distribution: Endemic in tropical developing countries (India, Malaysia, Brazil). Urban outbreaks spike during heavy rainfall and flooding when rodents are displaced and leptospires wash into floodwaters. Risk is increasing with climate change-driven extreme rainfall events.
Independent risk factors include flooding, lacerated wounds, and contact with livestock. About half of fatalities occur in young adult males.
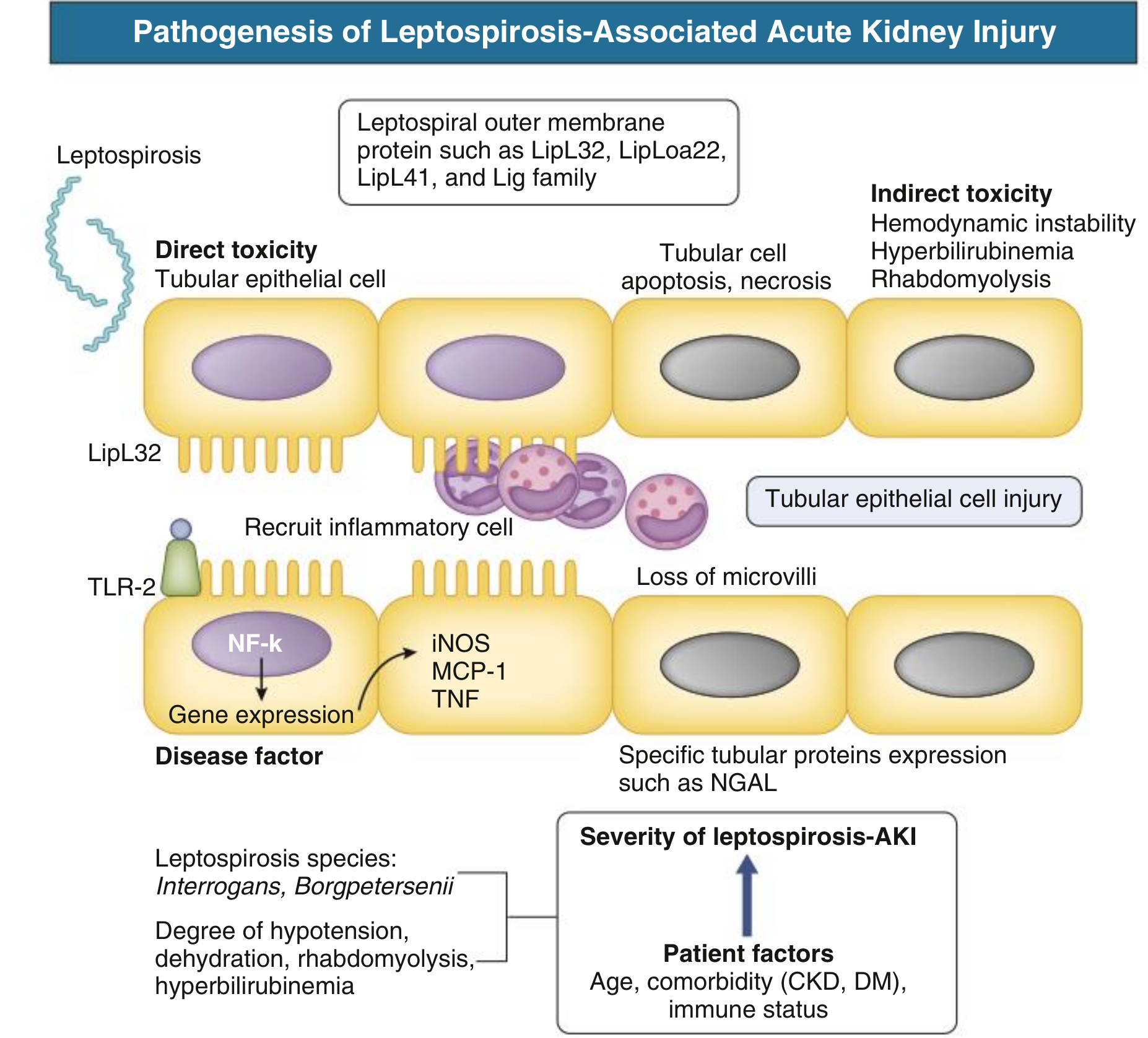
Pathogenesis
The organism enters through small skin breaks, conjunctiva, or upper alimentary mucosa. Active motility via periplasmic flagella facilitates tissue burrowing. The disease is biphasic:
Phase 1 - Leptospiremic phase (days 1-7):
- Bacteremia with dissemination to liver, kidney, CNS, lungs
- Leptospires evade the innate immune system through several mechanisms: outer membrane proteins bind LPS and peptidoglycan (shielding these from pattern recognition), and surface proteins bind complement regulators (resisting complement killing)
- Colonization of proximal renal tubules impairs Na+ and water reabsorption, causing potassium wasting and hypokalemia
- Hepatic sinusoidal invasion causes hepatocellular disruption and bile leakage (jaundice)
- Endothelial injury and impaired hemostasis lead to bleeding
Phase 2 - Immune phase (week 2+):
- Agglutinating antibodies appear; bacteremia clears
- Generalized immune activation may produce a sepsis-like syndrome
- Antimicrobials are less effective at this stage
- May manifest as aseptic meningitis, uveitis, or multiorgan failure
Clinical Manifestations
Incubation period: 6-29 days (median ~15 days).
Most infections are subclinical or mild and self-limited. Symptomatic disease ranges from an influenza-like illness to fulminant Weil disease.
Mild/Anicteric Leptospirosis (~90%)
- Abrupt onset: fever, rigors, severe headache (bifrontal/temporal, retro-orbital, with photophobia)
- Myalgia - characteristic and intense, especially calves and thighs
- Conjunctival suffusion (not purulent conjunctivitis - a key distinguishing sign)
- Nausea, vomiting, diarrhea
- Rash (less common)
- Fever typically resolves in ~1 week, may recur
Weil Disease (Severe Leptospirosis, ~5-10%)
The classic triad:
- Jaundice (deep, may be profound)
- Acute kidney injury (typically non-oliguric with hypokalemia)
- Bleeding (thrombocytopenia + coagulation disorders; petechiae to frank hemorrhage)

Additional severe features:
- Pulmonary hemorrhage / ARDS - severe pulmonary involvement is increasingly recognized as a cause of death
- Aseptic meningitis
- Uveitis (may occur weeks to months later, even after bacteremia has cleared)
- Myocarditis, arrhythmias
- Rhabdomyolysis
Renal specifics: AKI is almost universal in Weil disease. It is characteristically non-oliguric with hypokalemia (due to tubular potassium wasting). Histology shows interstitial nephritis with cellular infiltration. Long-term CKD can develop after leptospirosis-associated AKI.
Diagnosis
High index of suspicion is needed - the disease mimics dengue, malaria, viral hepatitis, and influenza.
| Method | Timing | Notes |
|---|---|---|
| PCR (serum/urine) | First week | High sensitivity early; test of choice for acute disease |
| Microscopic Agglutination Test (MAT) | After week 1 | Gold standard serology; requires paired sera (4x titer rise); lower sensitivity in first week |
| Blood culture (EMJH medium) | First week | Slow (weeks to grow); useful early in course |
| Urine culture | After week 1 | Positive later in course |
| Rapid IgM ELISA | After day 5-7 | Useful for field settings; less specific than MAT |
The THAI Leptospirosis Score and similar clinical scoring systems can help stratify patients when diagnostics are limited.
Treatment
Mild disease:
- Doxycycline 100 mg orally twice daily x 7 days
- Azithromycin (alternative, especially in pregnancy)
Severe disease:
- IV Penicillin G 1.5 million units q6h - traditional first-line
- IV Ampicillin or IV Ceftriaxone 1 g daily - equivalent efficacy, easier administration
- Early treatment is most effective; antibiotics given in the immune phase have limited impact on bacteremia but may reduce complications
Supportive care:
- Non-oliguric AKI with hypokalemia: aggressive IV fluid replacement + potassium supplementation
- Oliguric renal failure: prompt initiation of hemodialysis or peritoneal dialysis
- Pulmonary hemorrhage: mechanical ventilation, consider corticosteroids (see note below)
- Thrombocytopenia/bleeding: platelet transfusion as needed
Recent evidence note: A 2025 Cochrane systematic review (PMID 40704556) evaluated corticosteroids for leptospirosis treatment - this is relevant to the management of severe pulmonary hemorrhage cases, where corticosteroid use has been debated. Also, a 2025 meta-analysis (PMID 40111731) provides updated data on the incidence and outcomes of leptospirosis-associated kidney involvement.
Prevention
- Avoid wading through potentially contaminated floodwater; cover skin cuts and abrasions
- Doxycycline prophylaxis: 200 mg once weekly for high-risk exposure (e.g., military, flood rescue workers)
- Rodent control in urban environments
- Occupational protective equipment (waterproof boots, gloves)
- Vaccines: Available for livestock and dogs; human vaccines exist in some endemic countries (Cuba, China) but are serovar-specific and not widely available globally
Key "Don't Miss" Points
| Feature | Clinical significance |
|---|---|
| Conjunctival suffusion | Characteristic, non-purulent redness - key distinguishing sign |
| Non-oliguric AKI + hypokalemia | Paradoxical but typical - replace K+ aggressively |
| Pulmonary hemorrhage | Leading cause of death in severe disease |
| Uveitis | May occur weeks-months after apparent recovery |
| Misdiagnosis as dengue | Both cause fever, headache, myalgia, thrombocytopenia in the same tropical settings |
Sources: Goldman-Cecil Medicine, Sherris & Ryan's Medical Microbiology 8e, Comprehensive Clinical Nephrology 7e, Brenner & Rector's The Kidney
This is a shared conversation. Sign in to Orris to start your own chat.