Korsokoff psychosis
Reading File
Finding Sources
Finding Sources
Searching PubMed
Korsakoff syndrome thiamine
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Here is a thorough overview of Korsakoff psychosis (Korsakoff syndrome) drawn from multiple authoritative textbooks.
Korsakoff Syndrome (Korsakoff Psychosis)
Terminology
The terms Korsakoff psychosis, Korsakoff dementia, and Korsakoff syndrome have historically been used interchangeably. Modern texts prefer "Korsakoff syndrome" or "amnesic syndrome," as the word "psychosis" is misleading - the patient is typically alert, not psychotic. It is now formally classified under alcohol-induced major neurocognitive disorder, amnestic-confabulatory type (DSM-5). When it follows Wernicke encephalopathy (as it usually does), the combined disorder is called Wernicke-Korsakoff syndrome.
- Adams and Victor's Principles of Neurology, 12th Edition, p. 457
History
-
1881: Carl Wernicke described acute confusion, ophthalmoplegia, and gait ataxia.
-
1889: Sergei Korsakoff described a chronic syndrome of polyneuritis, anterograde amnesia, and confabulation in patients with chronic alcohol use, but did not link it to Wernicke's findings.
-
The clinical connection was made ~10 years later by other investigators.
-
The thiamine-deficiency etiology was established in the early 1930s. The diencephalic lesion was characterized by Maurice Victor in the 1960s.
-
Bradley and Daroff's Neurology in Clinical Practice, p. 1802
Pathophysiology
Cause: Thiamine (Vitamin B1) Deficiency
Thiamine pyrophosphate (TPP), the active form, is required for three key enzymatic reactions in glucose metabolism and neurotransmitter synthesis (including acetylcholine). Deficiency leads to:
- Cerebral energy dysfunction
- Breakdown of the blood-brain barrier
- Altered glutamate neurotransmission and NMDA receptor-mediated excitotoxicity
- Accumulation of toxic metabolites
Alcohol-related thiamine deficiency arises through:
- Dietary insufficiency / malnutrition
- Folate deficiency reducing GI thiamine absorption
- Direct damage to intestinal mucosa
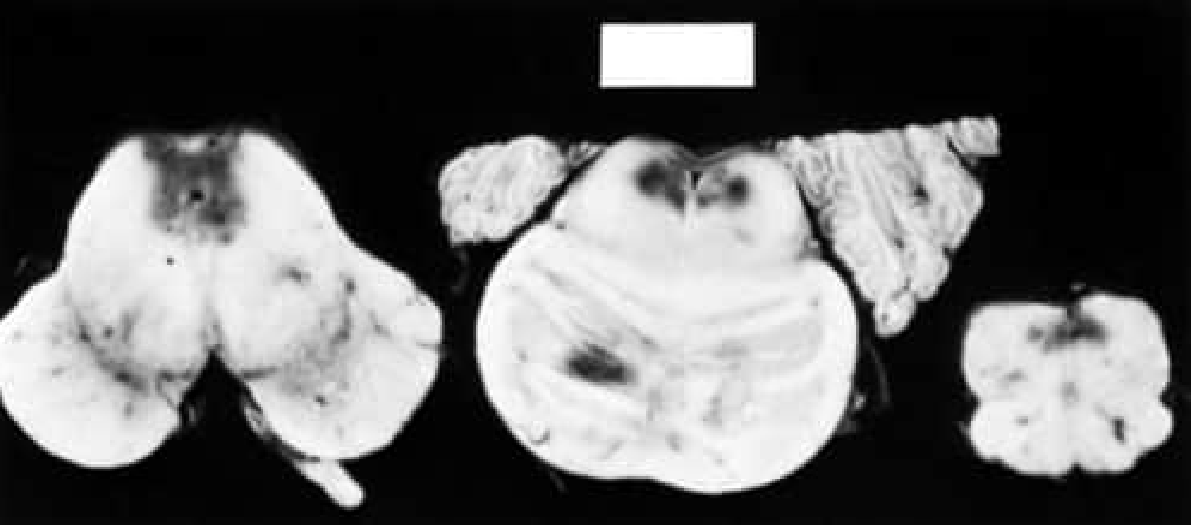
Structural Lesions (Anatomic Basis)
The hallmark is symmetric periventricular damage, especially:
- Medial thalami (mammillothalamic tract, dorsomedial nucleus)
- Mammillary bodies (most classic finding)
- Periaqueductal gray matter
- Walls of the third and fourth ventricles
Memory dysfunction reflects the predilection for the diencephalon and temporal lobes. Any injury to these regions (infarction, trauma, tumor, herpes simplex encephalitis) can produce an indistinguishable syndrome.
Etiology: Who Gets It?
Most common: chronic alcoholism (>20 years of use, usually >40 years of age).
Non-alcoholic causes (any state of nutritional insufficiency):
- Hyperemesis gravidarum
- Bariatric surgery
- Anorexia nervosa
- Cancer / chemotherapy
- HIV/AIDS
- Long-term dialysis
- Prolonged IV feeding / refeeding syndrome
- Congestive heart failure treated long-term with furosemide (reduces renal tubular thiamine reabsorption)
- Thyrotoxicosis, hypomagnesemia
Precipitant: IV glucose administration to a malnourished patient can acutely exhaust thiamine stores and precipitate Wernicke encephalopathy.
- Bradley and Daroff's Neurology in Clinical Practice, p. 1802; Kaplan & Sadock's Comprehensive Textbook of Psychiatry
Clinical Features
Relationship to Wernicke Encephalopathy
Korsakoff syndrome typically emerges as Wernicke encephalopathy resolves - as the ocular signs and acute confusion improve, the amnesic syndrome becomes apparent. However, some cases arise without a clinically apparent Wernicke phase.
Core Features of Korsakoff Syndrome
The key features (from Adams and Victor) are:
| Feature | Description |
|---|---|
| Anterograde amnesia | Inability to form new memories (learning is severely impaired) |
| Retrograde amnesia | Impaired recall of events before illness onset |
| Temporal disorientation | Cannot locate past experiences in the correct time sequence |
| Confabulation | Filling memory gaps with fabricated or misplaced memories |
| Preserved consciousness | Patient is alert, attentive, and responsive |
| Preserved immediate recall | Can repeat a string of digits (working memory) |
| Relatively preserved other cognition | Concentration, spatial tasks, verbal/visual abstraction often intact |
The Ribot rule applies: remote memory is relatively better preserved than recent memory.
Confabulation - Details
Two types are recognized:
- Momentary (provoked): Partially remembered events misplaced in time, elicited by questioning
- Fantastic (spontaneous): Dramatic fabricated personal histories - more common in the acute phase
Confabulation is not obligatory for diagnosis. In chronic, stable Korsakoff syndrome, it often disappears.
- Adams and Victor's Principles of Neurology, 12th Edition, p. 457
What Korsakoff Syndrome is NOT
The disorder must be distinguished from:
- Delirium / confusional states (impaired attention/perception)
- Hysterical amnesia (loss of personal identity)
- Frontal lobe disease / depression (impaired volition/apathy)
- Dementia (broad cognitive loss, not isolated memory)
Epidemiology
- Prevalence: ~0.4% in France, up to ~2% in the USA, Scandinavia, and Australia
- Typically seen in patients over age 40
- Autopsy studies show clinical diagnosis is made in only ~20-25% of pathologically confirmed cases - significantly underdiagnosed
Investigation
MRI Brain (key investigation)
- T2/FLAIR signal abnormalities symmetrically distributed around:
- Periaqueductal regions and tectal plates
- Medial thalami
- Bilateral mammillary bodies
- Cerebellar vermis, pons, medulla, dentate nuclei (sometimes)
- Petechial hemorrhages on SWI sequences
- Contrast enhancement possible in acute phase
- Chronic residual finding: shrunken mammillary bodies
- CT scan is far less sensitive
Labs
- Serum thiamine level - depressed
- Erythrocyte transketolase activity - depressed
- Serum pyruvate - elevated
- CSF: normal or mildly elevated protein
Pathology
Macroscopic: congestion, petechial hemorrhages, shrinkage, and discoloration in periventricular structures.
Chronic: glial proliferation and myelin pallor.
Treatment
Acute Wernicke/Prevention of Korsakoff Syndrome
This is a medical emergency. Treatment must not wait for laboratory results.
- IV thiamine first, BEFORE glucose - giving glucose without thiamine can precipitate or worsen encephalopathy.
- Dose: 500 mg IV thiamine (higher doses needed to replete stores; lower doses like 2-3 mg may modify only ocular signs).
- Repeat IM/IV daily until normal diet resumes.
- Add magnesium (required as cofactor for thiamine activity).
- Replace all B vitamins (patients are usually deficient in multiple vitamins).
Prompt thiamine can prevent progression to irreversible Korsakoff amnesic syndrome.
Chronic Korsakoff Syndrome
-
Prognosis is poor: fewer than 20% recover entirely (Victor's series)
-
Recovery is delayed (weeks to months) and slow
-
Thiamine replacement arrests progression but does not reverse established structural damage
-
Long-term abstinence from alcohol and nutritional rehabilitation are central to management
-
Adams and Victor's Principles of Neurology, 12th Edition, p. 1170; Bradley and Daroff's Neurology, p. 1803
Summary Table
| Feature | Detail |
|---|---|
| Cause | Thiamine (B1) deficiency |
| Most common setting | Chronic alcoholism |
| Acute precursor | Wernicke encephalopathy |
| Classic triad of Wernicke | Confusion, ophthalmoplegia, ataxia |
| Core deficit of Korsakoff | Anterograde > retrograde amnesia |
| Hallmark sign | Confabulation |
| Key anatomy | Mammillary bodies, medial thalamus |
| MRI finding | Bilateral mammillary body and periaqueductal T2 signal change |
| Treatment | IV thiamine (500 mg) BEFORE glucose; magnesium |
| Prognosis | <20% full recovery once Korsakoff established |
This is a shared conversation. Sign in to Orris to start your own chat.