Can yiu explain about the steps during labour in details
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have everything needed for a comprehensive, well-illustrated answer. Here is the full detailed explanation:
Steps/Stages of Labour - A Detailed Guide
Labour is defined as the onset of regular, painful uterine contractions associated with progressive cervical effacement and dilation, ultimately resulting in delivery of the baby and placenta. By clinical convention, labour is divided into four stages.
Before Labour Begins: Prodromal Events
In the 2-4 weeks before true labour, several preparatory changes occur:
- Lightening: The fetal presenting part settles into the pelvis
- Braxton Hicks contractions: Irregular, painless uterine tightenings increase in frequency
- Cervical ripening: The cervix softens, shortens (effaces), and may begin to dilate slightly (1.8 cm in nulliparas; 2.2 cm in multiparas on average, in the final 3 days)
- Bloody show: The cervical mucous plug breaks free, often with slight bleeding, 1 week to 1 hour before true labour begins
True labour begins when Braxton Hicks contractions become organised, reaching 25-60 mmHg in strength, occurring every 15-20 minutes, and causing progressive cervical change. - Morgan & Mikhail's Clinical Anesthesiology, 7e
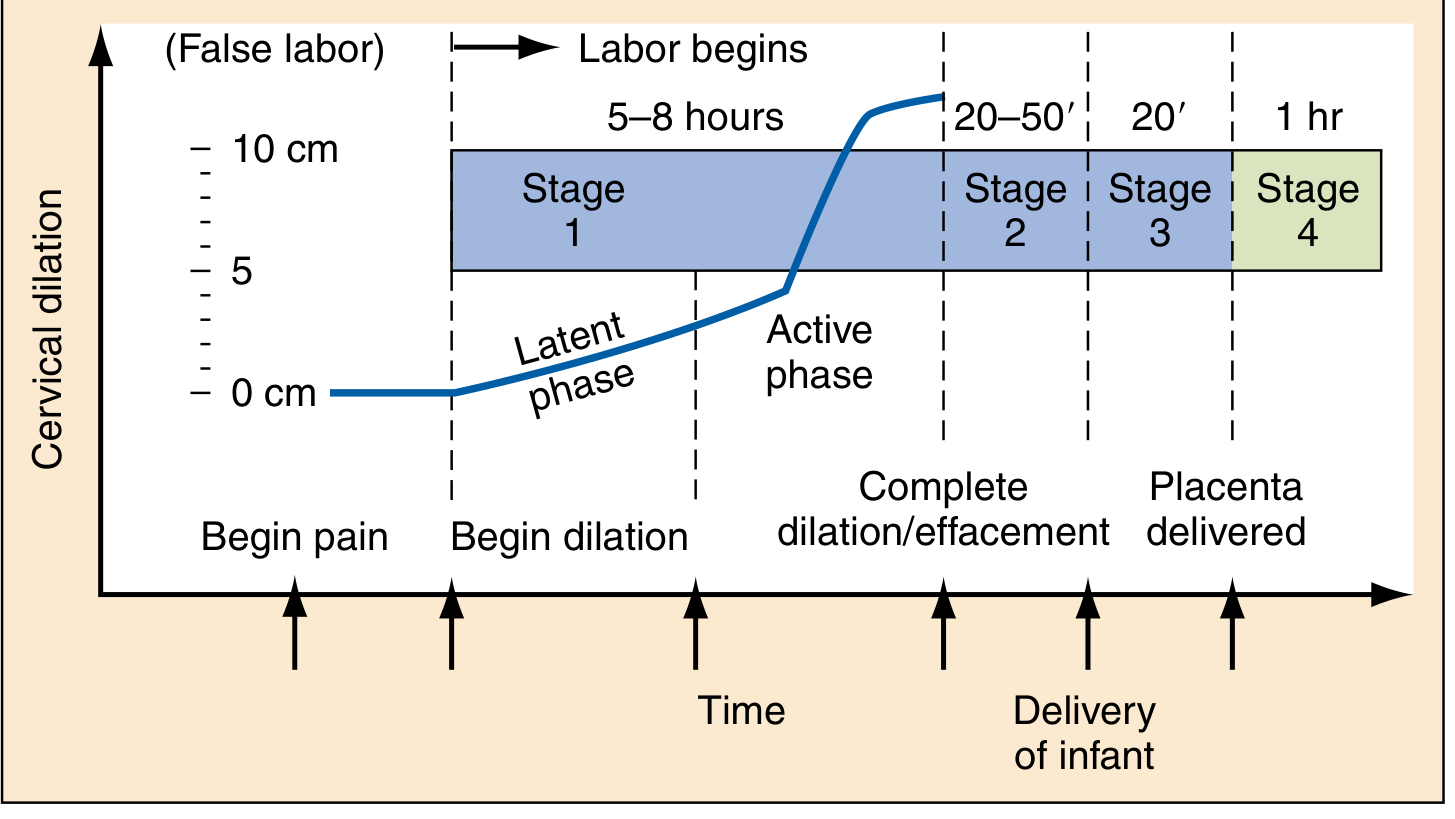
STAGE 1 - From Onset of Labour to Full Cervical Dilation (10 cm)
This is the longest stage. It is further subdivided into two phases:
Phase 1a: Latent Phase
- Begins with the onset of regular uterine contractions
- Slow, progressive cervical effacement and minor dilation (0 to ~2-4 cm)
- Contractions are relatively mild, often irregular
- Duration: Up to 20 hours in nulliparas (primiparas); up to 14 hours in multiparas
- This phase ends when the rate of cervical dilation begins to accelerate
Phase 1b: Active Phase
- Begins at approximately 3-4 cm of dilation
- Contractions become stronger, longer (up to 60 seconds), and more frequent (every 3-5 minutes)
- Cervical dilation accelerates rapidly up to 10 cm
- Total Stage 1 duration: 8-12 hours in nulliparas; 5-8 hours in multiparas
- Creasy & Resnik's Maternal-Fetal Medicine
Key cervical parameters assessed during Stage 1:
| Parameter | Description |
|---|---|
| Effacement | Thinning/shortening of the cervix; 100% = paper thin |
| Dilation | Opening of the cervical os, 0 to 10 cm |
| Station | Position of presenting part relative to ischial spines (−3 to +3) |
| Position | Relationship of fetal head to birth canal (usually occiput anterior) |
| Presentation | Part of fetus leading through the canal |
STAGE 2 - Full Dilation to Delivery of the Baby
Begins when the cervix reaches 10 cm and ends when the baby is born. The mother feels a strong urge to push.
Duration:
- Nulliparas: 20-50 minutes (up to 2-3 hours with epidural)
- Multiparas: typically shorter
The Cardinal Movements of Labour (Mechanism of Labour)
During Stage 2, the fetus makes a series of passive positional adjustments to navigate through the bony pelvis. These are called the cardinal movements:
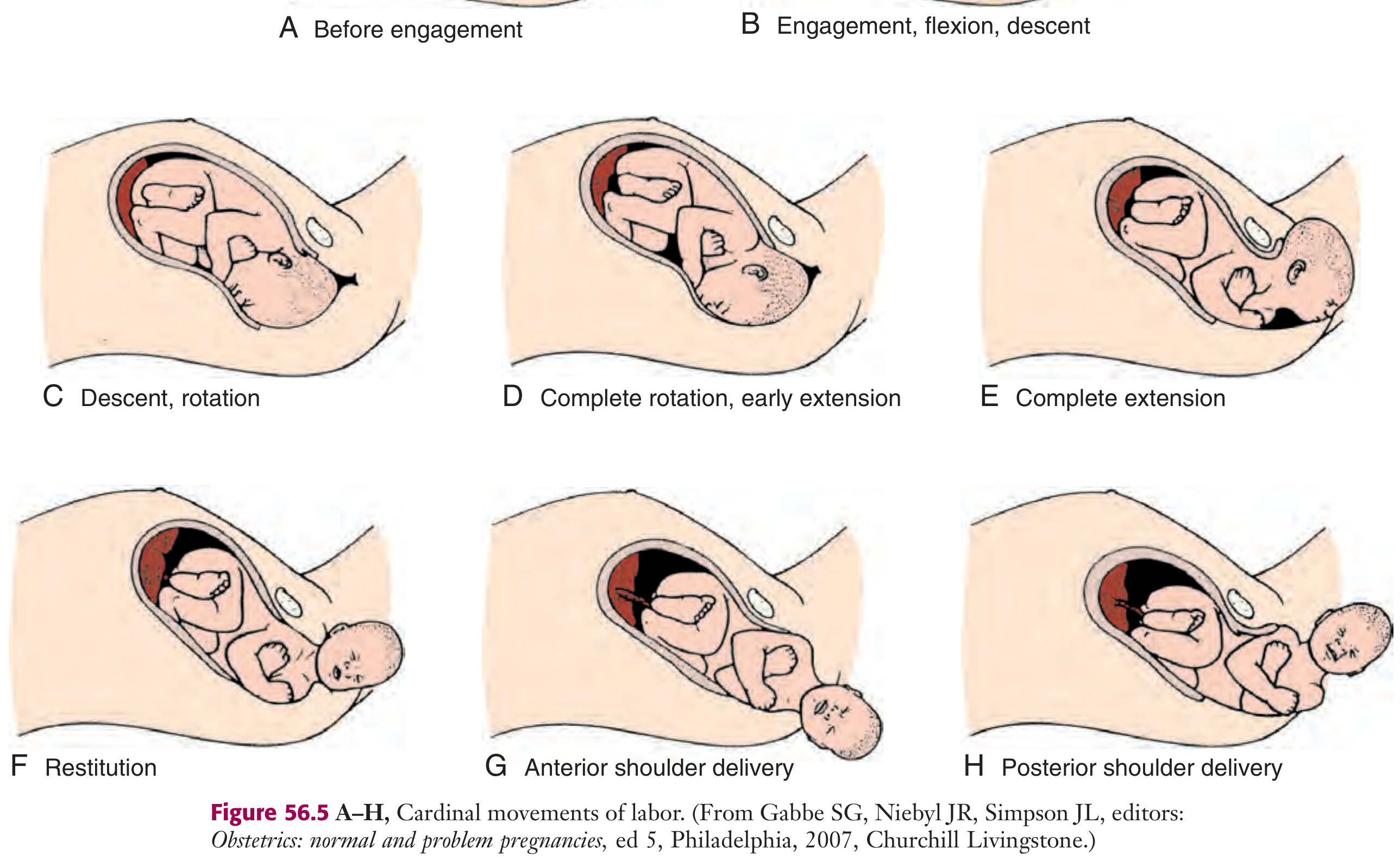
1. Engagement
The widest transverse diameter of the fetal head (biparietal diameter, ~9.5 cm) passes through the pelvic inlet. The fetus is "engaged" when the presenting part reaches 0 station. In nulliparas this usually occurs in the last 2 weeks of pregnancy; in multiparas it may happen only at the onset of labour.
2. Flexion
The fetal head flexes chin-on-chest to present its smallest diameter (suboccipitobregmatic, ~9.5 cm) rather than a larger one. This is a passive movement that allows the head to fit through the narrowest part of the pelvis.
3. Descent
The downward movement of the fetal presenting part through the birth canal, driven by uterine contractions, maternal expulsive efforts, and straightening of the fetal body. It is gradual and progressive.
4. Internal Rotation
As the head descends through the ischial spines, it rotates so the occiput moves from its originally transverse position anteriorly toward the pubic symphysis (occiput anterior - the most common and favourable position). Less commonly the occiput rotates posteriorly.
5. Extension
As the flexed head reaches the vaginal introitus, the occiput contacts the inferior margin of the pubic symphysis. The head then extends (unbends), and the occiput, bregma, forehead, nose, mouth, and chin pass in sequence over the perineum. The head is born by this extension movement.
6. External Rotation (Restitution)
Immediately after the head is delivered, it rotates back to the transverse position to realign with the fetal shoulders. This is a passive movement.
7. Expulsion (Delivery of Shoulders and Body)
- Gentle downward traction on the head delivers the anterior shoulder under the pubic arch
- Gentle upward traction delivers the posterior shoulder
- The rest of the body follows rapidly
Roberts & Hedges' Clinical Procedures in Emergency Medicine
Delivery Technique Notes
- The modified Ritgen maneuver is used: a towel-draped hand stretches the perineum and applies gentle pressure to the fetal chin, while the other hand applies pressure to the occiput to guide controlled, slow delivery and prevent perineal tears
- The mother is instructed to pant (not push) as the head crowns, to slow delivery and protect the perineum
- After the head delivers, the clinician checks for and reduces any nuchal cord
- The cord is clamped 10 cm from the abdomen (2 clamps 4-5 cm apart) and cut
- Apgar scores are documented at 1 and 5 minutes
STAGE 3 - Delivery of the Placenta
From delivery of the baby to delivery of the placenta.
Signs of placental separation (occur within 5-10 minutes):
- The uterus becomes firmer and rises in the abdomen
- The umbilical cord lengthens by 5-10 cm
- A sudden gush of blood
Duration: Normally within 5-10 minutes; up to 30 minutes is acceptable. Beyond 30 minutes, risk of postpartum hemorrhage increases up to 6-fold.
Active management of Stage 3 (recommended to reduce PPH):
- Administration of a uterotonic agent (oxytocin, syntometrine)
- Controlled cord traction while applying counterpressure above the pubic symphysis
- Uterine massage after placental delivery
After delivery, the placenta is examined for completeness (3 vessels in cord; intact membranes and cotyledons) to ensure no retained fragments. - Rosen's Emergency Medicine
STAGE 4 - The First Hour After Delivery
Described by Pritchard & MacDonald, this "fourth stage" covers the first hour following placental delivery.
Key activities:
- Monitoring uterine tone (fundal massage to prevent uterine atony - the leading cause of postpartum hemorrhage)
- Monitoring vital signs and blood loss
- Repair of any perineal lacerations or episiotomy
- Skin-to-skin contact and initiation of breastfeeding
- Newborn assessment and Apgar scoring
Summary Table
| Stage | From | To | Duration (Nullipara) | Duration (Multipara) |
|---|---|---|---|---|
| Stage 1 - Latent | Onset of regular contractions | Active phase (~3-4 cm) | Up to 20 hours | Up to 14 hours |
| Stage 1 - Active | ~3-4 cm dilation | 10 cm (complete) | 8-12 hours total Stage 1 | 5-8 hours total Stage 1 |
| Stage 2 | Full dilation (10 cm) | Delivery of baby | 20-50 minutes | Minutes to 20 min |
| Stage 3 | Delivery of baby | Delivery of placenta | < 30 minutes | < 30 minutes |
| Stage 4 | Delivery of placenta | 1 hour postpartum | 1 hour | 1 hour |
Key teaching points:
- True labour contractions are regular, progressive, and cause cervical change - unlike Braxton Hicks which are irregular and do not change the cervix
- A prolonged latent phase (>20h nullipara / >14h multipara) warrants evaluation; causes include excessive sedation, unfavourable cervix, and myometrial dysfunction
- The cardinal movements (engagement → flexion → descent → internal rotation → extension → external rotation → expulsion) describe how the fetus adapts to the bony pelvis
- Active management of Stage 3 significantly reduces postpartum hemorrhage risk
Sources: Creasy & Resnik's Maternal-Fetal Medicine; Rosen's Emergency Medicine; Roberts & Hedges' Clinical Procedures in Emergency Medicine; Morgan & Mikhail's Clinical Anesthesiology, 7e; Tintinalli's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.