Development of pancreas and annular pancreas
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
I now have comprehensive information from multiple authoritative textbooks and all the key images. Let me compile a thorough answer.
Development of the Pancreas and Annular Pancreas
1. Overview
The pancreas develops from posterior foregut endoderm and arises as two distinct outgrowths - a dorsal bud and a ventral bud - that later fuse into a single organ. This process occurs between the 5th and 8th weeks of embryonic life.
2. The Two Pancreatic Buds
Dorsal Pancreatic Bud
- Appears first, slightly cranial to the ventral bud
- Develops within the dorsal mesentery (dorsal mesogastrium)
- Forms the tail, body, and superior portion of the head of the pancreas
- Contains the dorsal duct, which becomes the distal portion of the main pancreatic duct (of Wirsung) and the entire accessory duct (of Santorini)
- Molecular induction: FGF2 and Activin (a TGF-β family member), produced by the notochord and dorsal aortic endothelium, repress SHH expression in the gut endoderm destined to become the dorsal bud, thereby allowing pancreatic specification
Ventral Pancreatic Bud
- Arises as an outgrowth of the hepatic diverticulum, near the entry of the bile duct into the duodenum
- Has a bilobed (bifid) origin - the left ventral bud normally regresses; only the right portion completes rotation
- Grows within the ventral mesentery
- Forms the uncinate process and inferior part of the head
- Contains the ventral duct, which becomes the proximal portion of the main pancreatic duct (of Wirsung)
- Molecular induction: the ventral bud is induced by visceral mesoderm
Both processes lead to upregulation of PDX-1 (Pancreatic and Duodenal Homeobox 1 gene), the master regulator of pancreatic development.
3. Rotation and Fusion (5th-8th weeks)
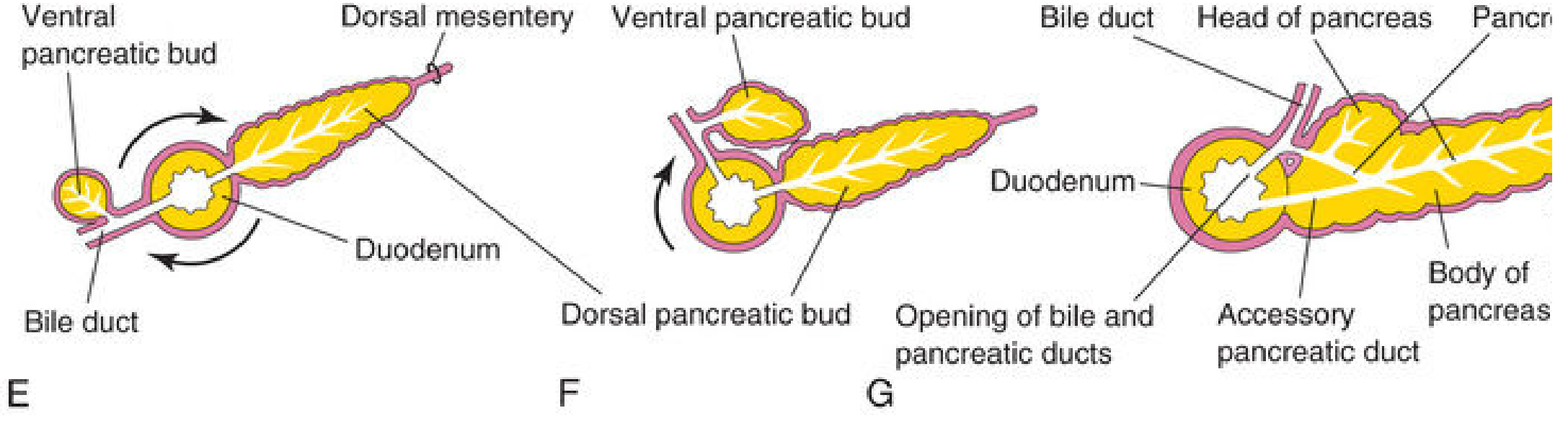
E-G: Rotation of the ventral pancreatic bud (with the bile duct) around the duodenum, followed by fusion with the dorsal bud and formation of the main and accessory pancreatic ducts - The Developing Human, Fig. 11.10
As the duodenum rotates to the right and becomes C-shaped, the ventral pancreatic bud (carried along with the bile duct) swings posteriorly and to the left around days 37-42 of gestation. It comes to lie posterior to the dorsal bud, and the two buds then fuse.
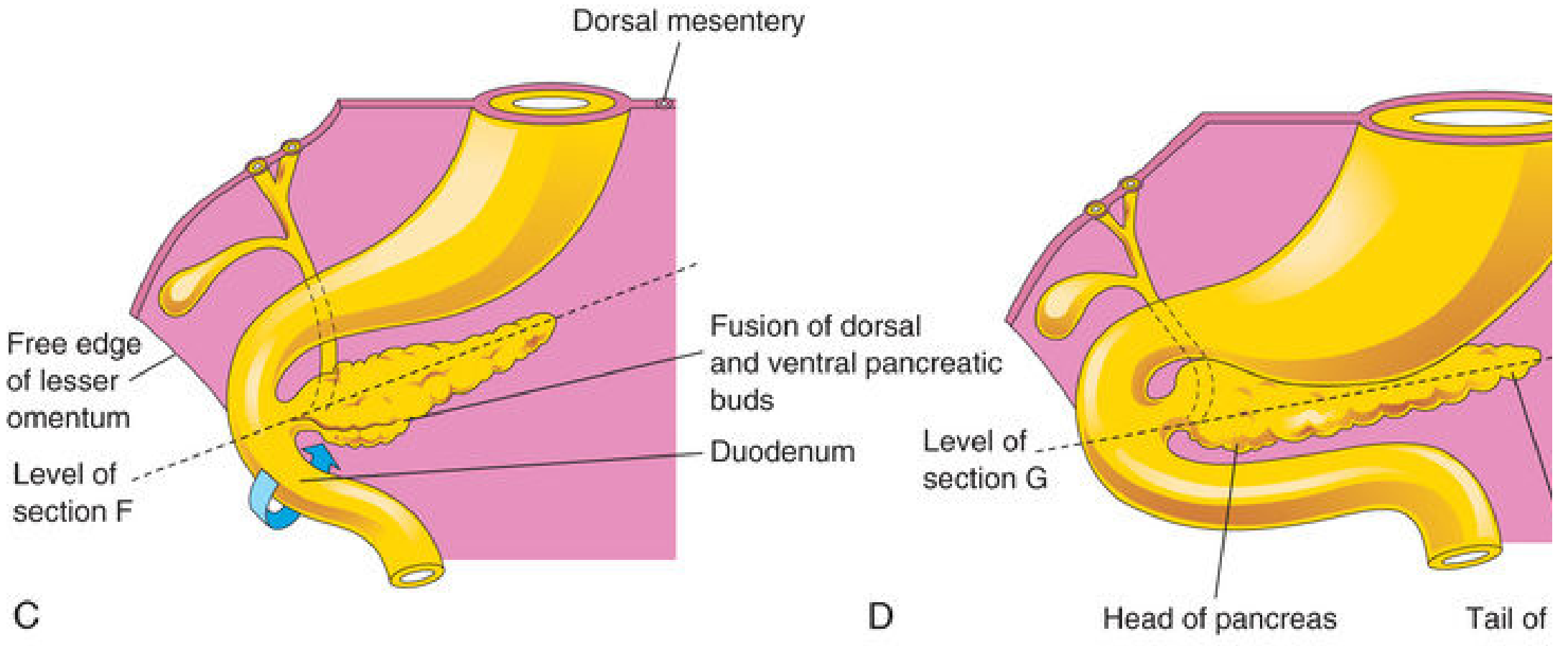
C & D: Fusion complete - the pancreas now lies along the dorsal abdominal wall in retroperitoneal position - The Developing Human, Fig. 11.10
4. Duct System After Fusion
After the buds fuse, their ducts anastomose:
| Duct | Formed From | Opens Into |
|---|---|---|
| Main pancreatic duct (of Wirsung) | Entire ventral duct + distal part of dorsal duct | Major duodenal papilla (with bile duct) |
| Accessory pancreatic duct (of Santorini) | Proximal part of dorsal duct | Minor duodenal papilla (~2 cm cranial to main duct) |
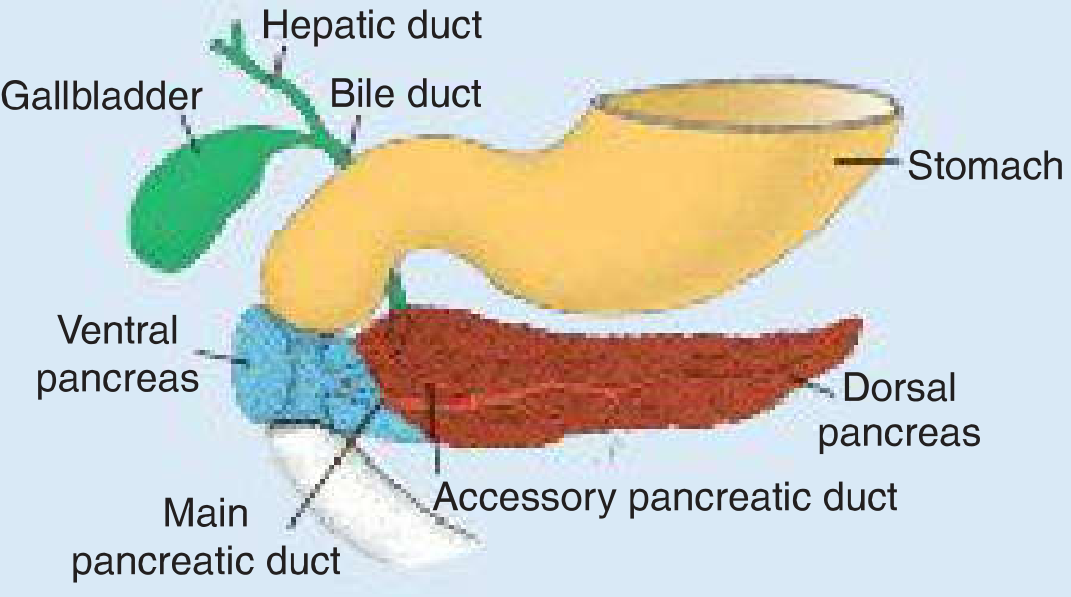
Fusion result: the dorsal pancreas (red) and ventral pancreas (blue) with their duct anatomy - Langman's Medical Embryology
5. Cellular Differentiation
After bud fusion, all three parenchymal cell types - acinar, ductal, and islet cells - differentiate from a common pancreatic progenitor lineage.
- Pancreatic islets of Langerhans develop from parenchymal pancreatic tissue in the 3rd month; insulin secretion begins at ~5th month
- Islet cell specification is controlled by paired homeobox genes:
- PAX4 + PAX6 co-expression → β cells (insulin), δ cells (somatostatin), γ cells (pancreatic polypeptide)
- PAX6 alone → α cells (glucagon)
- Visceral mesoderm surrounding the pancreatic buds forms the pancreatic connective tissue and stroma
Islet Cell Proportions (mature pancreas)
| Cell Type | Proportion | Hormone |
|---|---|---|
| Beta (β) | 50-80% | Insulin, amylin |
| PP / F cells | 10-35% | Pancreatic polypeptide |
| Alpha (α) | 5-20% | Glucagon |
| Delta (δ) | ~5% | Somatostatin |
| Epsilon (ε) | Rare | Ghrelin |
6. Final Position
As the stomach, duodenum, and ventral mesentery rotate, the fused pancreas comes to lie along the dorsal abdominal wall in a retroperitoneal position.
7. Annular Pancreas
Definition
A congenital anomaly in which a thin band of pancreatic tissue forms a ring (annulus) around the descending (second) part of the duodenum, at the preampullary level. Incidence: approximately 1 in 1,000 (imaging studies) to 3 in 20,000 (autopsy studies).
Embryologic Mechanism
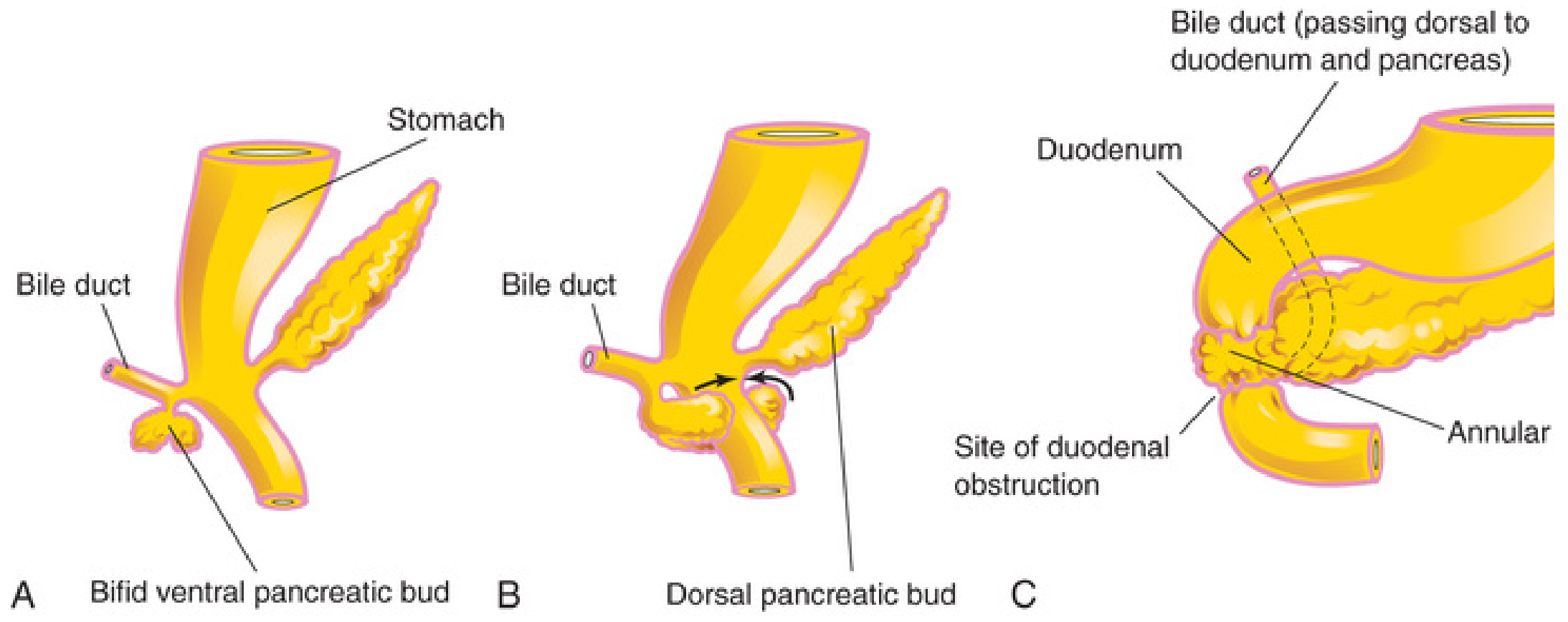
A: Bifid ventral bud. B: The two segments rotate in opposite directions encircling the duodenum. C: Resulting annular pancreas with site of obstruction - The Developing Human, Fig. 11.11
The defect arises by one of two mechanisms:
- The ventral bud splits (becomes bifid) - the right portion migrates normally (posteriorly), but the left portion migrates in the opposite direction (anteriorly). The two segments then encircle the duodenum and fuse with the dorsal bud, forming a ring.
- Failure of the left ventral bud to regress - persistence of the left ventral lobe contributes to annular tissue.
Both result in the same anatomic consequence: pancreatic tissue encircling and potentially compressing the duodenum.
Associations and Genetics
- Trisomy 21 (Down syndrome) - most common association
- Cardiac defects
- Intestinal malrotation
- Duodenal atresia
- Genitourinary anomalies
- Tracheoesophageal fistula
- Females affected more frequently than males
- Familial cases reported (siblings, identical twins); microduplication on chromosome 6q24.2 (utrophin gene) identified in familial cases
- Shh and Ihh gene defects show 42-85% incidence of annular pancreas in mouse models
Clinical Presentation
Two peaks of presentation:
| Age Group | Symptoms |
|---|---|
| Neonates / Infants | Non-bilious vomiting, feeding intolerance, failure to thrive; complete or partial duodenal obstruction |
| Adults (4th-7th decades) | Abdominal pain, pancreatitis, biliary obstruction, nausea, vomiting, bloating |
- Prenatal: duodenal obstruction prevents the fetus from swallowing amniotic fluid → polyhydramnios; may be detected on prenatal ultrasound
- Inflammation (pancreatitis) in the annular tissue can worsen or precipitate obstruction
Investigations
- Children: abdominal X-ray (classic "double bubble" sign), ultrasound, upper GI series
- Adults: CT scan, MRCP, or ERCP; diagnosis sometimes made at laparotomy
- Classic radiological sign: mid-duodenal stricture with proximal dilatation on barium contrast upper GI series
Treatment
- Duodenoduodenostomy - surgical bypass of the obstructed segment; treatment of choice in children and many adults
- The annular tissue must never be divided (contains functional pancreatic tissue and the pancreatic duct may run through the annulus)
- Complex pancreatic surgery may be required in adults
- Long-term risks: increased risk of acute/recurrent pancreatitis and pancreaticobiliary neoplasia (including duodenal carcinoma); ongoing surveillance recommended
8. Other Developmental Anomalies of the Pancreas
| Anomaly | Mechanism | Clinical Significance |
|---|---|---|
| Pancreas divisum | Failure of dorsal and ventral duct systems to fuse (up to 10% of population) | Accessory duct becomes main conduit; possible recurrent pancreatitis |
| Ectopic pancreatic tissue | Separate nests of pancreatic tissue | Found in gastric mucosa, proximal duodenum, jejunum, pyloric antrum, Meckel's diverticulum; usually asymptomatic |
| Pancreatic agenesis | Failure of bud formation; PDX-1 mutations | Rare; associated with neonatal diabetes |
Sources:
- The Developing Human: Clinically Oriented Embryology (Moore et al.), Ch. 11 - pancreatic buds and annular pancreas
- Langman's Medical Embryology, Ch. 15 - molecular regulation, PAX4/PAX6 signaling, annular pancreas mechanism
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, Ch. 55 - embryonic/fetal development, islet cell proportions, annular pancreas clinical details
- Gray's Anatomy for Students, Ch. 4 - bifid ventral bud mechanism, polyhydramnios
This is a shared conversation. Sign in to Orris to start your own chat.