Diagnosis of Bronchogenic Carcinoma
Reading File
Finding Sources
Searching PubMed
"bronchogenic carcinoma" AND diagnosis
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I have enough rich content from multiple authoritative sources. Let me now compose the comprehensive answer.
Diagnosis of Bronchogenic Carcinoma
Bronchogenic carcinoma (lung cancer) is the leading cause of cancer-related death worldwide. Diagnosis requires a coordinated approach: clinical evaluation, imaging, tissue sampling, histopathologic subtyping, molecular testing, and formal staging. The dual goals are (1) histopathologic diagnosis with molecular characterization, and (2) accurate staging to guide therapy - accomplished in the safest, least invasive manner possible.
1. Clinical Evaluation
History
More than 75% of patients are symptomatic at initial diagnosis because most present at an advanced stage. Symptoms fall into three categories:
| Category | Symptoms |
|---|---|
| Primary (local) | Cough, hemoptysis, dyspnea, wheezing, post-obstructive pneumonia |
| Regional extension | Chest pain, hoarseness (recurrent laryngeal nerve), SVC syndrome, dysphagia, Horner syndrome, Pancoast syndrome (shoulder/arm pain, C8-T2 distribution) |
| Systemic / Metastatic | Weight loss, anorexia, bone pain, focal neurological deficits, headache (brain metastases) |
Paraneoplastic Syndromes (suggest specific cell types):
- SIADH (inappropriate ADH) - small cell lung cancer (SCLC)
- Ectopic ACTH / Cushing syndrome - SCLC
- Hypercalcemia (PTHrP) - squamous cell carcinoma
- Hypertrophic pulmonary osteoarthropathy - adenocarcinoma
- Lambert-Eaton myasthenic syndrome - SCLC
Physical Examination: Supraclavicular/cervical lymphadenopathy (accessible for biopsy), signs of pleural effusion, SVC syndrome, Horner syndrome, clubbing, hepatomegaly.
Functional Assessment: Comorbid conditions are catalogued - limited cardiopulmonary reserve may preclude surgical resection and affects therapy planning.
2. Initial Imaging
Chest X-Ray (CXR)
Usually the first investigation. Findings that raise suspicion:
- Hilar mass or enlargement
- Peripheral pulmonary nodule or mass
- Unilateral pleural effusion
- Mediastinal widening
- Collapse/consolidation (post-obstructive)
- Elevated hemidiaphragm (phrenic nerve palsy)
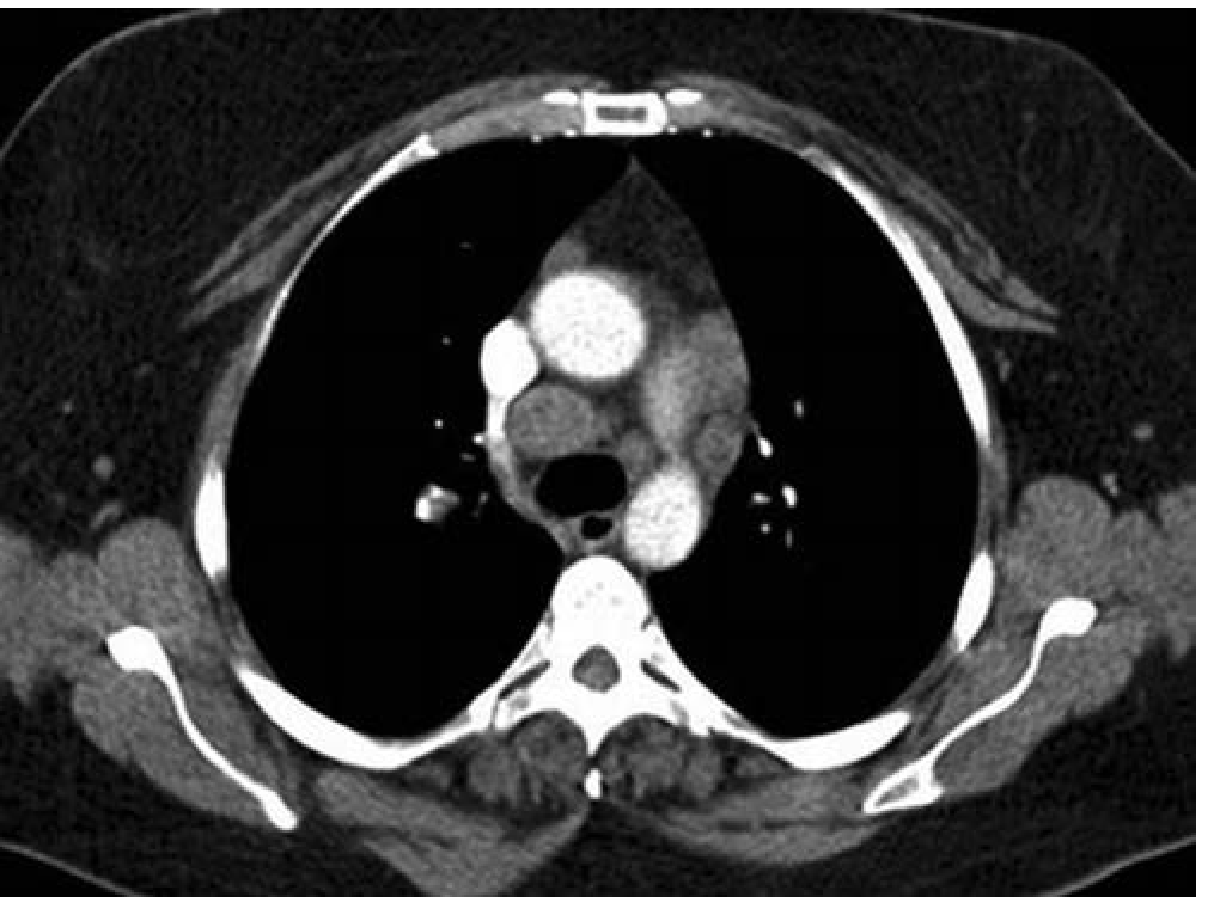
Chest CT Scan (with IV contrast)
Mandatory in all patients unless no treatment is planned. The scan covers the chest and upper abdomen, including the liver and adrenal glands in entirety. Contrast helps differentiate lymph nodes from vessels and characterizes hepatic/adrenal lesions.
CT defines:
- Primary tumor: size, location, satellite nodules, atelectasis, invasion of adjacent structures (T stage)
- Lymph node status: nodes >1 cm short-axis diameter are considered pathologically enlarged - 62% of nodes 10-15 mm are malignant, 90% of nodes >15 mm are malignant; however, CT alone has pooled sensitivity of only 51% and specificity of 86% for mediastinal nodal metastases
- Extrathoracic disease: pleural effusion, pericardial effusion, pleural nodules, adrenal lesions (found in 4-18% but up to 50% are benign)
3. Advanced Imaging
PET-CT (18-FDG)
PET has a prominent role in the initial noninvasive evaluation:
- Sensitivity 96%, specificity ~85% for malignancy
- More sensitive and specific than CT for mediastinal lymph node assessment (pooled sensitivity 74%, specificity 85%)
- In patients with enlarged mediastinal nodes: sensitivity up to 100%, specificity 78%
- False positives occur with inflammatory processes (infections, sarcoid, vasculitis, recent surgery, immunotherapy reaction)
- False negatives occur with low-grade malignancies, small lesions (<0.8-1.0 cm), and hyperglycemia
- Approximately 20% of patients with normal mediastinal nodes on both CT and PET will still have occult malignant mediastinal disease
MRI Brain
Recommended for patients with neurological symptoms or when staging requires brain metastasis evaluation. MRI is superior to CT for brain metastases. SCLC and adenocarcinoma have the highest rates of brain metastases.
Bone Scan / Skeletal Survey
Indicated when bone metastases are suspected (bone pain, elevated alkaline phosphatase).
4. Tissue Diagnosis - Biopsy Techniques
Tissue is required for:
- Histopathologic classification (NSCLC vs. SCLC; subtyping within NSCLC)
- Immunohistochemistry (IHC) markers
- Molecular/genomic testing for actionable mutations
- PD-L1 expression for immunotherapy eligibility
The least invasive procedure that can provide adequate tissue should be chosen first.
Bronchoscopy
- Flexible bronchoscopy: preferred for central, endobronchial lesions; allows direct visualization, biopsy, brushings, and bronchoalveolar lavage (BAL)
- Endobronchial Ultrasound (EBUS) with Transbronchial Needle Aspiration (TBNA): the current standard for mediastinal and hilar lymph node sampling; can reach stations 2R, 2L, 4R, 4L, 7, 10, 11, and 12
- Navigational bronchoscopy (electromagnetic or radial EBUS): extends reach to peripheral lesions
CT-Guided Transthoracic Needle Aspiration/Biopsy (TTNA/TTNB)
- Best for peripheral lesions not reachable by bronchoscopy
- High sensitivity (~90%) for peripheral nodules
- Risk of pneumothorax (~20-25%)
Endoscopic Ultrasound (EUS/EUS-FNA)
- Complements EBUS, particularly for stations 5, 7, 8, and 9 (posterior and inferior mediastinum)
- Combined EBUS + EUS gives the highest diagnostic yield for mediastinal staging
Surgical Biopsy
- Mediastinoscopy: gold standard for mediastinal staging; accesses stations 2R/L, 4R/L, 7
- Video-Assisted Thoracoscopic Surgery (VATS): for pleural effusion/nodules, parenchymal lesions, or accessible lymph nodes not reachable by less invasive methods
- Anterior mediastinotomy (Chamberlain procedure): for stations 5 and 6 (aortopulmonary window, para-aortic)
Other Sites
- Supraclavicular / scalene lymph node biopsy: if palpable nodes present
- Pleural fluid cytology: for effusions (with repeat thoracentesis if initial cytology is negative)
- Bone marrow biopsy: in SCLC with suspected marrow involvement
5. Histopathologic Classification (WHO 2015/2021)
Non-Small Cell Lung Cancer (NSCLC) - ~87% of all cases
| Subtype | Key Features | IHC Markers |
|---|---|---|
| Adenocarcinoma (~40%) | Peripheral location; acinar, papillary, micropapillary, lepidic, or solid patterns | TTF-1+, Napsin A+, CK7+ |
| Squamous Cell Carcinoma (~25-30%) | Central, endobronchial; keratinization, intercellular bridges | p40+, p63+, CK5/6+, TTF-1- |
| Large Cell Carcinoma (~10%) | Diagnosis of exclusion; no squamous or glandular differentiation | Variable |
| Adenosquamous (<5%) | Mixed features | Mixed markers |
Small Cell Lung Cancer (SCLC) - ~13%
- Central location, rapid doubling time
- Neuroendocrine features: synaptophysin+, chromogranin A+, CD56+, TTF-1+ (diffuse)
- Ki-67 very high (>70-90%)
- Almost universally associated with smoking
Carcinoid Tumors (typical and atypical) and large cell neuroendocrine carcinoma (LCNEC) are also classified under the neuroendocrine spectrum.
6. Molecular / Biomarker Testing
In NSCLC (especially adenocarcinoma), molecular profiling is mandatory before treatment decisions:
| Biomarker | Prevalence | Targeted Drug |
|---|---|---|
| EGFR mutations (exon 19 del, exon 21 L858R) | 10-15% Western; 30-50% Asian | Osimertinib, Erlotinib, Gefitinib |
| ALK rearrangement | 3-7% | Alectinib, Crizotinib |
| ROS1 rearrangement | 1-2% | Crizotinib, Entrectinib |
| KRAS G12C | ~13% | Sotorasib, Adagrasib |
| BRAF V600E | 1-3% | Dabrafenib + Trametinib |
| MET exon 14 skipping | 3-4% | Tepotinib, Capmatinib |
| RET fusion | 1-2% | Selpercatinib |
| NTRK fusion | <1% | Larotrectinib |
| PD-L1 expression | Variable | Pembrolizumab (if ≥50%) |
Liquid biopsy (circulating tumor DNA) can be used when tissue is insufficient.
7. TNM Staging (IASLC 8th Edition)
Staging is the other core diagnostic goal. Clinical stage (cTNM) is established before treatment; pathologic stage (pTNM) only after resection.
T (Primary Tumor)
- T1a: ≤1 cm; T1b: >1-2 cm; T1c: >2-3 cm
- T2: >3-5 cm, or invades visceral pleura/main bronchus/causes atelectasis to hilum
- T3: >5-7 cm, or invades chest wall/pericardium/phrenic nerve, or separate nodule in same lobe
- T4: >7 cm, or invades mediastinum/heart/great vessels/carina/spine, or nodule in different ipsilateral lobe
N (Regional Lymph Nodes)
- N0: none; N1: ipsilateral pulmonary/hilar; N2: ipsilateral mediastinal/subcarinal; N3: contralateral mediastinal/hilar or supraclavicular
M (Distant Metastasis)
- M0: none; M1a: contralateral lung nodule, pleural/pericardial effusion or nodules; M1b: single extrathoracic metastasis; M1c: multiple extrathoracic metastases (one or more organs)
Stage Groups:
- Stage I: T1-T2a, N0 (surgically resectable)
- Stage II: T1-T3, N1 or T3 N0 (surgical ± adjuvant)
- Stage III: N2-N3 or T4 (multimodality)
- Stage IV: M1 (systemic therapy)
SCLC Staging
A simpler two-stage system is used:
- Limited stage: confined to ipsilateral hemithorax and regional nodes within a single tolerable radiation port (broadly TNM stages I-III) - chemoradiation with curative intent
- Extensive stage: beyond one radiation port, contralateral nodal involvement, malignant effusions, or distant metastases (60-65% of SCLC) - chemotherapy ± palliative radiation
8. Radiographic Staging Groups for Mediastinal Evaluation
A practical classification guides the approach to invasive mediastinal staging:
| Group | Description | Action |
|---|---|---|
| A | Suspected metastatic disease (M1) | Sample most accessible/distant metastatic site |
| B | Discrete mediastinal lymph node enlargement | Invasive mediastinal staging mandatory (up to 40% of enlarged nodes are benign) |
| C | Central lesion/N1 disease, normal-sized mediastinal nodes | Invasive staging needed (20-25% have occult N2 disease) |
| D | Peripheral stage I, normal mediastinal and hilar nodes | Invasive mediastinal staging not required (low pretest probability) |
9. Laboratory Investigations
Routine bloods in the workup:
- CBC (anaemia, thrombocytopenia suggest marrow involvement)
- LFTs, ALP (hepatic or bony metastases)
- Serum calcium (hypercalcaemia in squamous cell carcinoma)
- Serum sodium (hyponatraemia in SIADH/SCLC)
- Renal function (contrast for imaging, nephrotoxic chemotherapy)
- LDH (prognosis in SCLC)
Sputum cytology has low sensitivity (30-60%) and is generally reserved for centrally located tumors with hemoptysis when bronchoscopy is not feasible.
10. Summary Diagnostic Algorithm
Suspected Lung Cancer (CXR abnormality / symptoms)
↓
Chest CT (chest + upper abdomen, IV contrast)
↓
PET-CT (metabolic staging, exclude occult metastases)
↓
Determine radiographic staging group (A, B, C, D)
↓
Tissue Biopsy (least invasive approach first):
- Peripheral: CT-guided TTNB
- Central/endobronchial: Bronchoscopy
- Mediastinal nodes (Groups B & C): EBUS-TBNA ± EUS
- If above fail: Mediastinoscopy / VATS
↓
Histopathology + IHC subtyping
↓
Molecular profiling (NSCLC): EGFR, ALK, ROS1, KRAS, BRAF,
MET, RET, NTRK, PD-L1
↓
Clinical TNM Stage assignment → Treatment planning
Key Points
- Over 75% of patients present at locally advanced or metastatic stage; only ~25% have early-stage disease at diagnosis
- CT alone is insufficient for mediastinal staging (sensitivity only 51%); PET-CT and EBUS are required
- Clinical and pathologic TNM stages disagree in ~48% of NSCLC cases, with most patients being clinically understaged
- Histologic subtyping and molecular profiling are now inseparable from diagnosis - targeted therapy depends entirely on them
- SCLC is staged using the limited/extensive two-stage system, though TNM applies and carries prognostic value
Sources: Fishman's Pulmonary Diseases and Disorders, 2-Volume Set (Chapter 116: Clinical Evaluation, Diagnosis, and Staging of Lung Cancer); Murray & Nadel's Textbook of Respiratory Medicine (Chapter 76: Lung Cancer - Diagnosis and Staging)
This is a shared conversation. Sign in to Orris to start your own chat.