Trabeculectomy
Reading File
Finding Sources
Finding Sources
Searching PubMed
trabeculectomy glaucoma outcomes
Reading File
Reading File
Reading File
Reading File
Loading Image
I have all the content needed. Here is the comprehensive response.
Trabeculectomy
Definition and Principle
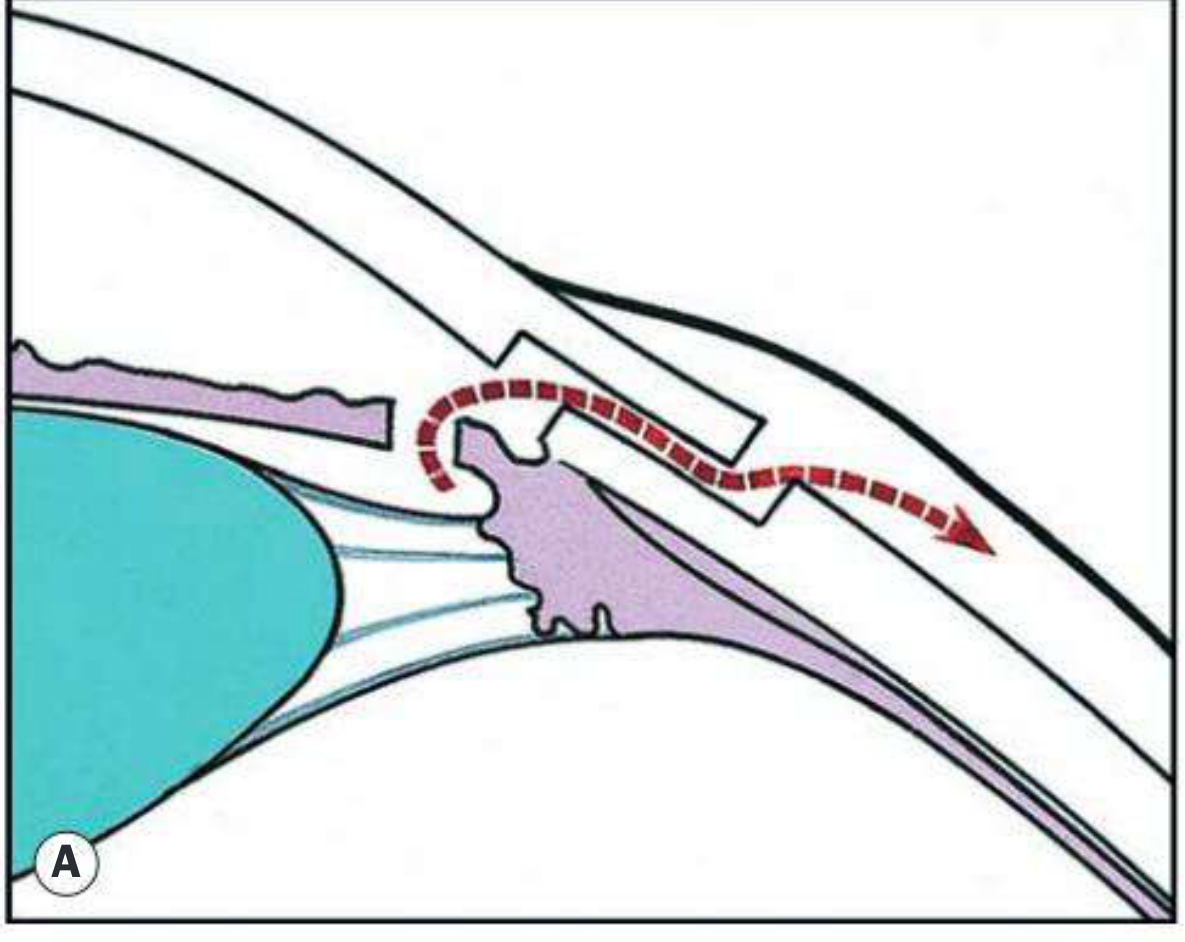
Trabeculectomy is the gold-standard glaucoma filtration surgery that lowers intraocular pressure (IOP) by creating a protected fistula between the anterior chamber and the sub-Tenon space, allowing aqueous humor to bypass the blocked trabecular meshwork and drain beneath the conjunctiva (forming a filtering bleb).
Indications
- Failure of conservative therapy - inadequate IOP control despite maximal medical therapy
- Progressive deterioration despite seemingly adequate IOP control (including non-adherence)
- Primary therapy - advanced disease requiring very low target pressure; early surgery may be superior in younger patients
- Patient preference - desire to be free of chronic topical medication
Surgical Technique (Classical Procedure)
All steps are performed under local or general anaesthesia at the 12 o'clock position (minimises bleb dysaesthesia):
| Step | Action |
|---|---|
| 1 | Pupil constricted preoperatively (pilocarpine 2%) |
| 2 | Bridle suture inserted (superior cornea or superior rectus) |
| 3 | Limbal or fornix-based conjunctival/Tenon flap fashioned superiorly |
| 4 | Episcleral tissue cleared; major vessels cauterised |
| 5 | Lamellar scleral "trapdoor" flap cut to ~50% depth (3×3-4 mm rectangular, trapezoidal, or triangular) |
| 6 | Superficial flap dissected forward to clear cornea |
| 7 | Paracentesis made in temporal peripheral clear cornea |
| 8 | Anterior chamber entered along the width of the trapdoor base |
| 9 | Deep scleral block excised with a punch (e.g. Kelly punch) |
| 10 | Peripheral iridectomy created to prevent iris prolapse into the sclerostomy |
| 11 | Superficial scleral flap sutured (releasable/lysable sutures) |
| 12 | Balanced salt solution injected through paracentesis to test fistula patency |
| 13 | Conjunctiva/Tenon flap sutured watertight |
| 14 | Atropine 1% drop instilled; subconjunctival steroid + antibiotic injected inferiorly |
Ex-PRESS Mini-Shunt (Modification)
A valveless, titanium, MRI-compatible stent inserted under the scleral flap (replacing the punch sclerostomy). No peripheral iridectomy needed. Offers lower rates of hypotony and hyphaema versus standard trabeculectomy, with equivalent IOP control. Not suitable for primary angle-closure glaucoma without concurrent cataract surgery.
Adjunctive Antimetabolites
Used to inhibit subconjunctival fibrosis and improve bleb survival:
- Mitomycin C (MMC) - more potent; applied intraoperatively as a soaked sponge to the episcleral tissue; preferred in high-risk eyes (aphakia, previous surgery, young patients, uveitic or neovascular glaucoma)
- 5-Fluorouracil (5-FU) - applied intraoperatively or as repeated subconjunctival postoperative injections
Both agents significantly improve long-term IOP control but increase the risk of thin, avascular blebs, hypotony, and bleb-related infections.
Postoperative Management
- Topical steroids (4x/day for 2 weeks, then tapered over 8-12 further weeks) to suppress healing and maintain bleb patency
- Topical antibiotics for 2 weeks
- Suture manipulation: Releasable sutures can be removed, or laser suture lysis (LSL) of buried flap sutures performed postoperatively to titrate IOP - a low bleb with raised IOP suggests tight sutures
- Bleb massage can be used to increase filtration
The Filtering Bleb
A functioning bleb should be:
- Slightly elevated
- Relatively avascular
- Show superficial microcysts (distended conjunctival goblet cells - a positive sign of good function)
A cystic, thin-walled bleb is not uncommon with antimetabolite use.
Complications
Early Complications
| Complication | Notes |
|---|---|
| Hypotony | IOP < 5 mmHg; from over-drainage, wound leak, or choroidal detachment |
| Hyphaema | Blood in anterior chamber from iris/ciliary body trauma |
| Bleb leak | Positive Seidel test (aqueous dilutes fluorescein); risk increased with antimetabolites |
| Shallow/flat anterior chamber | From hypotony; classified into 3 grades |
| Choroidal detachment | Separation of choroid from sclera due to low IOP; managed conservatively unless severe |
Late Complications
| Complication | Notes |
|---|---|
| Bleb failure / fibrosis | Most common cause of late failure; Tenon cyst formation |
| Bleb-related infection / Blebitis | Particularly with thin avascular blebs and antimetabolite use; can progress to endophthalmitis |
| Cataract | Accelerated nuclear sclerosis following surgery |
| Hypotony maculopathy | Chronic low IOP causing chorioretinal folds and reduced vision |
| Diplopia | Restrictive strabismus from fibrosis or damage to extraocular muscle |
Malignant Glaucoma (Aqueous Misdirection)
A rare but serious complication - particularly after angle-closure glaucoma surgery. Caused by anterior rotation of ciliary processes and iris root (ciliolenticular block) with posterior misdirection of aqueous.
- Signs: Shallow AC with myopic shift, high IOP, absent bleb, negative Seidel test
- Treatment:
- Mydriatics (atropine 1% + phenylephrine 10%) - first line
- IV mannitol if mydriatics fail
- Nd:YAG laser through the iridectomy to disrupt anterior hyaloid
- Pars plana vitrectomy as last resort
Failure of Filtration and Salvage Options
When a bleb fails (flat, vascularised, encapsulated "Tenon cyst"):
- 5-FU subconjunctival injections - stimulate bleb survival
- Needling - mechanical disruption of encapsulating fibrosis under the bleb (with MMC)
- Glaucoma drainage devices (GDD) - tube-shunt if trabeculectomy fails; the landmark Tube versus Trabeculectomy (TVT) Study showed GDD safety is comparable to trabeculectomy with MMC
- Cyclodiode laser (cyclodestruction) - if all other options fail
Trabeculectomy vs. Glaucoma Drainage Devices
Circumstances where GDD may be superior to trabeculectomy include:
- Prior conjunctival scarring (previous failed trabeculectomy, vitreoretinal surgery)
- Uveitic or neovascular glaucoma
- Aphakic glaucoma
- The TVT study found GDD had slightly better IOP control at 5 years in previously operated eyes
Recent Evidence
Recent meta-analyses (2024-2026) are relevant:
- A 2025 systematic review (PMID 39394492) comparing PreserFlo MicroShunt vs. trabeculectomy found comparable IOP reduction, with the MicroShunt having a better safety profile
- A 2025 meta-analysis (PMID 40404077) found that anti-VEGF augmentation of trabeculectomy improves surgical success rates by reducing subconjunctival fibrosis
- A 2025 review on MIGS (PMID 39670502) contextualises trabeculectomy as still the reference standard against which minimally invasive procedures are compared, though MIGS devices are increasingly used in mild-moderate glaucoma
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed., pp. 431-435; The Wills Eye Manual, p. 559
This is a shared conversation. Sign in to Orris to start your own chat.